


Background
Dementia currently affects around 50 million people worldwide, and there are approximately 10 million new cases of dementia annually (World Health Organization, 2020). “Dementia” is an umbrella term encompassing any disorder which causes significant cognitive decline, leading to impairments in previous levels of functioning, including memory loss and the inability to perform daily tasks (Gale, Acar, & Daffner, Reference Gale, Acar and Daffner2018). In Canada, dementia affects an estimated 7.1 per cent of the senior population across the country (Government of Canada, 2017). Importantly, this statistic is accompanied by an increase in the prevalence of the disease, which doubles every 5 years among seniors (Government of Canada, 2017). This increase is attributable to an aging population, and therefore a growing senior population in Canada may present with a greater number of older adults impacted by dementia (Canadian Institute for Health Information, n.d.). Given the growing burden of disease, the topic of dementia as it pertains to the well-being and quality of life (and death) of Canadian seniors becomes all the more pertinent. As there is currently no cure for the disease, and an often rapid mental, physical, and social decline leaves limited time for planning, it is important to understand the wishes of older adults while they are cognitively able to participate in those conversations.
Advance Care Planning (ACP)
ACP is a proactive step that can be taken to prepare for the health complications which may accompany aging, and especially dementia. ACP is a process that allows a patient to have discussions with their health care provider (HCP) and/or family/friends regarding presumptive future health care plans in the face of potential diagnoses, cognitive decline, or health circumstances (deLima Thomas et al., Reference deLima Thomas, Sanchez-Reilly, Bernacki, O’Neill, Morrison and Kapo2018). ACP is an interactive process, aimed at ensuring that decisions made in the future are in line with a patient’s prerogatives, should the patient find themself in a state in which they are unable to express their wishes, as is the case with dementia (Speak Up Canada, 2020).
Recent literature has investigated the various clinical barriers that exist and can impede completion of ACP. A systematic review conducted in 2019 found that the most common barriers to ACP were insufficient education and time to discuss or complete ACP processes (Blackwood, Walker, Mythen, Taylor, & Vindrola‐Padros, Reference Blackwood, Walker, Mythen, Taylor and Vindrola‐Padros2019). Logistical factors, such as busy clinics, can present challenges to having thorough discussions about ACP and its elements. Successful completion of ACP also necessitates extensive training of HCPs, such that they can effectively hold relevant conversations and implement these plans (Blackwood et al., Reference Blackwood, Walker, Mythen, Taylor and Vindrola‐Padros2019). In a 2015 study, HCPs expressed that forming a strong rapport with patients and their families offered them more opportunities to have productive conversations in a timely manner as well as to understand the nature of the decisions being made (Brazil, Carter, Galway, Watson, & van der Steen, Reference Brazil, Carter, Galway, Watson and van der Steen2015). Furthermore, the ACP process and the implementation of plans required support from a myriad of parties, both at the patient and system levels (Blackwood et al., Reference Blackwood, Walker, Mythen, Taylor and Vindrola‐Padros2019). Patient-level aspects of ACP were particularly notable. During ACP, a patient would express their concerns, values, and goals for the care which they desire to be upheld in the future (Porteri, Reference Porteri2018). Uncertainty regarding the trajectory of the illness, potentially ensuring that a suitable surrogate was chosen, and making decisions that were aligned with the cultural beliefs of the patient, were all dilemmas that could arise in the context of ACP, particularly for cognitively impaired patients (deLima Thomas et al., Reference deLima Thomas, Sanchez-Reilly, Bernacki, O’Neill, Morrison and Kapo2018).
ACP is commonly recommended for persons living with dementia, yet increasing age and an uncertain disease trajectory contribute a layer of complexity to this process. It is widely recognized that the neurological decline associated with the disease, coupled with precarious disease trajectories, poses a threat to the autonomy of the patient (Barbas & Wilde, Reference Barbas and Wilde2001). A systematic review investigating ACP for people with dementia found that an early start to the process was imperative, in that it permitted the person living with dementia to be involved in decision making (Tilburgs et al., Reference Tilburgs, Vernooij-Dassen, Koopmans, van Gennip, Engels and Perry2018a). To this end, the review found that uncertainty regarding disease prognosis was the most common barrier that cognitively impaired patients experienced in trying to access ACP. To ameliorate this challenge, the authors suggested that HCPs follow up with patients and their families while providing comprehensive knowledge about the situation and advocating for a timely start to the overall ACP process.
Patient Involvement
The practice of having persons living with dementia participate in ACP has been gaining traction in the literature. A 2019 study conducted in the United States found that meaningful ACP tools and interventions could enable persons with dementia to articulate their end-of-life preferences coherently (Song et al., Reference Song, Ward, Hepburn, Paul, Kim and Shah2019). Another study assessed the factors which impacted ACP and end-of-life decision-making preferences among persons living with dementia and their caregivers, as well as how race might affect these variables (Pettigrew et al., Reference Pettigrew, Brichko, Black, O’Connor, Austrom and Robinson2020). Despite respondents being knowledgeable regarding dementia and hospice care – as well as demonstrating high engagement in ACP – there were racial differences. Black persons living with dementia had lower ACP completion and demonstrated less dementia knowledge than their White counterparts. Furthermore, a Belgian literature review sought to develop evidence-based clinical recommendations for the practical application of ACP in dementia care by professionals in varied settings (Piers et al., Reference Piers, Albers, Gilissen, De Lepeleire, Steyaert and Van Mechelen2018). Whereas it was found that no high-quality guidelines for ACP in dementia care were presently available, emphasis was placed on adequately educating HCPs to initiate and effectively perform all aspects of ACP. Similarly, cognizant of the practical limitations of form-based ACP procedures, other authors have explored alternative means of documenting care preferences and engaging stakeholders in ACP (Chan, Reference Chan2020; Molloy et al., Reference Molloy, Guyatt, Russo, Goeree, O’Brien and Bédard2000). Changes from written to multimedia formats (such as video or audio recording) were not without their legal challenges, however (Chan, Reference Chan2020).
Despite the availability of international studies on ACP for persons living with dementia, there is a paucity of Canadian literature investigating this topic. The current Canadian literature on ACP only offers a cursory overview of the basic attitudes and understandings that Canadians hold about ACP. An online opinion poll administered to elicit perspectives from the public concluded that Canadians had ACP discussions with family members rather than with HCPs; however, only a few respondents completed formal ACP documentation, opting instead for a substitute decision maker (Teixeira et al., Reference Teixeira, Hanvey, Tayler, Barwich, Baxter and Heyland2015). Likewise, a study by Howard et al. (Reference Howard, Bernard, Klein, Tan, Slaven and Barwich2018) yielded similar results, revealing that many Canadians participated in certain ACP activities, yet few had ACP discussions with their family physicians. Despite these findings on ACP engagement, Heyland et al. (Reference Heyland, Heyland, Dodek, You, Sinuff and Hiebert2015) observed that many individuals’ values included being comfortable, minimizing suffering, spending time with family, not being connected to machines, and not prolonging death. Given the increasing prevalence of dementia and the importance of person-centred health care, a review of the Canadian literature is necessary to understand ACP for seniors (≥ 65 years of age) living with dementia in a Canadian context, as well as to identify and fill the gaps in existing knowledge.
Objectives
The primary objectives of this scoping review were to assess the feasibility and acceptability of ACP for Canadian seniors (≥ 65 years of age) diagnosed with dementia. The secondary objectives were to offer recommendations for practice, policy, and research, such that ACP may become more widely recognized as an important aspect of accessible and equitable high-quality (hospice palliative) care for persons living with dementia. Finally, we sought to determine knowledge gaps in order to formulate recommendations for improvement alongside future areas of investigation.
Methods
To answer the question “What is the feasibility and acceptability of advance care planning for older adults (≥65 years of age) diagnosed with dementia in Canada?”, a scoping review of the Canadian literature was conducted following Arksey and O’Malley’s (Reference Arksey and O’Malley2005) five-step framework. A scoping review was chosen given that this study design enables researchers to describe available literature in a field by mapping key concepts. In so doing, scoping reviews can identify research gaps in the current literature as well as summarize and disseminate information for diverse audiences, including professionals, policy makers, and lay persons. This methodology consists of five key procedures: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, synthesizing, and presenting the results (Arksey & O’Malley, Reference Arksey and O’Malley2005).
Initial Review
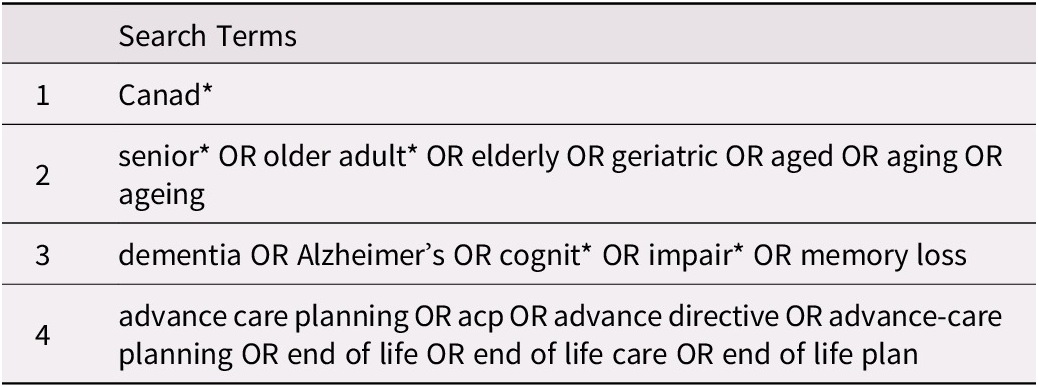
We reviewed electronic databases in the health and social sciences. AgeLine, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, MEDLINE®, Proquest, PsycInfo, and Sociological Abstracts online databases were searched systematically, and Google (Scholar) was hand searched for relevant (grey) literature articles. Seniors and older adults were defined as individuals 65 years of age and older. The search strategy was developed in collaboration with a librarian from the University of Toronto. Search terms were related to “Canadians”, “older adults”, “advance care planning”, and “dementia” as listed in Table 1. Articles generated from database and hand searching were de-duplicated and initially reviewed by title and abstract by independent reviewers (B.K.A., A.K., M.K., S.M.). Articles were deemed suitable for full-text review if they: (1) examined ACP or components of ACP for older adults living with dementia or a similar cognitive impairment, (2) reported on a Canadian study population or context, (3) were published in English between the time period of 1 January 2000 and 31 December 2019, and (4) were available electronically in full text, without cost, through the University of Toronto Library System.
Table 1. Search terms
Results
Database and hand searching yielded 6,645 studies, of which 29 were deemed acceptable for synthesis following the two-step review process described (Figure 1). Of these, 25 (86%) were original research articles. The remaining four articles (14%) consisted of two case studies and two policy-related articles. Two pieces of grey literature were included overall (7%). A summary of study characteristics and findings can be found in Table 2. Articles were grouped according to the following five key themes, based on a thematic content analysis (Anderson, Reference Anderson2007):
-
1. Feasibility of patient engagement in ACP
-
2. Opinions regarding medical assistance in dying (MAiD) for incompetent patients
-
3. Knowledge translation (KT) to support persons living with dementia, professionals, and caregivers
-
4. Barriers to and facilitators of the delivery of holistic dementia care
-
5. Indigenous health considerations.

Figure 1. Flow diagram of study results
Table 2. Study characteristics

* This study also reports on results from The Netherlands and Italy, however only Canadian findings are presented here.
Feasibility of Patient Engagement in ACP
A total of 12 of the 29 sources (41%) discussed the extent to which Canadian seniors and their caregivers engaged in ACP in the event of decisional incapacity (Bravo, Dubois, & Pâquet, Reference Bravo, Dubois and Pâquet2003; Bravo et al., Reference Bravo, Dubois, Cohen, Wildeman, Graham, Painter and Bellemare2011; Bravo, Sene, & Arcand, Reference Bravo, Sene and Arcand2017; Brink, Smith, & Kitson, Reference Brink, Smith and Kitson2008; Cramer, Tuokko, & Evans, Reference Cramer, Tuokko and Evans2001; Dyason Simon, & Martin, Reference Dyason, Simon and Martin2015; Garrett, Tuokko, Stajduhar, Lindsay, & Buehler, Reference Garrett, Tuokko, Stajduhar, Lindsay and Buehler2008; Goodridge, Reference Goodridge2010; Huggins et al., Reference Huggins, McGregor, Cox, Bauder, Slater and Yap2019; Jeznach, Tuokko, Garcia-Barrera, & Stajduhar, Reference Jeznach, Tuokko, Garcia-Barrera and Stajduhar2015; Nuhn et al., Reference Nuhn, Holmes, Kelly, Just, Shaw and Wiebe2018; Tanuseputro et al., Reference Tanuseputro, Hsu, Chalifoux, Talarico, Kobewka and Scott2019). Four studies examined the extent to which older adults considered or had already engaged in ACP (Bravo et al., Reference Bravo, Dubois and Pâquet2003, Reference Bravo, Dubois, Cohen, Wildeman, Graham, Painter and Bellemare2011; Cramer et al., Reference Cramer, Tuokko and Evans2001; Garrett et al., Reference Garrett, Tuokko, Stajduhar, Lindsay and Buehler2008). Two studies by Bravo et al. (Reference Bravo, Dubois and Pâquet2003, Reference Bravo, Dubois, Cohen, Wildeman, Graham, Painter and Bellemare2011) examined the degree to which Canadians communicated their health care preferences should they become incapacitated. A majority of subjects had completed informal plans, such as sharing their preferences orally, as compared with formalized written documents (Bravo et al., Reference Bravo, Dubois and Pâquet2003, Reference Bravo, Dubois, Cohen, Wildeman, Graham, Painter and Bellemare2011). Factors associated with ACP completion included cognitive impairment, higher age, knowing someone with a cognitive impairment, and being a woman. In one of these studies, married individuals who perceived their health as excellent had less often completed directives for health (Bravo et al., Reference Bravo, Dubois and Pâquet2003).
Similarly, two studies explored the extent to which people thought about or formalized preferences for end-of-life care or substitute decision makers (Cramer et al., Reference Cramer, Tuokko and Evans2001; Garrett et al., Reference Garrett, Tuokko, Stajduhar, Lindsay and Buehler2008). A study from Vancouver, British Columbia investigated which types of end-of-life planning seniors were completing and whether a hierarchy existed, the types of surrogate decision makers selected by married versus unmarried seniors, and how seniors discussed health preferences with others (Cramer et al., Reference Cramer, Tuokko and Evans2001). Wills and powers of attorney for finances were most common; furthermore, cognitive disabilities and age were positively associated with the completion of powers of attorney for health. Higher education was the only statistically significant predictor for completion of the aforementioned documents. Moreover, daughters were generally preferred as surrogates – as compared to spouses and sons – by married and unmarried individuals living alone and with other family members. Another study found that, although many individuals thought about substitute decision makers and expressed their health preferences, few had completed formal ACP documents (Garrett et al., Reference Garrett, Tuokko, Stajduhar, Lindsay and Buehler2008). Notably, females were 1.46 times more likely to have considered a possible surrogate than were males; higher education and Ontario residence status were predictors of such behaviour. Unmarried participants were more likely to have a formal advance directive in place than married or common-law participants. Thinking about end-of-life preferences was predictive of sharing them with others; likewise, thinking about and discussing preferences were associated with formalizing them.
Multiple studies looked at ACP participation by cognitively impaired seniors (Brink et al., Reference Brink, Smith and Kitson2008; Dyason et al., Reference Dyason, Simon and Martin2015; Goodridge, Reference Goodridge2010; Jeznach et al., Reference Jeznach, Tuokko, Garcia-Barrera and Stajduhar2015). In their study, inclusive of participants from across Canada, Jeznach et al. (Reference Jeznach, Tuokko, Garcia-Barrera and Stajduhar2015) found that older adults with cognitive impairments were more likely to have assigned a substitute decision maker and to have formalized legal documents for health care preferences or naming a decision maker. This group was also less likely to have discussed end-of-life care preferences. Patients who did not participate in ACP were less likely to die in a nursing home than in private residences, and there was no significant relationship between engaging in ACP and dying in a medical facility. Ultimately, it was noted that cognitively impaired persons experienced ACP differently than non-impaired persons. Similarly, a study of Western Canada’s acute care hospitals reviewed the charts of deceased patients and noted patterns pertaining to documents, end-of-life orders, and cognitive status (Goodridge, Reference Goodridge2010). Do not resuscitate (DNR) orders, compassionate terminal care, cardiopulmonary resuscitation (CPR), end-of-life care, comfort measures, and no codes (i.e., do not initiate CPR protocol) were most frequently cited in patients’ charts. The presence of an end-of-life order was positively associated with dementia and cancer diagnosis (Brink et al., Reference Brink, Smith and Kitson2008; Goodridge, Reference Goodridge2010). Moreover, patients accepting of their circumstances were 5.67 times more likely to have a formalized DNR, and persons with higher cognitive and functional impairments were more likely to have a recorded DNR than were unimpaired persons (Brink et al., Reference Brink, Smith and Kitson2008). Similar results were also found in the context of Alberta long-term care (LTC) and assisted living facilities (Dyason et al., Reference Dyason, Simon and Martin2015). The prevalence of cognitive impairments in LTC and assisted living facilities were 78 and 48 per cent, respectively, and a total of 272 ACP discussions were documented in the 166 charts reviewed and found to have documented ACP discussions. Residents were listed as being present in discussions about their preferences 47 per cent of the time, whereas 62 per cent of discussions had a family member in attendance. Only 20 per cent of cognitively impaired residents were documented as being present in such conversations; family members’ attendance was more common. Nurses were most commonly present in conversations, and physicians were more likely to be present in LTC than in assisted living facilities. Social workers, spiritual care providers and others (e.g., occupational therapists, pharmacists, and physiotherapists) were present 16, 2, and 15 per cent of the time, respectively, thereby reinforcing that ACP in LTC was based on relational autonomy. Likewise, studies from Huggins as well as Tanuseputro and colleagues reported that cognitive impairment, higher age, and primary language being French or English were positively associated with having completed a DNR or do-not-hospitalize order (Huggins et al., Reference Huggins, McGregor, Cox, Bauder, Slater and Yap2019; Tanuseputro et al., Reference Tanuseputro, Hsu, Chalifoux, Talarico, Kobewka and Scott2019). Their findings on the association between language and completion of ACP demonstrated the importance of considering cultural factors which hinder or promote engagement in ACP (Huggins et al., Reference Huggins, McGregor, Cox, Bauder, Slater and Yap2019; Tanuseputro et al., Reference Tanuseputro, Hsu, Chalifoux, Talarico, Kobewka and Scott2019).
Additionally, a Vancouver-based study assessed the “experiences, wishes, fears and beliefs” of patients who sought and were eligible for MAiD in the first year of its legalization (Nuhn et al., Reference Nuhn, Holmes, Kelly, Just, Shaw and Wiebe2018). Although only one participant out of 23 had dementia, the authors noted that all patients were confident in their pursuit of MAiD. Common reasons for wanting MAiD were the desire for autonomy, unacceptable quality of life, loss of independence and function, loss of physical ability, loss of ability to speak or communicate, and suffering or fear of future suffering (Nuhn et al., Reference Nuhn, Holmes, Kelly, Just, Shaw and Wiebe2018). It should be noted that pain was not frequently cited as a reason for wanting MAiD. Patients reported feeling supported when sharing their decisions to seek MAiD; most only told close friends and family, to avoid debate or the need to justify their actions. Patients’ religiosity varied from atheist to “very spiritual” (Nuhn et al., Reference Nuhn, Holmes, Kelly, Just, Shaw and Wiebe2018).
Finally, another study by Bravo et al. (Reference Bravo, Sene and Arcand2017) assessed the extent to which quality of life (QoL) ratings made by older adults in Québec were consistent with those of their designated proxies for health care, as well as consistent over time, in the context of increasing cognitive impairment. QoL ratings were persistent across time points and congruous between pairs of older adults and their proxies. This similarity was increased under worsening cognitive function, thereby suggesting the importance of conversations pertaining to QoL as part of ACP in the context of cognitive impairment as well as engaging designated proxies in these deliberations.
Opinions Regarding MAiD for Incompetent Patients
Four studies (14%) focused on the opinions of various stakeholders regarding offering MAiD to cognitively impaired patients (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018a, Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b, Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018c, Reference Bravo, Trottier, Rodrigue, Arcand, Downie and Dubois2019). Two of these elicited the opinions of Québec physicians and nurses towards extending MAiD to incompetent patients and found that both groups were generally supportive (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b, Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018c). In the context of dementia at an advanced stage, 45 and 14 per cent of 136 physicians (including family, internal medicine, neurology, psychiatry, and intensive care physicians) were in support of providing MAiD to incompetent patients with and without a formal request, respectively (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018c). In the context of dementia at a terminal stage, these percentages reached 79 and 52 per cent, respectively, for family physicians. Furthermore, 73 per cent of respondents agreed that health care preferences expressed before losing decisional capacity should carry the same weight as those expressed by a competent patient. Similarly, 83 per cent of surveyed nurses surveyed (including those working with patients with Alzheimer’s or a similar disorder, or working in geriatrics, gerontology, end-of-life care, or the public health care network) were in favour of offering MAiD to incompetent patients who were at the terminal stage of their disease, showing signs of distress, and had made the request prior to losing capacity (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b). Generally, nurses agreed with the process of self-determination and attached high value to advance directives. Importantly, there was a significant difference in support for MAiD; this difference was contingent on factors such as the perceived comfort level of the patient or the patient being in the terminal stage of their disease (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b). Three independent correlates of respondents’ attitudes were identified through multiple logistic regression: “having accompanied a relative or friend through the dying process, being somewhat or totally likely to make a MAiD request should they be diagnosed with Alzheimer’s disease, and being somewhat or totally likely to ask a physician to carry out the advance request made while competent by a now-incompetent relative diagnosed with Alzheimer’s disease” (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b).
Lay Persons’ Perspectives
Two studies assessed Québec lay persons’ perspectives towards extending MAiD to incompetent patients (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018a, Reference Bravo, Trottier, Rodrigue, Arcand, Downie and Dubois2019). Seventy-eight percent of informal caregiver survey respondents – a majority of whom were the adult child or spouse of an individual with dementia – felt that they would write an advance request for MAiD if personally diagnosed with Alzheimer’s disease (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018a). Conditions under which they would want their request for MAiD to be accommodated were physical and psychological suffering that could not be relieved, as well as complete dependence on others to fulfil basic needs. Self-determination was the most common argument in favour of rendering MAiD accessible to incompetent patients, and religiosity was identified as a correlate negatively associated with caregivers’ positive attitudes towards MAiD for the same patients. Akin to surveyed physicians, 82% of respondents expressed that all persons should have the right to decide how they would die and that preferences voiced ahead of losing capacity should be assigned equal merit to preferences expressed by a competent patient. These same respondents were supportive of extending MAiD to incompetent persons living with dementia at the advanced and terminal stages of their disease, in the presence or absence of advance requests. Finally, another study by Bravo et al. (Reference Bravo, Trottier, Rodrigue, Arcand, Downie and Dubois2019) elicited older adults’ opinions regarding MAiD for incompetent patients. In light of a dementia diagnosis, 76 per cent of the 317 respondents expressed being somewhat or extremely likely to write a request for MAiD and 74 per cent expressed being equally as likely to ask that a physician grant the MAiD request of a close relative diagnosed with the same disease. Physical pain that could not be relieved was the most common trigger for such positions, whereas admission to a LTC facility was the least common.
KT to Support Persons Living with Dementia, Professionals, and Caregivers
Five studies (17%) discussed current KT and patient engagement initiatives designed to support cognitively impaired patients and their circle of care in ACP (Arcand et al., Reference Arcand, Brazil, Nakanishi, Nakashima, Alix and Desson2013; Bayly, Blake, Peacock, Morgan, & Forbes, Reference Bayly, Blake, Peacock, Morgan and Forbes2018; Forbes et al., Reference Forbes, Finkelstein, Blake, Gibson, Morgan and Markle-Reid2012; van der Steen et al., Reference van der Steen, Arcand, Toscani, de Graas, Finetti and Beaulieu2012; Waxman, Russell, Iu, & Mulsant, Reference Waxman, Russell, Iu and Mulsant2018). Two studies examined the usefulness, quality, and acceptability of information booklets on dementia and end-of-life care (Arcand et al., Reference Arcand, Brazil, Nakanishi, Nakashima, Alix and Desson2013; van der Steen et al., Reference van der Steen, Arcand, Toscani, de Graas, Finetti and Beaulieu2012). These booklets were offered to patients – as well as family members and nurses – to inform them of dementia topics including disease trajectory, symptom management, end-of-life decision making, and conflict management, among others. Broadly, the booklets from each study were well received. The booklet examined by Arcand et al. (Reference Arcand, Brazil, Nakanishi, Nakashima, Alix and Desson2013) was generally acceptable in both French and English Canada, wherein a majority of surveyed nurses rated the booklet as a useful resource for families of persons living with advanced dementia, and had previously identified that the booklet contained information regarding the comfort care approach to dementia care at the end of life. Likewise, the booklet evaluated by van der Steen et al. (Reference van der Steen, Arcand, Toscani, de Graas, Finetti and Beaulieu2012) was highly rated by survey respondents. These respondents were also in favour of having practitioners involved in providing the resources. Importantly, both studies found similar results regarding the timing of booklet delivery; recipients wished to receive the booklet close to the time of dementia diagnosis, during goals-of-care discussions, or prior to hospital admission if applicable (Arcand et al., Reference Arcand, Brazil, Nakanishi, Nakashima, Alix and Desson2013; van der Steen et al., Reference van der Steen, Arcand, Toscani, de Graas, Finetti and Beaulieu2012).
Another two studies examined the impacts of KT programs (Bayly et al., Reference Bayly, Blake, Peacock, Morgan and Forbes2018; Waxman et al., Reference Waxman, Russell, Iu and Mulsant2018). Bayly et al. (Reference Bayly, Blake, Peacock, Morgan and Forbes2018) investigated the effects of a knowledge broker on the development and application of KT tactics for dementia care in Alberta rural home care settings. The knowledge broker, a dedicated team member, was deemed a valuable KT resource, particularly useful in rural settings where staff might have limited capacity to deliver specialized KT services to patients with dementia. The knowledge broker played a key role in facilitating knowledge exchange and negotiation, such as promoting further discussions among staff, persons living with dementia, and their families. By contrast, an intervention evaluated by Waxman et al. (Reference Waxman, Russell, Iu and Mulsant2018) assessed whether an educational session on Alzheimer’s disease affected healthy Toronto seniors’ treatment preferences, while also examining the extent to which pharmacotherapy to reduce Alzheimer’s disease symptoms was preferred over more restrictive interventions. The mean scores of correct answers on the Alzheimer’s knowledge questionnaire were 72 per cent ahead of the educational intervention, 78 per cent immediately following, and 80 per cent a month later. Participants chose less active treatments for moderate to severe stages of the disease post-educational session. Without being prompted by researchers, multiple participants expressed that they would seek MAiD should they develop Alzheimer’s disease, and that they hoped MAiD would be legalized soon. The authors affirmed the importance of considering patients’ backgrounds and familiarity with dementia when planning and implementing education on advance directives. Conversations surrounding the behavioural and psychological symptoms of dementia could impact a patient’s advance directives and health care preferences.
Finally, a study by Forbes et al. (Reference Forbes, Finkelstein, Blake, Gibson, Morgan and Markle-Reid2012) explored the information needs of multiple Southwestern Ontario stakeholders in dementia care as well as how these needs changed over time and how the aforementioned parties accessed, assessed, and applied dementia care knowledge. In this study, six stages to the dementia care journey were identified: “(1) recognizing the symptoms, (2) receiving a diagnosis, (3) loss of independence, (4) initiating and using home care and respite services, (5) LTC placement, and (6) decisions related to end-of-life care.” Rural care partners communicated that each stage required unique knowledge and that persons living with dementia rarely recognized a personal need for dementia care information. Promoters of knowledge exchange included care partners with health care knowledge who sought information, building trust amongst HCPs, patients, and caregivers, and formalized programs for information sharing with rural community organizations. Notwithstanding these facilitators, barriers included a scarcity of rural community-based dementia care services, limited capacity among caregivers, and limited availability of integrated dementia services and supports.
Barriers to and Facilitators of the Delivery of Holistic Dementia Care
Six studies (21%) looked at factors hindering or promoting the effective delivery of dementia care, particularly in the area of patient and caregiver decision making (Bernier & Régis, Reference Bernier and Régis2019; Brown, Reference Brown2003; Cohen, Reference Cohen2004; Leduc, Reference Leduc2013; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland, Wiersma, & Vange, Reference Sutherland, Wiersma and Vangel2019). Confusion and discomfort discussing the end of life and ACP were cited multiple times (Cohen, Reference Cohen2004; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). Discomfort conversing about death or similar sensitive topics – as well as fear of giving misinformation – could hinder effective communication between HCPs and patients’ family members, and ultimately prevent the initiation of ACP (Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). It was also common for families to experience difficulty discerning when a loved one had become incapable of making their own decisions (Cohen, Reference Cohen2004). Uncertain disease diagnosis and prognosis, urgency about making decisions, and lack of understanding about care options were highlighted as factors complicating ACP processes. Consequently, these findings asserted the need for more comprehensive and publicly-advertised medical and social services for vulnerable seniors and their families, in addition to improved communication means and decision-making tools to engage prospective ACP participants, caregivers, and HCPs more effectively.
Moreover, some articles discussed system-level barriers to ACP (Bernier & Régis, Reference Bernier and Régis2019; Brown, Reference Brown2003; Cohen, Reference Cohen2004; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). Factors preventing cognitively impaired older adults and their supports from accessing ACP effectively included, but were not limited to, inconsistencies in language, dominant biomedical approaches to care, lack of mandates for HCP involvement in supporting patients in ACP, form-focused policies, variable approaches to understanding autonomy, and jurisdiction-specific policies (Bernier & Régis, Reference Bernier and Régis2019; Cohen, Reference Cohen2004; Leduc, Reference Leduc2013; Straus & Stelfox, Reference Straus and Stelfox2007). Furthermore, these articles emphasized the value of understanding ACP in dementia as a collaborative and iterative process which involved multiple individuals, not just the person with dementia (Bernier & Régis, Reference Bernier and Régis2019; Cohen, Reference Cohen2004; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). A relational approach – one taking into account the broader social contexts in which individuals make decisions – was warranted, as were diverse resources for knowledge exchange and communication in the patient’s circle of care (Bernier & Régis, Reference Bernier and Régis2019; Cohen, Reference Cohen2004; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019).
Indigenous Health Considerations
Finally, two studies (7%) examined the intricacies of delivering high-quality dementia care in Canada’s Indigenous communities (Finkelstein, Forbes, & Richmond, Reference Finkelstein, Forbes and Richmond2012; Forbes et al., Reference Forbes, Blake, Thiessen, Finkelstein, Gibson and Morgan2013). A qualitative study by Forbes et al. (Reference Forbes, Blake, Thiessen, Finkelstein, Gibson and Morgan2013) assessed instances of dementia care knowledge exchange among HCPs, informal caregivers, and persons living with dementia in a First Nations community in Southwestern Ontario. Using a constructivist grounded theory approach, interviews were conducted with the aforementioned groups to inform culturally-sensitive applications of strategies for knowledge sharing in dementia care. Three themes for dementia care knowledge sharing emerged from this inquiry: “developing trusting relationships, accessing and adapting information, and applying the information.” The need to support collaboration among HCPs, informal caregivers, and persons living with dementia in planning and discussions about the future was evident. It was also clear that there was a need to address stigma and socio-cultural issues that underpinned multi-ethnic societies, particularly Indigenous ones, and contributed to inequities in health and knowledge exchange. Timely and accurate dementia diagnoses, as well as culturally-appropriate resources, were integral in enabling patients and their caregivers to seek information about the disease trajectory, treatment options, viability of supports, and legal aspects of care planning, such as designating powers of attorney. Similarly, another qualitative investigation, also performed in Southwestern Ontario, explored how dementia care was delivered to First Nations communities (Finkelstein et al., Reference Finkelstein, Forbes and Richmond2012). Here, in-depth interviews with HCPs revealed that dementia care for Indigenous persons could be understood through a care delivery framework and a knowledge framework. The first, identified goals of care, elements of care being delivered, barriers to care, and strategies to overcome these obstacles. The second, defined knowledge stakeholders, the knowledge they have, and how they share it. One of the key barriers to accomplishing these tasks was a lack of human resources for crisis management. There was a paucity of resources and programs including First Nations knowledge, thereby limiting HCPs in sharing dementia knowledge with Indigenous persons living with dementia and their caregivers, as well. Additionally, barriers such as failure of HCPs to collaborate with non-community workers, encountering mistrust from patients and community members, patients not accessing care, and burnout among providers were identified. There was a need to produce culturally-appropriate dementia care resources for Indigenous peoples, develop patient and community relationships, investigate knowledge gaps in this specific population, involve family members in the care of persons with dementia, and support caregivers by accepting their limitations.
Discussion
To answer the question “What is the feasibility and acceptability of advance care planning for older adults (≥65 years of age) diagnosed with dementia in Canada?” we performed a scoping review of the Canadian literature published between 1 January 2000 and 31 December 2019. The results from this review elucidate the feasibility and acceptability of ACP for Canadian seniors (≥65 years of age) diagnosed with dementia. Many older Canadians have considered health care preferences in the event of decisional incapacity; numerous incompetent patients present with completed ACP such as advance directives. Despite positive levels of engagement in ACP, there are considerable barriers which restrict patients, especially those living with dementia, along with the members of their circle of care, from accessing ACP. Indigenous persons living with dementia, caregivers, and providers encounter distinct challenges in this area. Importantly, recent work also illuminates professional and lay opinions towards expanding MAiD access to include incompetent patients. Such findings support that the landscape of ACP and end-of-life care for Canadian seniors living with dementia is fluid.
The findings from this review demonstrate the usefulness of exploring how Canadian seniors living with dementia might be best enabled to partake in ACP, with the support of caregivers and HCPs alike. Importantly, our findings highlight the extent to which older Canadian adults have completed ACP or thought about their health care wishes in the event they became incapacitated (Bravo et al., Reference Bravo, Dubois and Pâquet2003, Reference Bravo, Dubois, Cohen, Wildeman, Graham, Painter and Bellemare2011, Reference Bravo, Sene and Arcand2017; Brink et al., Reference Brink, Smith and Kitson2008; Cramer et al., Reference Cramer, Tuokko and Evans2001; Dyason et al., Reference Dyason, Simon and Martin2015; Garrett et al., Reference Garrett, Tuokko, Stajduhar, Lindsay and Buehler2008; Goodridge, Reference Goodridge2010; Huggins et al., Reference Huggins, McGregor, Cox, Bauder, Slater and Yap2019; Jeznach et al., Reference Jeznach, Tuokko, Garcia-Barrera and Stajduhar2015; Nuhn et al., Reference Nuhn, Holmes, Kelly, Just, Shaw and Wiebe2018; Tanuseputro et al., Reference Tanuseputro, Hsu, Chalifoux, Talarico, Kobewka and Scott2019). Although many individuals have thought about ACP or discussed their preferences informally, few have actually proceeded to formally documenting these wishes. Further, quite a few studies confirmed the existence of practical and emotional barriers preventing patients, caregivers, and HCPs from completing ACP (Bernier & Régis, Reference Bernier and Régis2019; Brown, Reference Brown2003; Cohen, Reference Cohen2004; Leduc, Reference Leduc2013; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). Uniquely, this review also highlights the literature examining ACP considerations specific to persons living with dementia, as well as their caregivers and HCPs, in Indigenous communities. Finally, our findings showcase recent work assessing the potential for interventions such as MAiD to become more accessible regardless of cognitive status (Bravo et al., Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018a, Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018b, Reference Bravo, Rodrigue, Arcand, Downie, Dubois and Kaasalainen2018c, Reference Bravo, Trottier, Rodrigue, Arcand, Downie and Dubois2019).
Canadian Literature in the Context of International Findings
Much of the literature reviewed in our study echoes findings from international studies. First, results from studies such as Ashton and colleagues’ work from the United Kingdom support the value of engaging informal caregivers in the ACP process for persons living with dementia (Ashton, Roe, Jack, & McClelland, Reference Ashton, Roe, Jack and McClelland2016). These individuals should be encouraged to seek information about the suitability of end-of-life care such as medical and nursing interventions (Ashton et al., Reference Ashton, Roe, Jack and McClelland2016). Additional work from the United Kingdom also concluded that, despite awareness of ACP benefits, staff, such as nursing home managers, were often hesitant to engage in the process because of knowledge deficits (Beck, McIlfatrick, Hasson, & Leavey, Reference Beck, McIlfatrick, Hasson and Leavey2017). Further training, education, and role clarification are required to target individual, organization, and system-level elements that prevent ACP for persons living with dementia (Beck et al., Reference Beck, McIlfatrick, Hasson and Leavey2017). Beyond conveying the need to involve formal and informal caregivers in ACP, a study from The Netherlands also explored the ACP barriers and facilitators experienced by community-dwelling persons living with dementia (Tilburgs et al., Reference Tilburgs, Vernooij-Dassen, Koopmans, Weidema, Perry and Engels2018b). Similar to findings from Canada, successful ACP engagement by persons living with dementia was largely contingent on developing trust among involved parties and discussing both medical and non-medical topics during ACP discussions (Tilburgs et al., Reference Tilburgs, Vernooij-Dassen, Koopmans, Weidema, Perry and Engels2018b). Concerns, such as physician time constraints, were analogous with our review’s findings. Huang and colleagues’ findings from Taiwan similarly reported on the usefulness of an educational intervention for strengthening both persons living with dementia and their informal caregivers’ ACP knowledge (Huang, Lu, Liu, & Chang, Reference Huang, Lu, Liu and Chang2020). Here, a family-centred ACP educational intervention conducted in the outpatient setting with persons living with mild dementia was effective in enhancing awareness and understanding of end-stage dementia care options and ACP, ultimately emphasizing the importance of making education a key component of dementia care (Huang et al., Reference Huang, Lu, Liu and Chang2020).
Policy Recommendations
There is a clear need to enhance and coordinate efforts to promote equitable access to, as well as delivery of, ACP for persons living with dementia, irrespective of age or their partners in care. As noted in the literature, several system-level barriers prevent cognitively impaired patients and their caregivers from actively and meaningfully engaging in ACP (Bernier & Régis, Reference Bernier and Régis2019; Brown, Reference Brown2003; Cohen, Reference Cohen2004; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). Policies should consider the practical limitations faced by those who will be most implicated, when developing means to implement policies. This may include rendering ACP language and terminology more suitable to lay persons, and/or introducing ACP processes that are not necessarily restricted to paper forms.
Moreover, positive attitudes from HCPs and lay persons surrounding access to ACP and MAiD for persons living with dementia suggest that MAiD should remain on the health policy agenda, if not be moved to the forefront. Given the support it is receiving in both professional and lay communities, more nuanced discussions should be held to ascertain and evaluate the legal and practical factors which may enable MAiD to become more widely accessible to patients regardless of cognitive status and decisional capacity, while still appreciating the differences in complex legal frameworks among jurisdictions. Multiple expert and lay stakeholders should be included in these deliberations to ensure that diverse viewpoints inform people-centred programs and policies. Some such conversations have already been initiated, for example, the extensive review of MAiD which was undertaken in 2016 included a “Call for Input” wherein Canadian groups and organizations could submit relevant information for panel consideration; as well as the recent forum which took place in Québec to engage multiple stakeholders in discussions about end-of-life care (Santé et Services sociaux Québec, 2020). Likewise, additional expert groups have recently offered recommendations pertaining to MAiD for persons living with mental disorders, spanning topics such as standards for clinical MAiD assessments and improved availability of social supports, to name a few (Council of Canadian Academies, 2018a, 2018b; Halifax Group, 2020). In October 2020, Bill C-7 An Act to Amend the Criminal Code (Assistance in Dying) was tabled in the House of Commons, to formalize exceptions to the existing criteria for final consent (Department of Justice, 2020). Whereas until the bill passed just recently, individuals receiving MAiD were required to provide final consent at the time of administration, a key goal of the new bill was to amend this criterion, among others, to include individuals “whose natural death is reasonably foreseeable and who have entered into an advance consent agreement” (Department of Justice, 2020). In other words, this new bill suggests that an individual who has formalized a request for MAiD as part of their advance care plan may be eligible to receive it whilst being incapacitated (with the safeguard that “MAID would not be permitted on the basis of such an agreement if the person demonstrates – by words, sounds or gestures – refusal or resistance to the administration of a substance that would cause their death”). Formerly this was not possible and persons living with dementia remained excluded from accessing MAiD. These recent developments in MAiD policy making emphasize the importance of ensuring that ACP and MAiD are discussed with persons living with dementia early in their disease trajectory. Lastly, the broad support for MAiD evidenced in this review, and the apparent relevant political will at the federal level, make the importance of advocacy efforts in the areas of ACP, MAiD, (hospice) palliative care, and geriatric care increasingly salient.
Practice Recommendations
In clinical practice, there is a need to acknowledge the bio-psycho-social contexts in which persons living with dementia and their circle of care conceptualize and formalize ACP. This review’s findings note value in using relational autonomy as a basis for ACP and involving multiple parties in the process. Many of the studies synthesized in this review also illustrated knowledge gaps as barriers to participating in ACP (Bernier & Régis, Reference Bernier and Régis2019; Brown, Reference Brown2003; Cohen, Reference Cohen2004; Leduc, Reference Leduc2013; Straus & Stelfox, Reference Straus and Stelfox2007; Sutherland et al., Reference Sutherland, Wiersma and Vangel2019). Patients, caregivers, and HCPs are unable to fully participate in ACP when they lack the requisite information to navigate the intricacies of the process. Although an array of online resources exists for numerous dementia-related topics, for example those provided by the Alzheimer Society of Canada (2020), this review’s findings suggest a need for tools dedicated to ACP which can be implemented in diverse settings to support both HCPs and lay persons in the process. Such tools would include a holistic collection of information, pertaining not only to the disease trajectory of dementia or end-of-life care options, but also to the practical and emotional aspects of ACP. For example, the inclusion of recommendations for having difficult conversations, negotiating cultural beliefs, or navigating legal processes when formulating ACP may be incorporated. To optimize benefits at the patient, staff, and system levels, the timely introduction of these tools should become a routine aspect of the current standard of clinical dementia care.
Research Recommendations
Certain groups may be prone to facing increased barriers to health care, particularly as a result of disparities in access to ACP. This has also been demonstrated in existing literature from outside of Canada (Pettigrew et al., Reference Pettigrew, Brichko, Black, O’Connor, Austrom and Robinson2020). Based on the sparseness of studies in this review, it is unambiguous that further research is vital to identify persons living with dementia who are at risk for marginalization and inadvertent exclusion from ACP discussions and processes. Little has been reported overall on Canadian socio-economic and socio-cultural factors which might be predictors of inclusion or exclusion from formal ACP. To this end, future studies could also consider how potential programs might be developed and implemented to foster guided discussions in a variety of settings where older adults may dwell. For example, such programs could be established in LTC and assisted living facilities, regardless of residents’ cognitive statuses. Lastly, the results of this study demonstrate the need for sustained funding to support research in the areas of dementia, ACP, and MAiD. The overall limitedness of Canadian literature exhibits the need for increased commitment to investigating these topics, so that the aforementioned policy and practice recommendations may be achieved.
Strengths and Limitations
This scoping review of the literature is limited given that studies not published in English or available online through the University of Toronto Library System in full and free of charge were excluded. For these reasons, our results may be biased. Only articles which could be accessed through the university library system in full and without financial cost were included, because the project was unfunded and undertaken as university coursework (B.K.A.). Furthermore, multiple synthesized articles were published by the same authors or research teams. Despite these limitations, however, our methodology involved hand searching Google (Scholar) in attempts to capture a comprehensive collection of literature, with the literature search strategy itself refined through librarian support.
Conclusions
This scoping review of the literature, as per Arksey and O’Malley’s (Reference Arksey and O’Malley2005) framework, assessed the feasibility and acceptability of ACP for Canadian seniors (≥ 65 years of age) diagnosed with dementia. The review’s findings contribute to the global literature on ACP for persons living with cognitive impairments, by surveying and synthesizing the state of the Canadian knowledge base on this topic. Importantly, this study highlights Canadian research findings that echo international literature on aspects of ACP such as engagement levels, barriers, and facilitators, as well as unmet patient and provider needs. In response to the results, this review provides propositions for policy, practice, and research, such that ACP may be emphasized as a critical aspect of equitable and high-quality dementia care for residents of Canada. There are numerous patient- and system-level barriers preventing seniors living with dementia, their caregivers, and providers from effectively engaging in ACP. Moreover, there is a range of lay and professional opinions towards extending access to interventions such as MAiD to incompetent patients. Future research should investigate socio-cultural and socio-demographic factors promoting or deterring seniors living with dementia – and their circle of care – from accessing ACP, practice should include the delivery of ACP KT tools, and policy deliberations should engage numerous stakeholders and adopt a multidisciplinary approach.



