
87 results
Childhood adversities characterize the heterogeneity in the brain pattern of individuals during neurodevelopment
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 21 March 2024, pp. 1-13
-
- Article
- Export citation
2 The Contribution of Brain Metastases to Neurocognitive Functioning in Patients with Advanced Metastatic Cancer
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 682-683
-
- Article
-
- You have access
- Export citation
PP129 Health Technology Assessment Adaptation: Pharyngolaryngeal Biopsies (OLB) For People with Suspected Head and Neck Cancer in the Outpatient Setting
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 39 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 14 December 2023, p. S86
-
- Article
-
- You have access
- Export citation
Antibiotic practice and stewardship in the management of neutropenic fever: A survey of US institutions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s25
-
- Article
-
- You have access
- Open access
- Export citation
Extension event attendance increases adoption of weed management practices by sports field managers
-
- Journal:
- Weed Technology / Volume 37 / Issue 5 / October 2023
- Published online by Cambridge University Press:
- 20 September 2023, pp. 578-587
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association of cannabis, cannabidiol and synthetic cannabinoid use with mental health in UK adolescents
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 24 July 2023, pp. 478-484
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Advancing college food security: priority research gaps
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 1 / June 2024
- Published online by Cambridge University Press:
- 09 May 2023, pp. 108-120
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Timing Their Positions: Cosponsorship in the State Legislature
-
- Journal:
- State Politics & Policy Quarterly / Volume 23 / Issue 3 / September 2023
- Published online by Cambridge University Press:
- 02 May 2023, pp. 245-266
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Reduced Healthcare Resource Utilization in Patients With Chronic Insomnia 24 Months After Treatment With Digital CBT-I: A Matched-Control Study
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 2 / April 2023
- Published online by Cambridge University Press:
- 14 April 2023, pp. 228-229
-
- Article
-
- You have access
- Export citation
A multimodal strategy to improve race/ethnic group equity in administration of neutralizing monoclonal antibody treatment for COVID-19 outpatients
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 10 February 2023, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Creating a culture that supports food security and health equity at higher education institutions
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 02 November 2022, pp. 503-509
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The ‘human element’ in the social space of the courtroom: framing and shaping the deliberative process in mental capacity law
-
- Journal:
- Legal Studies / Volume 42 / Issue 4 / December 2022
- Published online by Cambridge University Press:
- 24 May 2022, pp. 715-734
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Pediatric Blast Trauma: A Systematic Review and Meta-Analysis of Factors Associated with Mortality and Description of Injury Profiles
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 4 / August 2022
- Published online by Cambridge University Press:
- 23 May 2022, pp. 492-501
- Print publication:
- August 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characteristics of healthcare personnel who reported concerns related to PPE use during care of COVID-19 patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s8-s9
-
- Article
-
- You have access
- Open access
- Export citation
-
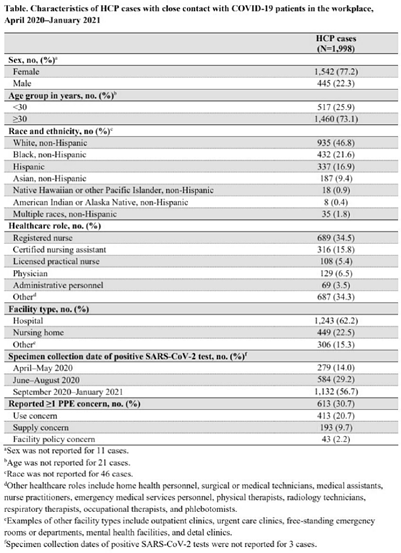
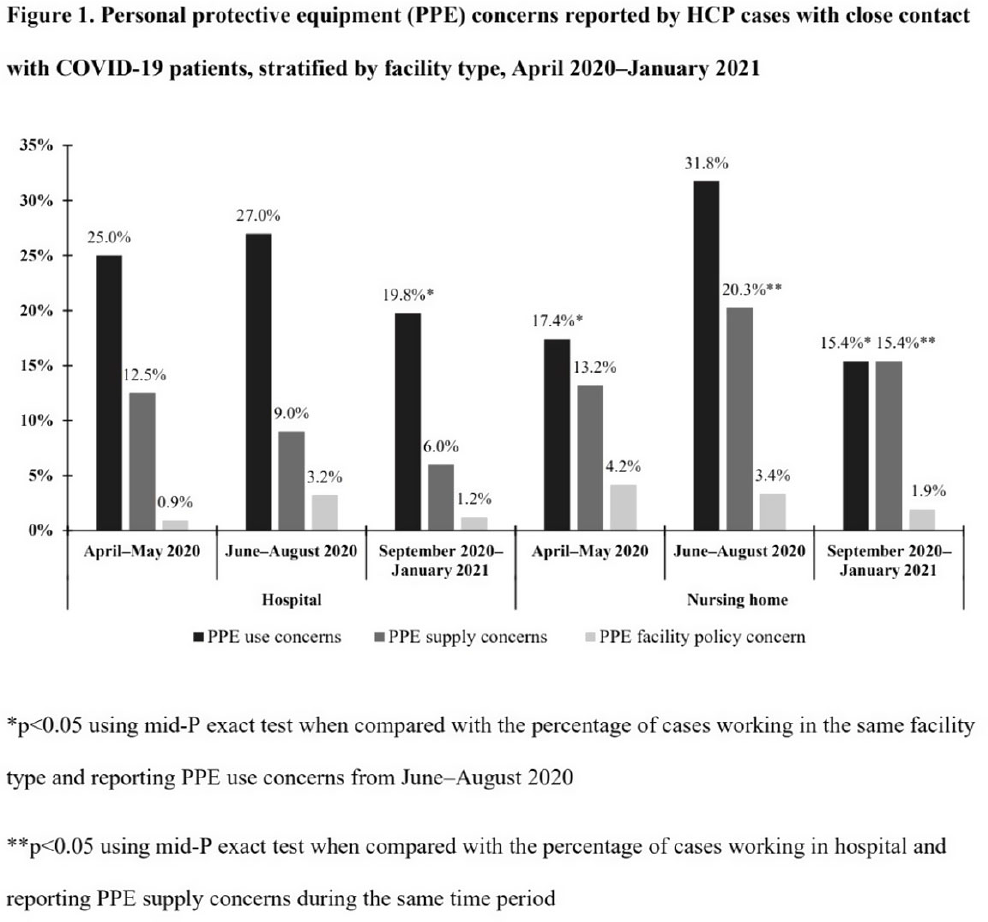
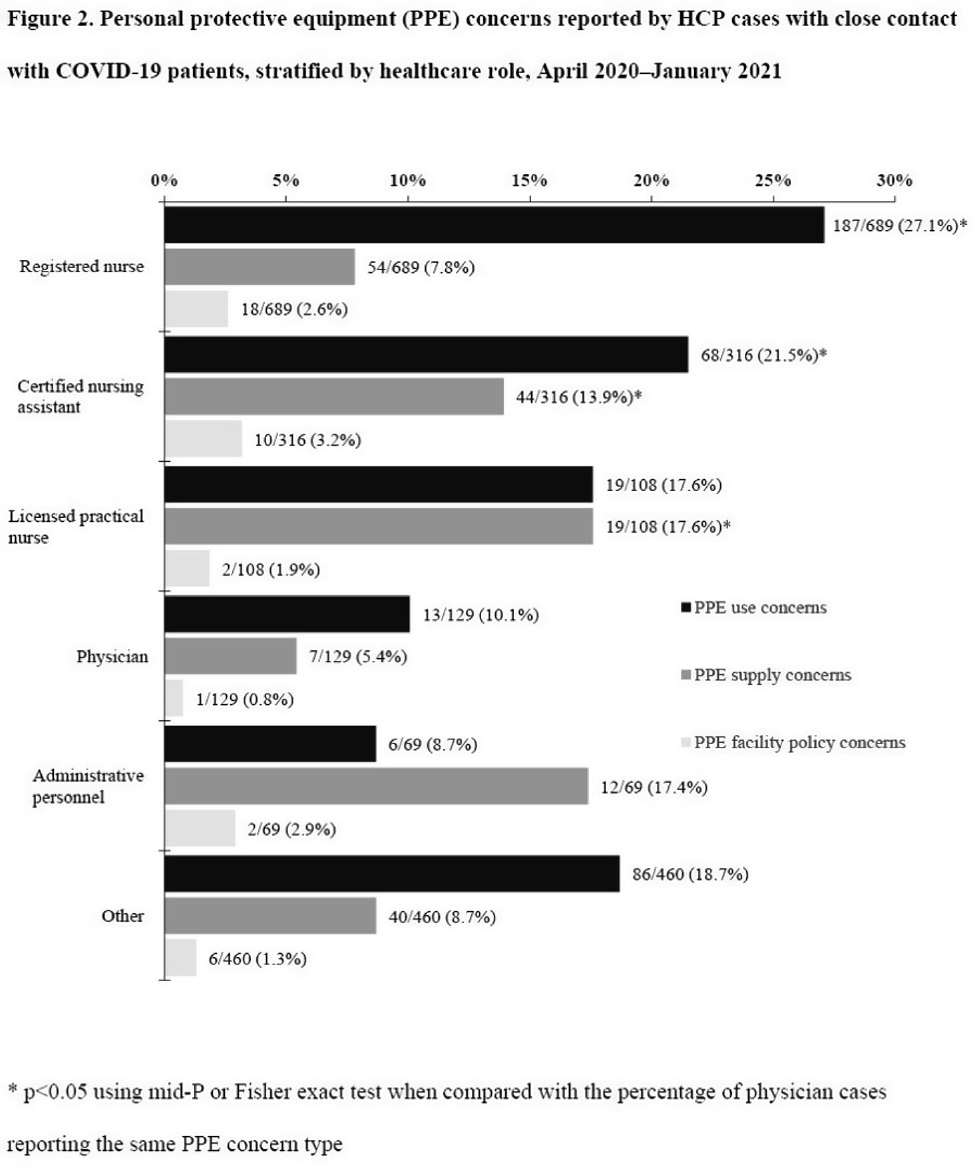
Background: Healthcare facilities have experienced many challenges during the COVID-19 pandemic, including limited personal protective equipment (PPE) supplies. Healthcare personnel (HCP) rely on PPE, vaccines, and other infection control measures to prevent SARS-CoV-2 infections. We describe PPE concerns reported by HCP who had close contact with COVID-19 patients in the workplace and tested positive for SARS-CoV-2. Method: The CDC collaborated with Emerging Infections Program (EIP) sites in 10 states to conduct surveillance for SARS-CoV-2 infections in HCP. EIP staff interviewed HCP with positive SARS-CoV-2 viral tests (ie, cases) to collect data on demographics, healthcare roles, exposures, PPE use, and concerns about their PPE use during COVID-19 patient care in the 14 days before the HCP’s SARS-CoV-2 positive test. PPE concerns were qualitatively coded as being related to supply (eg, low quality, shortages); use (eg, extended use, reuse, lack of fit test); or facility policy (eg, lack of guidance). We calculated and compared the percentages of cases reporting each concern type during the initial phase of the pandemic (April–May 2020), during the first US peak of daily COVID-19 cases (June–August 2020), and during the second US peak (September 2020–January 2021). We compared percentages using mid-P or Fisher exact tests (α = 0.05). Results: Among 1,998 HCP cases occurring during April 2020–January 2021 who had close contact with COVID-19 patients, 613 (30.7%) reported ≥1 PPE concern (Table 1). The percentage of cases reporting supply or use concerns was higher during the first peak period than the second peak period (supply concerns: 12.5% vs 7.5%; use concerns: 25.5% vs 18.2%; p Conclusions: Although lower percentages of HCP cases overall reported PPE concerns after the first US peak, our results highlight the importance of developing capacity to produce and distribute PPE during times of increased demand. The difference we observed among selected groups of cases may indicate that PPE access and use were more challenging for some, such as nonphysicians and nursing home HCP. These findings underscore the need to ensure that PPE is accessible and used correctly by HCP for whom use is recommended.
Funding: None
Disclosures: None



Defining the role of the hypothalamic-pituitary-adrenal axis in the relationship between fetal growth and adult cardiometabolic outcomes
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 13 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 21 April 2022, pp. 683-694
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Risk clustering and psychopathology from a multi-center cohort of Indian children, adolescents, and young adults
-
- Journal:
- Development and Psychopathology / Volume 35 / Issue 2 / May 2023
- Published online by Cambridge University Press:
- 08 April 2022, pp. 800-808
-
- Article
- Export citation
Suicide and other causes of death among working-age and older adults in the year after discharge from in-patient mental healthcare in England: matched cohort study
-
- Journal:
- The British Journal of Psychiatry / Volume 221 / Issue 2 / August 2022
- Published online by Cambridge University Press:
- 14 December 2021, pp. 468-475
- Print publication:
- August 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A longitudinal study of predictors of serious psychological distress during COVID-19 pandemic
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 6 / April 2023
- Published online by Cambridge University Press:
- 11 October 2021, pp. 2418-2426
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effect of frequent assessment of suicidal thinking on its incidence and severity: high-resolution real-time monitoring study
-
- Journal:
- The British Journal of Psychiatry / Volume 220 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 09 July 2021, pp. 41-43
- Print publication:
- January 2022
-
- Article
-
- You have access
- HTML
- Export citation
