
659 results
Teleonomy, legibility, and diversity: Do we need more “proxynomics”?
-
- Journal:
- Behavioral and Brain Sciences / Volume 47 / 2024
- Published online by Cambridge University Press:
- 13 May 2024, e88
-
- Article
- Export citation
The Role of Individual Income in Modulating the Impact of Health Determinants: Exploring the Interplay between Socioeconomic Factors and Health Outcomes
-
- Journal:
- European Review / Volume 32 / Issue 2 / April 2024
- Published online by Cambridge University Press:
- 24 April 2024, pp. 150-176
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A next-generation protective emblem: Cross-frequency protective options for non-combatants in the context of (fully) autonomous warfare
-
- Journal:
- International Review of the Red Cross , First View
- Published online by Cambridge University Press:
- 20 March 2024, pp. 1-29
-
- Article
- Export citation
Associations between disturbed sleep and attenuated psychotic experiences in people at clinical high risk for psychosis
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 07 March 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Lateral flexure of Erebus Ice Tongue due to ocean current forcing and fast ice coupling
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 29 February 2024, pp. 1-13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Dissolution Rates of Allophane With Variable Fe Contents: Implications for Aqueous Alteration and the Preservation of X-Ray Amorphous Materials on Mars
-
- Journal:
- Clays and Clay Minerals / Volume 69 / Issue 2 / April 2021
- Published online by Cambridge University Press:
- 01 January 2024, pp. 263-288
-
- Article
- Export citation
11 NASA-TLX Workload Profile of the Trail Making Test
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 695-696
-
- Article
-
- You have access
- Export citation
The nonlinear evolution of whistler-mode chorus: modulation instability as the source of tones
-
- Journal:
- Journal of Plasma Physics / Volume 89 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 12 December 2023, 905890607
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We review the modulation stability of parallel-propagating/field-aligned whistler-mode chorus (WMC) waves propagating in a warm plasma from a formal perspective with a focus on wave–particle interactions via ponderomotive forces. The modulation instability criteria are characterised by the group velocity dispersion, $d c_g/dk$
 , for whistler-mode waves and a condition on the ratio between the group velocity $c_g$
, for whistler-mode waves and a condition on the ratio between the group velocity $c_g$ and the electron sound speed $c_{s,e}$
and the electron sound speed $c_{s,e}$ . We also demonstrate that in order to investigate the spatiotemporal evolution of the envelope and the formation of packets (according to this mechanism), one necessarily needs to account for the motion of ions within the system, leading to an ionic influence on the modulation instability threshold determined by the ion fraction of the plasma. Finally, we demonstrate that chirping may be captured when higher-order effects are included within the spatiotemporal evolution of the amplitude. This yields not only an explicit expression for the sweep rate but also identifies a possible origin for the power band gap that occurs at half the electron gyrofrequency. Numerical validation demonstrates that the interaction between wave packets is a source for the emergence of tones observed within mission data, and such interactions may be a major source of the electron energisation which WMC are responsible for.
. We also demonstrate that in order to investigate the spatiotemporal evolution of the envelope and the formation of packets (according to this mechanism), one necessarily needs to account for the motion of ions within the system, leading to an ionic influence on the modulation instability threshold determined by the ion fraction of the plasma. Finally, we demonstrate that chirping may be captured when higher-order effects are included within the spatiotemporal evolution of the amplitude. This yields not only an explicit expression for the sweep rate but also identifies a possible origin for the power band gap that occurs at half the electron gyrofrequency. Numerical validation demonstrates that the interaction between wave packets is a source for the emergence of tones observed within mission data, and such interactions may be a major source of the electron energisation which WMC are responsible for.



Income or educational attainment: which is more effective in the fight against overweight? Evidence from Spain and Andalusia
-
- Journal:
- Journal of Biosocial Science / Volume 56 / Issue 2 / March 2024
- Published online by Cambridge University Press:
- 04 December 2023, pp. 270-291
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ten new insights in climate science 2023
-
- Journal:
- Global Sustainability / Volume 7 / 2024
- Published online by Cambridge University Press:
- 01 December 2023, e19
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The influence of peer non-suicidal self-harm on young adults’ urges to self-harm: experimental study
-
- Journal:
- Acta Neuropsychiatrica , First View
- Published online by Cambridge University Press:
- 28 November 2023, pp. 1-13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Parametrized polyconvex hyperelasticity with physics-augmented neural networks
-
- Journal:
- Data-Centric Engineering / Volume 4 / 2023
- Published online by Cambridge University Press:
- 03 November 2023, e25
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Childhood trauma moderates schizotypy-related brain morphology: analyses of 1182 healthy individuals from the ENIGMA schizotypy working group
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 6 / April 2024
- Published online by Cambridge University Press:
- 20 October 2023, pp. 1215-1227
-
- Article
- Export citation
Sarcocystis cruzi (Hasselmann, 1923) Wenyon, 1926: redescription, molecular characterization and deposition of life cycle stages specimens in the Smithsonian Museum
-
- Journal:
- Parasitology / Volume 150 / Issue 13 / November 2023
- Published online by Cambridge University Press:
- 18 October 2023, pp. 1192-1206
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trajectories of remitted psychotic depression: identification of predictors of worsening by machine learning
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 6 / April 2024
- Published online by Cambridge University Press:
- 11 October 2023, pp. 1142-1151
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
For the Sake of the Ingroup: The Double-Edged Effects of Collectivism on Workplace Unethical Behavior
-
- Journal:
- Business Ethics Quarterly , First View
- Published online by Cambridge University Press:
- 02 October 2023, pp. 1-35
-
- Article
- Export citation
Sex differences in iron status during military training: a prospective cohort study of longitudinal changes and associations with endurance performance and musculoskeletal outcomes
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 4 / 28 February 2024
- Published online by Cambridge University Press:
- 21 September 2023, pp. 581-592
- Print publication:
- 28 February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Understanding the impact of the COVID-19 pandemic response on GI infection surveillance trends in England, January 2020–April 2022
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 25 August 2023, e147
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Suicidal risk in Latino patients with schizophrenia
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1080-S1081
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Schizophrenia is a highly debilitating disorder afflicting more than 24 million individuals worldwide. In Mexico, the Ministry of Health estimates that it affects more than 1 million people. Suicide is one of the main causes of death among people diagnosed with schizophrenia, their risk is 12 times higher than in. the general population
ObjectivesTo evaluate the clinical characteristics of schizophrenic patients at risk of suicide in the Latino population.
MethodsWe included 130 patients recruited from genetics studies in Latino patients with schizophrenia from the outpatient and inpatient psychiatric ward of the University Hospital “Dr José E. González” in Monterrey, Nuevo Leon, Mexico. Beck Depression Inventory (BDI-II), the Convergent Functional Information for Suicidality (CFI-S) were applied to all participants. We compared the sociodemographic and clinical characteristics of patients with suicidal risk (measured by history of suicidal attempt or current suicidal risk) and present depressive episode.
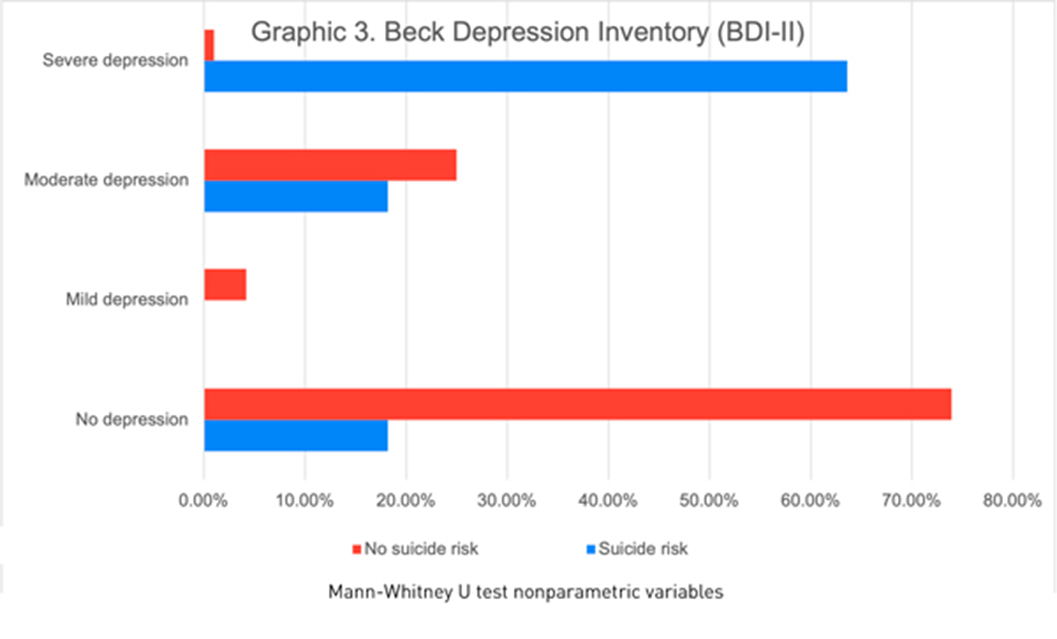
ResultsOf the 130 participants, 66.9% were male, the median age was 38 years. We found 11(14.3%) patients with suicidal risk and 119 (91.5%) without suicidal risk. Sociodemographic and clinical characteristics of the study population at risk of suicide are described in graphic 1. Patients with a history of suicide attempt scored higher on the CFI-S scale with a median of 0.5 (q1=0.45; q3=0.54) vs. 0.31 (q1=0.22; q3=0.45) (p= 0.004)(Graphic 2). Based on the BDI-II we found 2.30% patients showed a mild depression, 20.0% moderate depression and 4.61% severe depression (graphic 3). Schizophrenic patients with a previous suicide attempt and depressive episode had higher score range in CFI-S, median .65 (q1=.65; q2=.59, p=0.000). Also, 63.60% were severely depressive (p=0.000) when they compared with patients with low risk of suicide. Schizophrenic patients with suicidal risk were characterized by: age >=60 years old, unemployment, no children, single, without religion, family history of suicide, previous suicide attempt, depressive episodes, substance abuse, auditory hallucinations and referential delusions.
Image:
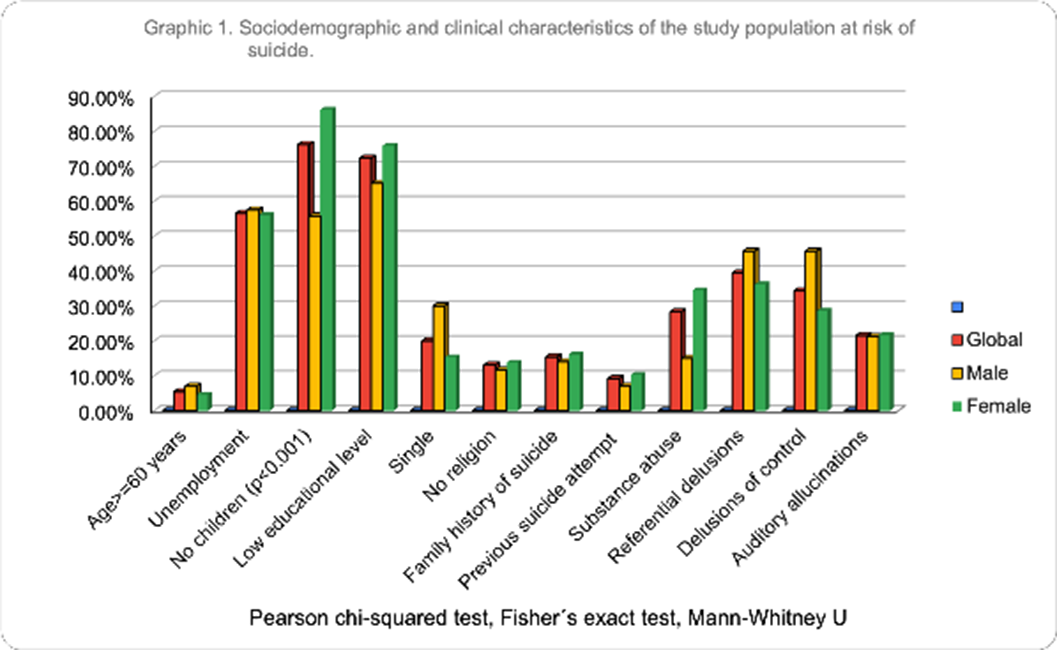
Image 2:
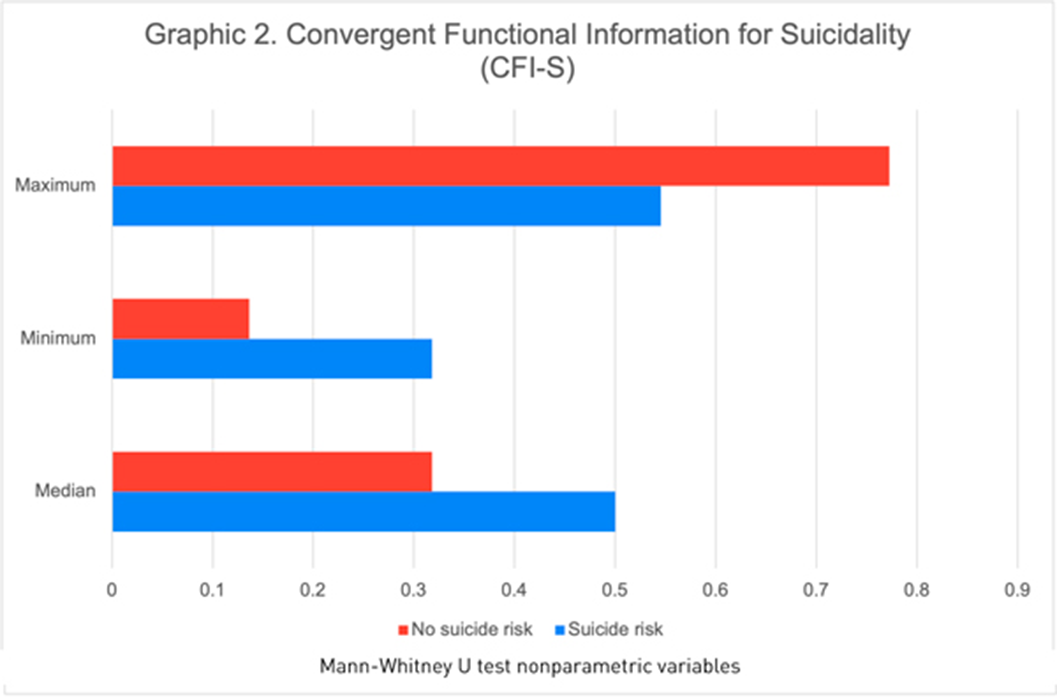
Image 3:
 Conclusions
ConclusionsIn our study with Latino population, we observed similar clinical characteristics predictive of suicide risk described in the international studies. Our study is relevant to applied preventive measures in groups of schizophrenic patients with risk factors and their relatives.
Disclosure of InterestNone Declared



Mental health and addiction in young refugees-Research on prevalence of alcohol and substance use, PTSD and psychological difficulties experienced by young migrants and refugees placed in two refugee centers in Serbia in the time of COVID-19 pandemic
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S37-S38
-
- Article
-
- You have access
- Open access
- Export citation
