
351 results
On the probability of a Pareto record
- Part of
-
- Journal:
- Probability in the Engineering and Informational Sciences , First View
- Published online by Cambridge University Press:
- 04 June 2024, pp. 1-13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
Given a sequence of independent random vectors taking values in
 ${\mathbb R}^d$ and having common continuous distribution function F, say that the
${\mathbb R}^d$ and having common continuous distribution function F, say that the  $n^{\rm \scriptsize}$th observation sets a (Pareto) record if it is not dominated (in every coordinate) by any preceding observation. Let
$n^{\rm \scriptsize}$th observation sets a (Pareto) record if it is not dominated (in every coordinate) by any preceding observation. Let  $p_n(F) \equiv p_{n, d}(F)$ denote the probability that the
$p_n(F) \equiv p_{n, d}(F)$ denote the probability that the  $n^{\rm \scriptsize}$th observation sets a record. There are many interesting questions to address concerning pn and multivariate records more generally, but this short paper focuses on how pn varies with F, particularly if, under F, the coordinates exhibit negative dependence or positive dependence (rather than independence, a more-studied case). We introduce new notions of negative and positive dependence ideally suited for such a study, called negative record-setting probability dependence (NRPD) and positive record-setting probability dependence (PRPD), relate these notions to existing notions of dependence, and for fixed
$n^{\rm \scriptsize}$th observation sets a record. There are many interesting questions to address concerning pn and multivariate records more generally, but this short paper focuses on how pn varies with F, particularly if, under F, the coordinates exhibit negative dependence or positive dependence (rather than independence, a more-studied case). We introduce new notions of negative and positive dependence ideally suited for such a study, called negative record-setting probability dependence (NRPD) and positive record-setting probability dependence (PRPD), relate these notions to existing notions of dependence, and for fixed  $d \geq 2$ and
$d \geq 2$ and  $n \geq 1$ prove that the image of the mapping pn on the domain of NRPD (respectively, PRPD) distributions is
$n \geq 1$ prove that the image of the mapping pn on the domain of NRPD (respectively, PRPD) distributions is  $[p^*_n, 1]$ (resp.,
$[p^*_n, 1]$ (resp.,  $[n^{-1}, p^*_n]$), where
$[n^{-1}, p^*_n]$), where  $p^*_n$ is the record-setting probability for any continuous F governing independent coordinates.
$p^*_n$ is the record-setting probability for any continuous F governing independent coordinates.









115 Strategies for Training and Advancing under-represented Researchers (STARs)
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 33
-
- Article
-
- You have access
- Open access
- Export citation
The Pandemic and Political Behavior: Staying the Course
-
- Journal:
- PS: Political Science & Politics , First View
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Extension event attendance increases adoption of weed management practices by sports field managers
-
- Journal:
- Weed Technology / Volume 37 / Issue 5 / October 2023
- Published online by Cambridge University Press:
- 20 September 2023, pp. 578-587
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The age and paleoclimate implications of relict periglacial block deposits on the New England Tablelands, Australia
-
- Journal:
- Quaternary Research / Volume 111 / January 2023
- Published online by Cambridge University Press:
- 23 August 2022, pp. 121-137
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Using laboratory intergroup conflict and riots as a “stress test”
-
- Journal:
- Behavioral and Brain Sciences / Volume 45 / 2022
- Published online by Cambridge University Press:
- 07 July 2022, e98
-
- Article
- Export citation
6 - Care arrangements for older adults: exploring the intergenerational contract in emigrant households of Goa, India
-
-
- Book:
- Care for Older Adults in India
- Published by:
- Bristol University Press
- Published online:
- 13 October 2022
- Print publication:
- 31 May 2022, pp 86-117
-
- Chapter
- Export citation
Chapter 13 - Programs with Promise
- from Part III - Strategies for Inclusion and Retention
-
-
- Book:
- We're Not OK
- Published online:
- 21 April 2022
- Print publication:
- 05 May 2022, pp 218-232
-
- Chapter
- Export citation
Automating 3D Imaging of Inorganic Nanoparticles
-
- Journal:
- Microscopy and Microanalysis / Volume 27 / Issue S1 / August 2021
- Published online by Cambridge University Press:
- 30 July 2021, pp. 2864-2866
- Print publication:
- August 2021
-
- Article
-
- You have access
- Export citation
Nomenclature for Pediatric and Congenital Cardiac Care: Unification of Clinical and Administrative Nomenclature – The 2021 International Paediatric and Congenital Cardiac Code (IPCCC) and the Eleventh Revision of the International Classification of Diseases (ICD-11)
- Part of
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 7 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. 1057-1188
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antimicrobial Stewardship-Driven Monoclonal Antibody Treatment Program for COVID-19 Patients in the Bronx, New York
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s57
-
- Article
-
- You have access
- Open access
- Export citation
-
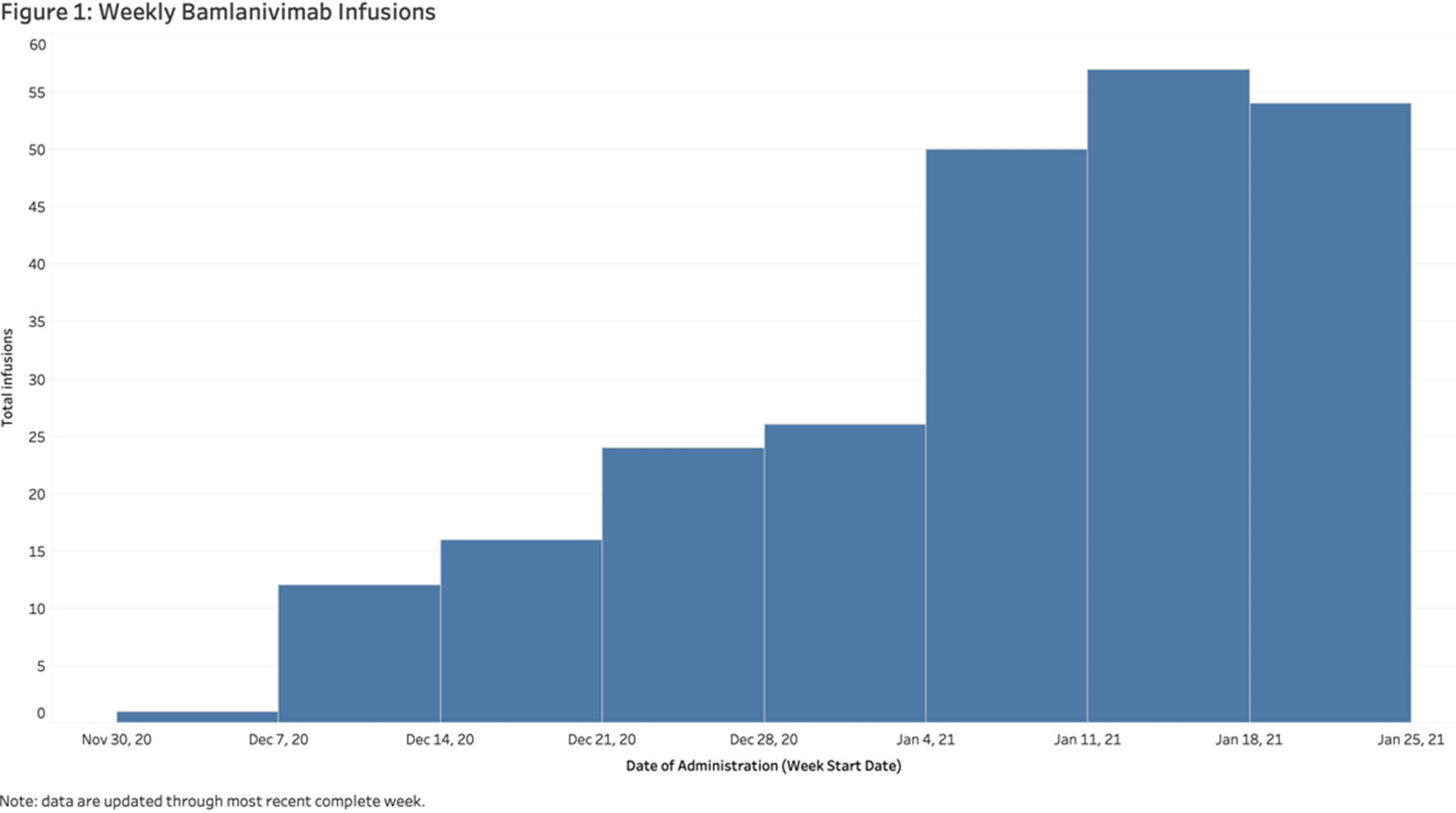
Background: In November 2020, bamlanivimab received emergency use authorization (EUA) to treat patients with early, mild-to-moderate COVID-19 who are at high risk of progression. Montefiore Medical Center serves an economically underserved community of >1.4 million residents in the Bronx, New York. Montefiore’s antimicrobial stewardship team (AST) developed a multidisciplinary treatment pathway for patients meeting EUA criteria: (1) outpatients and hospital associates and (2) acute-care patients (EDs or inpatient). Methods: The Montefiore AST established a centralized process for screening high-risk COVID-19 patients 7 days a week. Referrals were sent by e-mail from occupational health, primary care practices, specialty practices, emergency departments, and urgent care centers. Patients were screened in real time and were treated in the ED or a newly established infusion center within 24 hours. After infusion, all patients received phone calls from nurses and had an infectious diseases televisit. Demographics, clinical symptoms, subsequent ED visit or hospital admission, and timing from infusion to ED or hospitalization were obtained from the electronic health record. Results: In total, 281 high-risk patients (median age, 62 years; 57% female) received bamlanivimab at the infusion center or in the acute-care setting between December 2, 2020, and January 27, 2021 (Table 1). The number of treated patients increased weekly (Figure 1). Also, 62% were Hispanic or black, and 96% met EUA criteria. Furthermore, 51 (18%) were referred from occupational health, 205 (73%) were referred from the community, and 25 (9%) were inpatients (https://www.fda.gov/media/143605/download). All patients were successfully infused without adverse reactions. In addition, 23 patients (8.2%) were hospitalized and 6 (2.1%) visited EDs within 30 days of treatment. The average number of days between symptom onset and infusion was 4.9. The median age of admitted versus nonadmitted patients was 68 years versus 61.5 years (P = .07). Conclusions: An AST-coordinated bamlanivimab treatment program successfully treated multiple high-risk COVID-19 patients and potentially reduced hospitalizations. However, the effort, personnel, and resources required are significant. Dedicated hospital investment is necessary for maximal success.
Funding: No
Disclosures: None
Table 1. 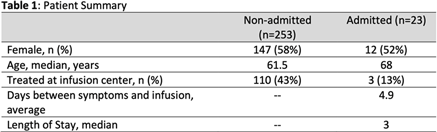
Figure 1.


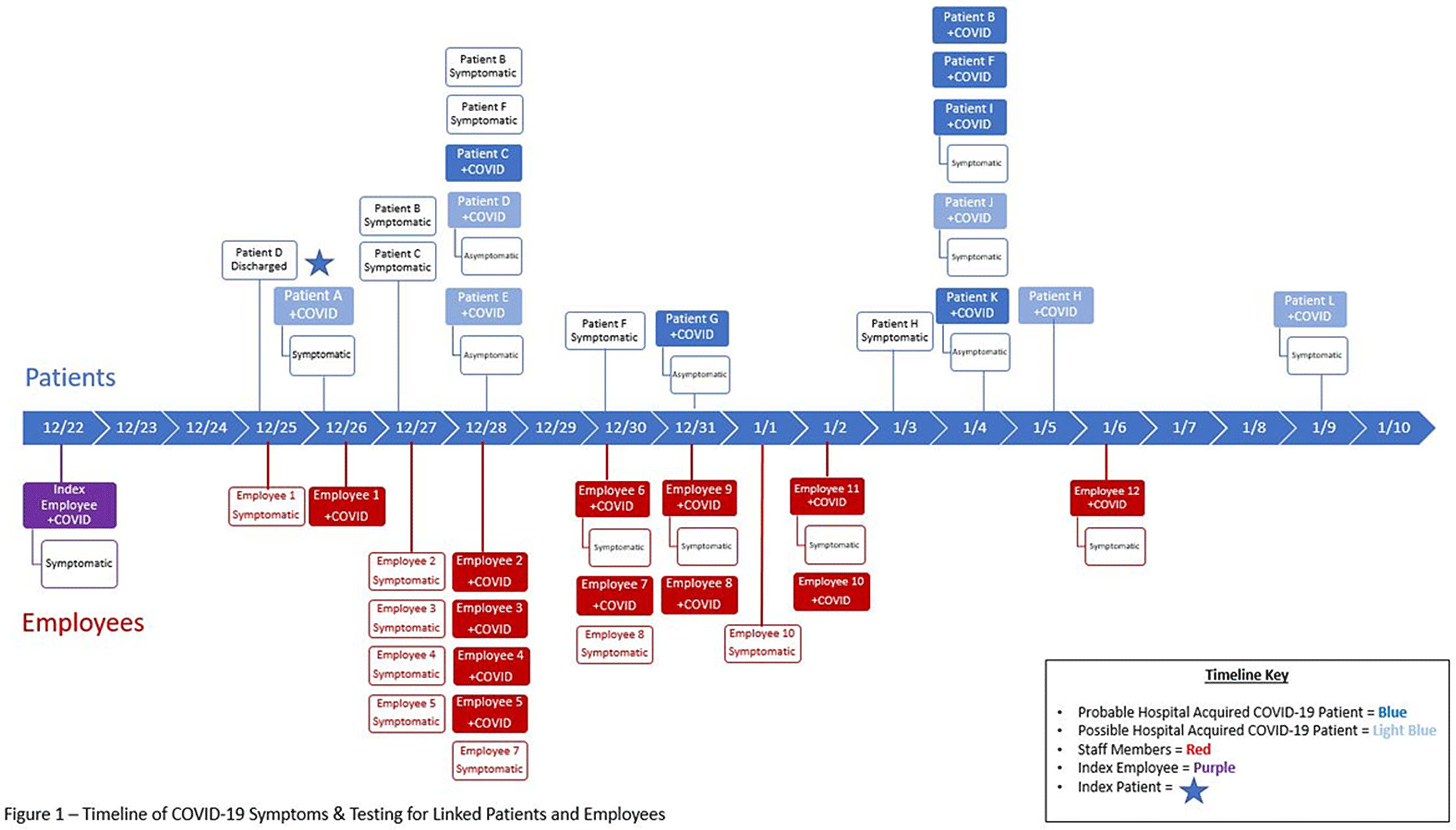
A Cluster of Coronavirus Disease 2019 (COVID-19) Cases on an Inpatient Hospital Unit Involving Multiple Modes of Transmission
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s2-s3
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The Ohio State University Wexner Medical Center identified a cluster of coronavirus disease 2019 (COVID-19) cases on an inpatient geriatric stroke care unit involving both patients and staff. The period of suspected severe acute respiratory coronavirus virus 2 (SARS-CoV-2) transmission and exposure on the unit was December 20, 2020, to January 1, 2021, with some patients and staff developing symptoms and testing positive within the 14 days thereafter. Methods: An epidemiologic investigation was conducted via chart review, staff interviews, and contact tracing to identify potential patient and staff linkages. All staff who worked on the unit were offered testing regardless of the presence of symptoms as well as all patients admitted during the outbreak period. Results: In total, 6 patients likely acquired COVID-19 in the hospital (HCA). An additional 6 patients admitted to the unit during the outbreak period subsequently tested positive but had other possible exposures outside the hospital (Fig. 1). One patient failed to undergo COVID-19 testing on admission but tested positive early in the cluster and is suspected to have contributed to patient to employee transmission. Moreover, 32 employees who worked on the unit in some capacity during this period tested positive, many of whom became symptomatic during their shifts. In addition, 18 employees elected for asymptomatic testing with 3 testing positive; these were included in the total. Some staff also identified potential community exposures. Additionally, staff reported an employee who was working while symptomatic with inconsistent mask use (index employee) early in the outbreak period. The index employee likely contributed to employee transmission but had no direct patient contact. Our epidemiologic investigation ultimately identified 12 employees felt to be linked to transmission based on significant, direct patient care provided to the patients within the outbreak period (Fig. 1). In addition, 3 employees had an exposure outside the hospital indicating likely community transmission. Conclusions: Transmission was felt to be multidirectional and included employee-to-employee, employee-to-patient, and patient-to-employee transmission in the setting of widespread community transmission. Interventions to stop transmission included widespread staff testing, staff auditing regarding temperature and symptom monitoring, and re-education on infection prevention practices. Particular focus was placed on appropriate PPE use including masking and eye protection, hand hygiene, and cleaning and disinfection practices throughout the unit. SARS-CoV-2 admission testing and limited visitation remain important strategies to minimize transmission in the hospital.
Figure 1.
Funding: No
Disclosures: None

Effects of energy balance on appetite and physiological mediators of appetite during strenuous physical activity: secondary analysis of a randomised crossover trial
-
- Journal:
- British Journal of Nutrition / Volume 126 / Issue 10 / 28 November 2021
- Published online by Cambridge University Press:
- 14 January 2021, pp. 1571-1584
- Print publication:
- 28 November 2021
-
- Article
-
- You have access
- HTML
- Export citation
Big Data on BHR: Innovative Approaches to Analysing the Business & Human Rights Resource Centre Database – ERRATUM
-
- Journal:
- Business and Human Rights Journal / Volume 6 / Issue 1 / February 2021
- Published online by Cambridge University Press:
- 09 November 2020, p. 178
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Automorphy lifting for residually reducible
 $l$-adic Galois representations, II
$l$-adic Galois representations, II
- Part of
-
- Journal:
- Compositio Mathematica / Volume 156 / Issue 11 / November 2020
- Published online by Cambridge University Press:
- 15 December 2020, pp. 2399-2422
- Print publication:
- November 2020
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We revisit the paper [Automorphy lifting for residually reducible
 $l$-adic Galois representations, J. Amer. Math. Soc. 28 (2015), 785–870] by the third author. We prove new automorphy lifting theorems for residually reducible Galois representations of unitary type in which the residual representation is permitted to have an arbitrary number of irreducible constituents.
$l$-adic Galois representations, J. Amer. Math. Soc. 28 (2015), 785–870] by the third author. We prove new automorphy lifting theorems for residually reducible Galois representations of unitary type in which the residual representation is permitted to have an arbitrary number of irreducible constituents.


Big Data on BHR: Innovative Approaches to Analysing the Business & Human Rights Resource Centre Database
-
- Journal:
- Business and Human Rights Journal / Volume 6 / Issue 1 / February 2021
- Published online by Cambridge University Press:
- 30 September 2020, pp. 120-126
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Breaking bivariate records
- Part of
-
- Journal:
- Combinatorics, Probability and Computing / Volume 30 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 18 August 2020, pp. 105-123
-
- Article
- Export citation
The Fontan outcomes network: first steps towards building a lifespan registry for individuals with Fontan circulation in the United States – CORRIGENDUM
-
- Journal:
- Cardiology in the Young / Volume 30 / Issue 9 / September 2020
- Published online by Cambridge University Press:
- 30 July 2020, p. 1381
-
- Article
-
- You have access
- HTML
- Export citation
