
219 results
Unintended consequences, conflict and resilience in a small-scale irrigation development, Marakwet, Kenya
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
System fertilization in the pasture phase enhances productivity in integrated crop–livestock systems
-
- Journal:
- The Journal of Agricultural Science / Volume 161 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 14 December 2023, pp. 755-762
-
- Article
-
- You have access
- HTML
- Export citation
Are We Adequately Assessing Delirium? An Analysis Of Liaison Psychiatry Referrals
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S518-S519
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Delirium is characterised by an acute, fluctuating change in cognition, attention and awareness (Wilson et al. Nature Reviews 2020; 6). This presentation can make the diagnosis of delirium extremely challenging to clinicians (Gofton., Canadian Journal of neurological sciences. 2011; 38 673-680). It is commonly reported in hospitalised patients, particularly in those over the age of sixty five (NICE. Delirium: prevention, diagnosis and management. 2010).
ObjectivesOur aim is to identify which investigations and cognitive assessments are completed prior to a referral to the liaison psychiatry services in patients with symptoms of delirium.
MethodsReferrals (N = 6012) to the liaison psychiatry team at Croydon University Hospital made between April and September 2022 were screened. Search parameters used to identify referrals related to a potential diagnosis of delirium were selected by the authors. The terms used were confusion; delirium; agitation; aggression; cognitive decline or impairment; disorientation; challenging behaviour. Data was collected on the completion rates of investigations for delirium as advised by the NICE clinical knowledge summaries. Further data was gathered on neuroimaging (CT or MRI), cognitive assessment tools (MOCA/MMSE) and delirium screening tools (4AT/AMTS).
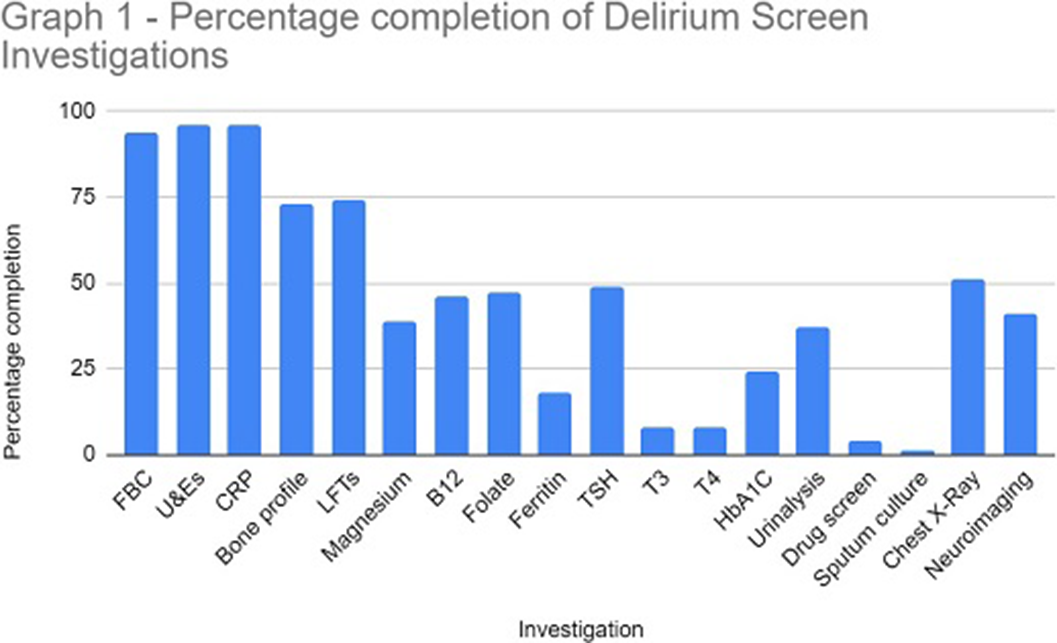
ResultsThe study sample identified 114 referrals (61 males and 53 females), with 82% over 65 years at the time of referral. In 96% of referrals, U&E and CRP were performed. Sputum culture (1%), urine toxin screen (4%) and free T3/4 (8%) were the tests utilised the least. Neuroimaging was completed in 41% of referrals (see Graph 1 for a full breakdown of results).
A formal cognitive assessment or delirium screening tool was completed in 32% of referrals. The AMTS and 4AT tools were documented for 65% and 24% respectively. A total of 19 referrals explicitly stated the patient was suspected to have dementia. A delirium screening tool was documented in 47% of these cases however, a formal cognitive assessment was documented in only 5% of these patients.
Following psychiatric assessment 47% of referrals were confirmed as delirium.
Image:
 Conclusions
ConclusionsOur data highlights the low level completion of the NICE recommended delirium screen prior to referral to liaison psychiatry. The effective implementation of a delirium screen and cognitive assessment is paramount to reduce the number of inappropriate psychiatric referrals in hospital and helps to identify reversible organic causes of delirium. This in turn will ensure timely treatment of reversible causes of delirium and reduce the length of hospital admission.
Disclosure of InterestNone Declared

Risk and resilience factors for psychopathology during pregnancy: An application of the Hierarchical Taxonomy of Psychopathology (HiTOP)
-
- Journal:
- Development and Psychopathology / Volume 36 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 03 February 2023, pp. 545-561
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Depression, anxiety and PTSD symptoms before and during the COVID-19 pandemic in the UK
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 12 / September 2023
- Published online by Cambridge University Press:
- 26 July 2022, pp. 5428-5441
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations between unpasteurised camel and other milk consumption, livestock ownership, and self-reported febrile and gastrointestinal symptoms among semi-pastoralists and pastoralists in the Somali Region of Ethiopia
- Part of
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 02 May 2022, e44
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Seed-shattering phenology at soybean harvest of economically important weeds in multiple regions of the United States. Part 3: Drivers of seed shatter
-
- Journal:
- Weed Science / Volume 70 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 15 November 2021, pp. 79-86
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outcomes of clinical decision support for outpatient management of Clostridioides difficile infection
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 29 September 2021, pp. 1345-1348
- Print publication:
- October 2022
-
- Article
- Export citation
The MAGPI survey: Science goals, design, observing strategy, early results and theoretical framework
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 38 / 2021
- Published online by Cambridge University Press:
- 26 July 2021, e031
-
- Article
-
- You have access
- HTML
- Export citation
-
We present an overview of the Middle Ages Galaxy Properties with Integral Field Spectroscopy (MAGPI) survey, a Large Program on the European Southern Observatory Very Large Telescope. MAGPI is designed to study the physical drivers of galaxy transformation at a lookback time of 3–4 Gyr, during which the dynamical, morphological, and chemical properties of galaxies are predicted to evolve significantly. The survey uses new medium-deep adaptive optics aided Multi-Unit Spectroscopic Explorer (MUSE) observations of fields selected from the Galaxy and Mass Assembly (GAMA) survey, providing a wealth of publicly available ancillary multi-wavelength data. With these data, MAGPI will map the kinematic and chemical properties of stars and ionised gas for a sample of 60 massive (
 ${>}7 \times 10^{10} {\mathrm{M}}_\odot$
) central galaxies at
${>}7 \times 10^{10} {\mathrm{M}}_\odot$
) central galaxies at  $0.25 < z <0.35$
in a representative range of environments (isolated, groups and clusters). The spatial resolution delivered by MUSE with Ground Layer Adaptive Optics (
$0.25 < z <0.35$
in a representative range of environments (isolated, groups and clusters). The spatial resolution delivered by MUSE with Ground Layer Adaptive Optics ( $0.6-0.8$
arcsec FWHM) will facilitate a direct comparison with Integral Field Spectroscopy surveys of the nearby Universe, such as SAMI and MaNGA, and at higher redshifts using adaptive optics, for example, SINS. In addition to the primary (central) galaxy sample, MAGPI will deliver resolved and unresolved spectra for as many as 150 satellite galaxies at
$0.6-0.8$
arcsec FWHM) will facilitate a direct comparison with Integral Field Spectroscopy surveys of the nearby Universe, such as SAMI and MaNGA, and at higher redshifts using adaptive optics, for example, SINS. In addition to the primary (central) galaxy sample, MAGPI will deliver resolved and unresolved spectra for as many as 150 satellite galaxies at  $0.25 < z <0.35$
, as well as hundreds of emission-line sources at
$0.25 < z <0.35$
, as well as hundreds of emission-line sources at  $z < 6$
. This paper outlines the science goals, survey design, and observing strategy of MAGPI. We also present a first look at the MAGPI data, and the theoretical framework to which MAGPI data will be compared using the current generation of cosmological hydrodynamical simulations including EAGLE, Magneticum, HORIZON-AGN, and Illustris-TNG. Our results show that cosmological hydrodynamical simulations make discrepant predictions in the spatially resolved properties of galaxies at
$z < 6$
. This paper outlines the science goals, survey design, and observing strategy of MAGPI. We also present a first look at the MAGPI data, and the theoretical framework to which MAGPI data will be compared using the current generation of cosmological hydrodynamical simulations including EAGLE, Magneticum, HORIZON-AGN, and Illustris-TNG. Our results show that cosmological hydrodynamical simulations make discrepant predictions in the spatially resolved properties of galaxies at  $z\approx 0.3$
. MAGPI observations will place new constraints and allow for tangible improvements in galaxy formation theory.
$z\approx 0.3$
. MAGPI observations will place new constraints and allow for tangible improvements in galaxy formation theory.






Role of age, gender and marital status in prognosis for adults with depression: An individual patient data meta-analysis
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 30 / 2021
- Published online by Cambridge University Press:
- 04 June 2021, e42
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The treatment gap for mental disorders in adults enrolled in HIV treatment programmes in South Africa: a cohort study using linked electronic health records
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 30 / 2021
- Published online by Cambridge University Press:
- 17 May 2021, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Turbulent impurity transport simulations in Wendelstein 7-X plasmas
- Part of
-
- Journal:
- Journal of Plasma Physics / Volume 87 / Issue 1 / February 2021
- Published online by Cambridge University Press:
- 02 February 2021, 855870103
-
- Article
- Export citation
Seed-shattering phenology at soybean harvest of economically important weeds in multiple regions of the United States. Part 1: Broadleaf species
-
- Journal:
- Weed Science / Volume 69 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 04 November 2020, pp. 95-103
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Seed-shattering phenology at soybean harvest of economically important weeds in multiple regions of the United States. Part 2: Grass species
-
- Journal:
- Weed Science / Volume 69 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 26 October 2020, pp. 104-110
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Validation and calibration of the Eating Assessment in Toddlers FFQ (EAT FFQ) for children, used in the Growing Up Milk – Lite (GUMLi) randomised controlled trial
-
- Journal:
- British Journal of Nutrition / Volume 125 / Issue 2 / 28 January 2021
- Published online by Cambridge University Press:
- 17 August 2020, pp. 183-193
- Print publication:
- 28 January 2021
-
- Article
-
- You have access
- HTML
- Export citation
Impact of unit-specific metrics and prescribing tools on a family medicine ward
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 11 / November 2020
- Published online by Cambridge University Press:
- 01 July 2020, pp. 1272-1278
- Print publication:
- November 2020
-
- Article
- Export citation
The Role of Zinc in Depressed Pregnant and Non-Pregnant Women: A Systematic Review and Meta-Analysis
-
- Journal:
- Proceedings of the Nutrition Society / Volume 79 / Issue OCE2 / 2020
- Published online by Cambridge University Press:
- 10 June 2020, E542
-
- Article
-
- You have access
- Export citation
Documentation of acute change in mental status in nursing homes highlights opportunity to augment infection surveillance criteria
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 7 / July 2020
- Published online by Cambridge University Press:
- 28 April 2020, pp. 848-850
- Print publication:
- July 2020
-
- Article
- Export citation
PKS 2250–351: A giant radio galaxy in Abell 3936
- Part of
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 37 / 2020
- Published online by Cambridge University Press:
- 25 March 2020, e013
-
- Article
-
- You have access
- HTML
- Export citation
-
We present a detailed analysis of the radio galaxy PKS
 $2250{-}351$
, a giant of 1.2 Mpc projected size, its host galaxy, and its environment. We use radio data from the Murchison Widefield Array, the upgraded Giant Metre-wavelength Radio Telescope, the Australian Square Kilometre Array Pathfinder, and the Australia Telescope Compact Array to model the jet power and age. Optical and IR data come from the Galaxy And Mass Assembly (GAMA) survey and provide information on the host galaxy and environment. GAMA spectroscopy confirms that PKS
$2250{-}351$
, a giant of 1.2 Mpc projected size, its host galaxy, and its environment. We use radio data from the Murchison Widefield Array, the upgraded Giant Metre-wavelength Radio Telescope, the Australian Square Kilometre Array Pathfinder, and the Australia Telescope Compact Array to model the jet power and age. Optical and IR data come from the Galaxy And Mass Assembly (GAMA) survey and provide information on the host galaxy and environment. GAMA spectroscopy confirms that PKS  $2250{-}351$
lies at
$2250{-}351$
lies at  $z=0.2115$
in the irregular, and likely unrelaxed, cluster Abell 3936. We find its host is a massive, ‘red and dead’ elliptical galaxy with negligible star formation but with a highly obscured active galactic nucleus dominating the mid-IR emission. Assuming it lies on the local M–
$z=0.2115$
in the irregular, and likely unrelaxed, cluster Abell 3936. We find its host is a massive, ‘red and dead’ elliptical galaxy with negligible star formation but with a highly obscured active galactic nucleus dominating the mid-IR emission. Assuming it lies on the local M– $\sigma$
relation, it has an Eddington accretion rate of
$\sigma$
relation, it has an Eddington accretion rate of  $\lambda_{\rm EDD}\sim 0.014$
. We find that the lobe-derived jet power (a time-averaged measure) is an order of magnitude greater than the hotspot-derived jet power (an instantaneous measure). We propose that over the lifetime of the observed radio emission (
$\lambda_{\rm EDD}\sim 0.014$
. We find that the lobe-derived jet power (a time-averaged measure) is an order of magnitude greater than the hotspot-derived jet power (an instantaneous measure). We propose that over the lifetime of the observed radio emission ( ${\sim} 300\,$
Myr), the accretion has switched from an inefficient advection-dominated mode to a thin disc efficient mode, consistent with the decrease in jet power. We also suggest that the asymmetric radio morphology is due to its environment, with the host of PKS
${\sim} 300\,$
Myr), the accretion has switched from an inefficient advection-dominated mode to a thin disc efficient mode, consistent with the decrease in jet power. We also suggest that the asymmetric radio morphology is due to its environment, with the host of PKS  $2250{-}351$
lying to the west of the densest concentration of galaxies in Abell 3936.
$2250{-}351$
lying to the west of the densest concentration of galaxies in Abell 3936.







