
127 results
Comparisons between dual-energy X-ray absorptiometry and bioimpedance devices for appendicular lean mass and muscle quality in Hispanic adults
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 12 / 28 June 2024
- Published online by Cambridge University Press:
- 15 April 2024, pp. 2031-2038
- Print publication:
- 28 June 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Random pinhole attenuator for high-power laser beams
-
- Journal:
- High Power Laser Science and Engineering / Volume 12 / 2024
- Published online by Cambridge University Press:
- 01 April 2024, e34
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
P86: Effect of Virtual Reality on Stress Reduction and Change of Physiological Parameters Including Heart Rate Variability in People With High Stress: An Open Randomized Crossover Trial
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 129-130
-
- Article
-
- You have access
- Export citation
PP50 Early Diagnosis Effect Of Newborns With Critical Congenital Heart Disease Using National Health Insurance Data In South Korea
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 39 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 14 December 2023, p. S66
-
- Article
-
- You have access
- Export citation
PP122 The Feasibility Assessment For Domestic Introduction Of Newborn Pulse Oximetry Screening For Critical Congenital Heart Disease
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 39 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 14 December 2023, p. S84
-
- Article
-
- You have access
- Export citation
Comparison of Perceived Importance and Performance of Community Pharmacists’ Role in South Korea During the Coronavirus Disease 2019 Pandemic
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 04 December 2023, e569
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Application of Deep Learning to Solar and Space Weather Data
-
- Journal:
- Proceedings of the International Astronomical Union / Volume 18 / Issue S372 / August 2022
- Published online by Cambridge University Press:
- 28 September 2023, pp. 131-149
- Print publication:
- August 2022
-
- Article
- Export citation
Outbreak of COVID-19 among children and young adults in a cancer centre daycare unit
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 21 February 2022, e40
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The impact of the COVID-19 pandemic on depression in community-dwelling older adults: a prospective cohort study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 7 / May 2023
- Published online by Cambridge University Press:
- 17 December 2021, pp. 2992-2999
-
- Article
- Export citation
Impact of data extraction errors in meta-analyses on the association between depression and peripheral inflammatory biomarkers: an umbrella review
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 5 / April 2023
- Published online by Cambridge University Press:
- 09 November 2021, pp. 2017-2030
-
- Article
- Export citation
Manufacturers’ perceptions of the decision-making process for new drug reimbursement in South Korea
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 37 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 17 September 2021, e88
-
- Article
- Export citation
Differences in the Clinical Outcome of Community-Acquired APN According to the Appropriateness of Antibiotic Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s6
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The purpose of this study was to find out the relationship between appropriateness of antibiotic prescription and clinical outcomes in patients with community-acquired acute pyelonephritis (CA-APN). Methods: A multicenter prospective cohort study was performed in 8 Korean hospitals from September 2017 to August 2018. All hospitalized patients aged ≥19 years diagnosed with CA-APN at admission were recruited. Pregnant women and patients with insufficient data were excluded. In addition, patients with prolonged hospitalization due to medical problems that were not associated with APN treatment were excluded. The appropriateness of empirical and definitive antibiotics was divided into “optimal,” “suboptimal,” and “inappropriate,” and optimal and suboptimal were regarded as appropriate antibiotic use. The standard for the classification of empirical antibiotics was defined reflecting the Korean national guideline for the antibiotic use in urinary tract infection 2018. The standards for the classification of definitive antibiotics were defined according to the result of in vitro susceptibility tests of causative organisms. Clinical outcomes including clinical failure (mortality or recurrence) rate, hospitalization days, and medical costs were compared between patients who were prescribed antibiotics appropriately and those who were prescribed them inappropriately. Results: In total, 397 and 318 patients were eligible for the analysis of the appropriateness of empirical and definitive antibiotics, respectively. Of these, 10 (2.5%) and 18 (5.7%) were inappropriately prescribed empirical and definitive antibiotics, respectively, and 28 (8.8%) were prescribed either empirical or definitive antibiotics inappropriately. Patients who were prescribed empirical antibiotics appropriately showed a lower mortality rate (0 vs 10%; P = .025), shorter hospitalization days (9 vs 12.5 days; P = .014), and lower medical costs (US$2,333 vs US$4,531; P = .007) compared to those who were prescribed empirical antibiotics “inappropriately.” In comparison, we detected no significant differences in clinical outcomes between patients who were prescribed definitive antibiotics appropriately and those who were prescribed definitive antibiotics inappropriately. Patients who were prescribed both empirical and definitive antibiotics appropriately showed a lower clinical failure rate (0.3 vs 7.1%; P = .021) and shorter hospitalization days (9 vs 10.5 days; P = .041) compared to those who were prescribed either empirical or definitive antibiotics inappropriately. Conclusions: Appropriate use of antibiotics leads patients with CA-APN to better clinical outcomes including fewer hospitalization days and lower medical costs.
Funding: No
Disclosures: None
Table 1. 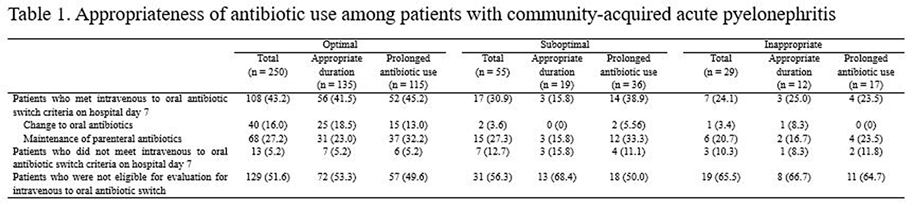
Table 2. 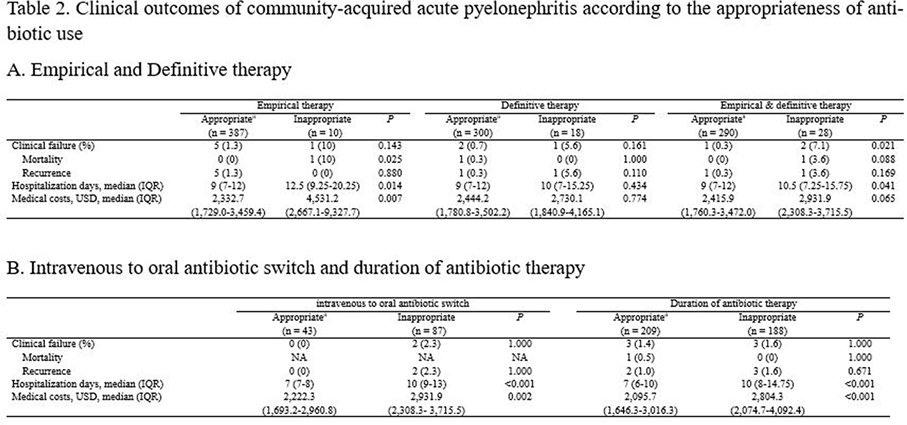


Clinical impact of early reinsertion of a central venous catheter after catheter removal in patients with catheter-related bloodstream infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 2 / February 2021
- Published online by Cambridge University Press:
- 09 September 2020, pp. 162-168
- Print publication:
- February 2021
-
- Article
- Export citation
Imperatives of Care: Women and Medicine in Colonial Korea. By Sonja M. Kim. Honolulu: University of Hawai‘i Press, 2019. 232 pp. ISBN: 9780824855451 (cloth).
-
- Journal:
- The Journal of Asian Studies / Volume 79 / Issue 3 / August 2020
- Published online by Cambridge University Press:
- 05 October 2020, pp. 780-781
- Print publication:
- August 2020
-
- Article
- Export citation
Whole-genome sequencing combined with a case-control study of an outbreak of staphylococcal food-poisoning
-
- Journal:
- Epidemiology & Infection / Accepted manuscript
- Published online by Cambridge University Press:
- 20 May 2020, pp. 1-16
-
- Article
-
- You have access
- Export citation
The Differential Cognitive Deficits Between Patients with Early Stage Alzheimer's Disease and Patients with Early Stage Vascular Dementia
-
- Journal:
- European Psychiatry / Volume 41 / Issue S1 / April 2017
- Published online by Cambridge University Press:
- 23 March 2020, p. S175
-
- Article
-
- You have access
- Export citation
Preserved Serotonergic Activity in Early-Onset Parkinson’s Disease
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 47 / Issue 3 / May 2020
- Published online by Cambridge University Press:
- 05 November 2019, pp. 344-349
-
- Article
-
- You have access
- HTML
- Export citation
Effects of a Korean version of the metacognitive training program for outpatients with schizophrenia on theory of mind, positive symptoms, and interpersonal relationships
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 48 / Issue 1 / January 2020
- Published online by Cambridge University Press:
- 18 October 2019, pp. 14-24
- Print publication:
- January 2020
-
- Article
- Export citation
Alexithymia and frontal–amygdala functional connectivity in North Korean refugees
-
- Journal:
- Psychological Medicine / Volume 50 / Issue 2 / January 2020
- Published online by Cambridge University Press:
- 12 February 2019, pp. 334-341
-
- Article
-
- You have access
- HTML
- Export citation
Looking backward through the looking glass: Reference groups and social comparison
-
- Journal:
- Journal of Management & Organization / Volume 26 / Issue 1 / January 2020
- Published online by Cambridge University Press:
- 05 November 2018, pp. 110-131
-
- Article
- Export citation
