
84 results
Synthesis and Characterization of Montmorillonite-Supported Tio2 Composites for Enhanced UV Absorption
-
- Journal:
- Clays and Clay Minerals / Volume 68 / Issue 6 / December 2020
- Published online by Cambridge University Press:
- 01 January 2024, pp. 533-543
-
- Article
- Export citation
The biological standard of living of Korean men under Confucianism, colonialism, capitalism, and communism
-
- Journal:
- Journal of Biosocial Science / Volume 56 / Issue 3 / May 2024
- Published online by Cambridge University Press:
- 29 November 2023, pp. 413-425
-
- Article
- Export citation
Against Defending Science: Asking Better Questions About Indigenous Knowledge and Science
-
- Journal:
- Philosophy of Science ,
- Published online by Cambridge University Press:
- 23 October 2023, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Seroprevalence of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) antibodies among healthcare personnel in the Midwestern United States, September 2020–April 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 04 August 2023, e133
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of patient beliefs regarding the need for antibiotics and prescribing outcomes on patient satisfaction in urgent-care settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 26 April 2023, e83
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Safety Outcomes of Selective Serotonin Reuptake Inhibitors in Adolescent Attention-Deficit/Hyperactivity Disorder with Comorbid Depression: The ASSURE Study – CORRIGENDUM
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 10 / July 2023
- Published online by Cambridge University Press:
- 20 April 2023, p. 4831
-
- Article
-
- You have access
- HTML
- Export citation
Excessive Daytime Sleepiness in a Real-World Study of Participants With OSA With or Without Comorbid Depression
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 2 / April 2023
- Published online by Cambridge University Press:
- 14 April 2023, p. 231
-
- Article
-
- You have access
- Export citation
Comorbidities and Presenting Symptoms in a Real-World Population With Obstructive Sleep Apnea
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 2 / April 2023
- Published online by Cambridge University Press:
- 14 April 2023, pp. 230-231
-
- Article
-
- You have access
- Export citation
Personal protective equipment use among dental healthcare personnel during the coronavirus disease 2019 (COVID-19) pandemic and the impact of an educational video in clinical practice
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 16 March 2023, pp. 1472-1480
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Safety outcomes of selective serotonin reuptake inhibitors in adolescent attention-deficit/hyperactivity disorder with comorbid depression: the ASSURE study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 10 / July 2023
- Published online by Cambridge University Press:
- 20 February 2023, pp. 4811-4819
-
- Article
- Export citation
Ways to Suppress Electron Beam Damage Using High-Speed Electron Beam Control by Electrostatic Shutter in Sample Observation and Analysis
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2200-2201
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Morphology and Growth Habit of a Novel Flux-Grown Layered Semiconductor KBiS2 Revealed by Lab-based Diffraction-Contrast Tomography
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 278-279
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Chapter 60 - Caregiving
- from Section IV - Principles of Care for the Elderly
-
-
- Book:
- Reichel's Care of the Elderly
- Published online:
- 30 June 2022
- Print publication:
- 21 July 2022, pp 727-735
-
- Chapter
- Export citation
Fluidic operation of a polymer-based nanosensor chip for analysing single molecules
-
- Journal:
- Flow: Applications of Fluid Mechanics / Volume 2 / 2022
- Published online by Cambridge University Press:
- 27 June 2022, E14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antibodies in healthcare personnel following severe acute respiratory syndrome coronavirus virus 2 (SARS-CoV-2) infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 15 June 2022, e93
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Dynamic networks of psychological symptoms, impairment, substance use, and social support: The evolution of psychopathology among emerging adults
- Part of
-
- Journal:
- European Psychiatry / Volume 65 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 13 June 2022, e32
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Rapid streptococcal pharyngitis testing and antibiotic prescribing before and during the COVID-19 pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s20-s21
-
- Article
-
- You have access
- Open access
- Export citation
-
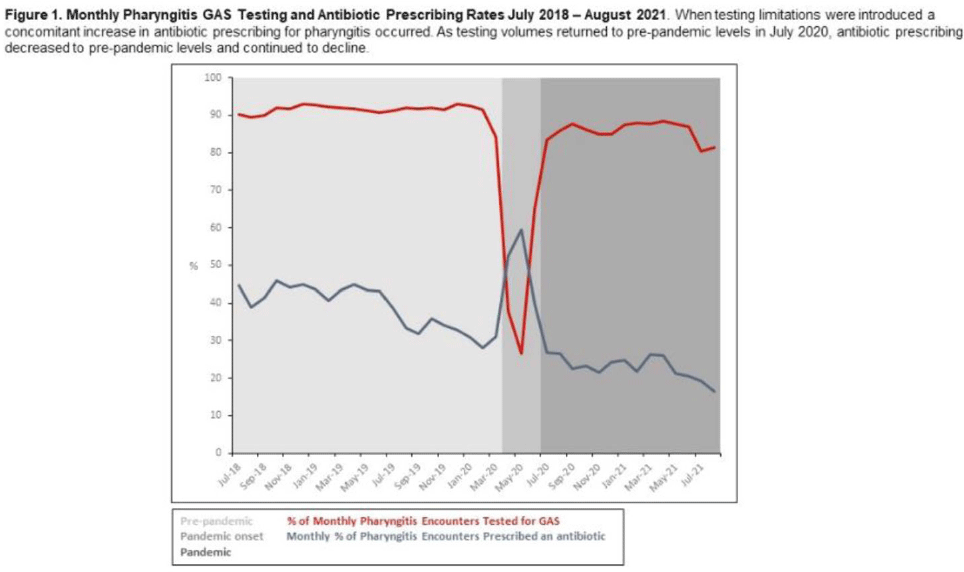
Background: Pharyngitis is 1 of the most common conditions leading to inappropriate antibiotic prescriptions. When personal protective equipment (PPE) was at first constrained during the COVID-19 pandemic, Intermountain Healthcare recommended limiting rapid group A streptococcal pharyngitis (GAS) testing in urgent-care clinics to preserve PPE. Notably, the percentage of pharyngitis encounters prescribed an antibiotic and that underwent GAS testing is a key Healthcare Effectiveness Data and Information Set (HEDIS) measure. We have described our experience with urgent-care pharyngitis encounters and the impact of temporarily reducing GAS testing on antibiotic prescribing before and during the COVID19 pandemic. Method: We identified all urgent care encounters between July 2018 and August 2021 associated with a primary diagnosis of pharyngitis using ICD-10 CM codes and a validated methodology. Pharyngitis encounters were assessed for antibiotic prescriptions ordered through the electronic health record (EHR) and the use of point-of-care rapid GAS tests. Pharyngitis encounters were analyzed monthly. We assessed the percentage of encounters associated with an antibiotic prescription regardless of testing and the percentage of encounters associated with an antibiotic prescription when a GAS test was or was not performed. We examined 3 periods relating to COVID-19 and GAS testing recommendations: the prepandemic period (July 2018–March 2020), the pandemic onset period (April 2020–June 2020), and the pandemic period (July 2020–August 2021). Results: Prior to the pandemic, the monthly percentage of pharyngitis encounters for which rapid GAS testing was performed was nearly 90% (Fig. 1). The average monthly percentage of urgent-care pharyngitis encounters prescribed an antibiotic was 38.9%, and the average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing was 90.4%. This HEDIS measure declined from 90.4% during the prepandemic period to 29.8% in the pandemic onset period when GAS testing was limited. Following resumption of routine testing practices the monthly percentage of urgent-care pharyngitis encounters for which rapid GAS testing was performed returned to levels ≥80% by July 2020 (Fig. 1). The average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing rose to 87.3% during this period. Conclusions: Limited PPE in our urgent care centers during the initial months of the COVID-19 pandemic was associated with a mandated substantial decline in rapid GAS testing. As testing volume decreased, we noted a simultaneous relative increase of >30% in antibiotic prescribing for pharyngitis. These findings suggest that rapid streptococcal testing promotes appropriate antibiotic prescribing.
Funding: None
Disclosures: None

Rapid streptococcal pharyngitis testing and antibiotic prescribing before and during the coronavirus disease 2019 (COVID-19) pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 10 May 2022, e80
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Right Accounting of Wrongs: Examining Temporal Changes to Human Rights Monitoring and Reporting
-
- Journal:
- British Journal of Political Science / Volume 53 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 07 February 2022, pp. 163-182
- Print publication:
- January 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prehospital Ketamine Administration for Excited Delirium with Illicit Substance Co-Ingestion and Subsequent Intubation in the Emergency Department
-
- Journal:
- Prehospital and Disaster Medicine / Volume 36 / Issue 6 / December 2021
- Published online by Cambridge University Press:
- 23 September 2021, pp. 697-701
- Print publication:
- December 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
