
10065 results in Prehospital and Disaster Medicine
EMT Response in COVID-19 Pandemic: Best Practices from Deployment of UK-MED and PCPM’s EMTs
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s52
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
What Happens After They All Go? Addressing the Gap between Field Hospital Departure and Restoration of Local Health Facilities Following Sudden-Onset Disasters
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s76
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
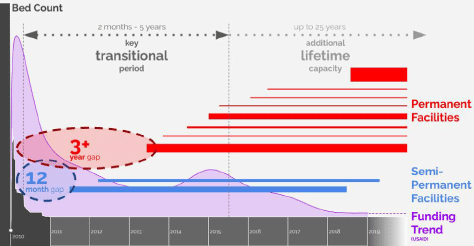
Field hospitals present an attractive solution for Emergency Medical Teams due to their portability and ease of assembly, yet are generally designed to be temporary, often leading to a gap until permanent facilities are restored after a sudden-onset disaster.
Objectives:The objective of this paper is to understand the duration of field hospitals deployed to the 2010 Haiti Earthquake, identify the time taken to re-open permanent facilities, and propose approaches to better address this gap.
Method/Description:Following a review of field hospital typologies and standards, a comparative study was conducted of five key field hospitals deployed to Haiti. Quantitative data from in-house reports, limited available studies, and mapping exercises were complemented with qualitative findings through interviews with key personnel. Additional data were collected for another 21 field hospitals, confirming the rough duration of 26 of the total 44 field hospitals deployed for Haiti. This was compared against information available on the re-opening of major permanent health care facilities.
Results/Outcomes:The results indicated most field hospitals were decommissioned after two-to-six months. Some semi-permanent facilities opened in their wake, but not until 18-24 months. Permanent facilities started re-opening after approximately four years, however the main 500 bed hospital did not fully re-open until almost 10 years after the disaster.
Conclusion:Provision of more durable, semi-permanent structures during early relief stages could better capture the initial funding impulse as well as reduce the gap of bed numbers as field hospitals reach the limit of their viable lifespan, lasting until more permanent facilities are re-opened often many years later.
Tables and Figures (optional)

Optimization of Patient Flow through EMT Facilities Applying Dynamic Behavioral Simulation Models
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s66
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
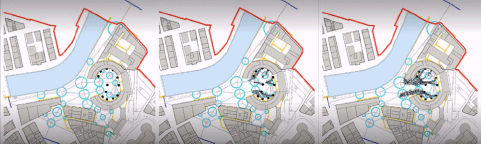
The effectiveness of care provided by EMTs is directly linked to the ability to ensure a controlled, coordinated, and safe patient flow through the post, especially in case of MCIs or disease outbreak. Currently, there are neither frameworks nor tools to analyze such flow that is often visualized on paper using arrows or simply connected to the care pathway, thus missing the impact of people’s interactions with the facility.
Objectives:This study aims at exploring the use of a behavioral-design-based approach in simulating patient flow through EMTs.1
Method/Description:It provides a dynamic behavioral simulation model to assess the interactions between patients, staff members, and the related dynamic movements/interactions with the health care facility, each of them having specific features also in relation to the emergency condition faced.2 Data used in this study consist of literature-based information concerning patient characteristics (eg, age), the variation of expected medical conditions and severity in relation to the time and typology of the emergency,3 layouts of existing facilities (eg, UKMed T1), and experimental activities (eg, exercise).
Results/Outcomes:The analysis of the results will allow to simulate different scenarios and improve the design of health care facilities layouts in order to prevent overcrowding situation, avoid disease spreading, estimate the optimal number of staff for each task, and investigate interactions between patients and staff.
Conclusion:Optimizing patient flow encompasses quickly, efficiently, and effectively movement meeting the demand for care by moving patients through care pathways while improving coordination of care, patient safety, and health outcomes.

I’M HERE: IMproving HEalth Communication in REfugee Camps
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s101
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
EMT2-ITA Regione Piemonte Greening Initiatives for Building Climate Resilient Field Hospital
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s54
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Adapting In-Person National Emergency Medical Teams (EMT) Introductory Training to a Virtual, Storytelling (Talanoa) Format for Pacific Island Countries and Areas (PICs)
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s90
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Use of Mobile Health Units in Natural Disasters – A Scoping Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s88
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Establishing an Emergency Medical Team in LMIC Setup; Experience from Ethiopia’s Challenges and Opportunity
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s67
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
Natural and man-made catastrophes have caused significant destruction and loss of lives throughout human history. Disasters accompany various events with multiple causes and consequences, often leading to a cascade of health-related events. Ethiopia, amongst the developing countries in the horn of Africa, is vulnerable to natural and man-made disasters. Over the last few years, Ethiopia learned the hardest way to transform its disaster management from a mere apparatus of response and recovery to preparedness and mitigation.
Objectives:Review the challenges and opportunities for establishing the Ethiopian EMT and its disaster response experience.
Method/Description:This was a mixed-methods, cross-sectional Intra-Action Review of activities of country EMT. It included a review of documents and key informant interviews. All data were analyzed thematically.
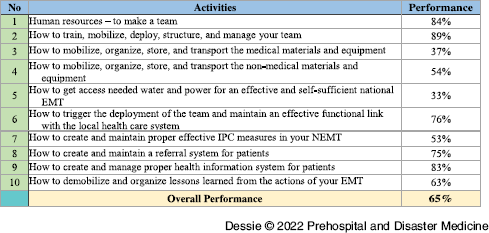
Results/Outcomes:In May 2022, the Ethiopian Federal MOH, in collaboration with WHO, adapted the WHO EMT initiative to tackle the identified challenges. Ethiopia’s EMT implementation plan was created, which included ten steps and 50 detailed activities. This initiative aims to have a classified Type I fixed EMT in the coming six months. Based on the objective evaluation of the last four months’ performance toward plan implementation, activities show that 65% of the overall plan has been completed.
Conclusion:Implementing the EMT initiative in Ethiopia has positively impacted the clinical quality of care, enhanced coordination, and improved health outcomes for the population served at times of great need. However, the implementation requires collaboration in support, guidance, and experience sharing from stakeholders and partners, including twinning with other organizations.
Tables and Figures (optional)
Table 1. Ethiopian EMT Ten Steps Implementation

Establishing a National Emergency Medical Team (EMT) in Papua New Guinea (PNG)
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s59
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Fiji Emergency Medical Assistance Team’s (FEMAT) Response to Tropical Cyclone Yasa, Fiji
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s94
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
A T2 Translational Science Modified Delphi Study: Spinal Motion Restriction in a Resource-Scarce Environment
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s70
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
Emerging evidence is guiding changes in prehospital management of potential spinal injuries. The majority of settings related to current recommendations are in resource-rich environments. Whereas there is a lack of guidance on the provision of spinal motion restriction (SMR) in resource-scarce environments (RSE).
Objectives:What is appropriate SMR in RSE?
Method/Description:The first round of this Modified Delphi (mD) study was a structured focus group. The result of the focus group discussion of open-ended questions produced ten statements that were added to ten statements derived from Fischer (2018) to create the 20 mD statements presented to the experts.
Experts rated their agreement with each statement on a scale from one to seven. Consensus amongst experts was defined as SD≤1.0. Statements that were in agreement reaching consensus were included in the final report. Those not reaching consensus advanced to the next mD round.
For these subsequent rounds, experts were shown the mean response and their own response for each of the remaining statements and asked to reconsider their rating. As above, those that did not reach consensus advanced to the next round until consensus was reached for each statement.
Results/Outcomes:Twenty-two experts completed the first mD round, 19 completed the second mD round, and 16 completed the third mD round. Eleven statements reached consensus (Table 1). Nine statements did not reach consensus (Table 2).
Conclusion:Experts reached consensus offering 11 statements to be incorporated into the creation of SMR clinical guidelines in RSE.
Tables and Figures (optional)
Table 1. 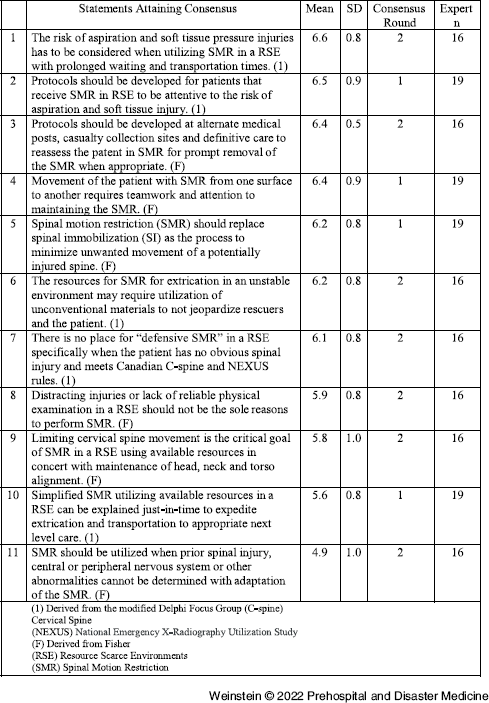
Table 2. 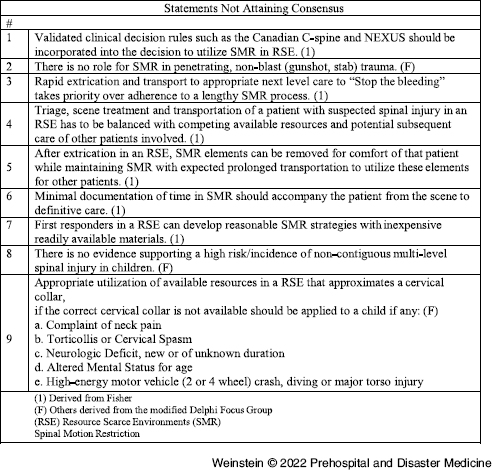


The Taal Volcano Eruption and Landfall of Super Typhoon Odette: A Dilogy of Disasters in the Philippines, An Abstract on the Response Strategies of Dr. Jose N. Rodriguez Memorial Hospital and Sanitarium-Philippine Emergency Medical Assistance Team (DJNRMHS PEMAT) for the TAAL and DINAGAT Missions in the Years 2020 and 2021
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s92
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Team Well-Being and Challenges of Deploying an EMT Halfway Around the World
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s97
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Investigation of the Receiving United States National Disaster Medical System (NDMS) Disaster Medical Assistant Team (DMAT) in Japan: Development of Standard Operation Procedures for Receiving International Medical Teams
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s63
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Stress and Burnout Levels among Emergency Medical Technicians Working during COVID-19 Pandemic: A Cross-Sectional Study in Spain
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s77
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
Among all health care workers, EMTs have played a notable role during COVID-19; working as a frontline, they faced many challenges, including working overload and an extremely cautious environment that requires a rapid and precise response, which led to experiencing higher severity of mental health symptoms.
Objectives:To explore the association between stress and burnout among EMTs while working during the COVID-19 pandemic.
Method/Description:A cross-sectional quantitative study with a descriptive design. It was conducted from March-April 2021 on 280 Spanish EMTs, using an online survey of 42 items about workload and working conditions during COVID-19 and other variables specific to COVID-19. The Perceived Stress Scale (PSS), Maslach Burnout Inventory (MBI), and Pearson’s correlation coefficient were used to determine the relationships between the variables.
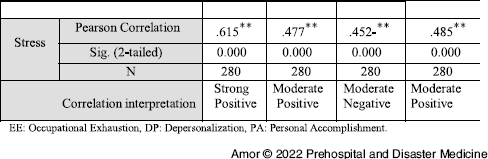
Results/Outcomes:The study revealed a moderate positive correlation between the perceived level of stress and burnout among the EMTs. Specifically, findings showed a strong positive correlation between stress and EE (0.62) and a moderate positive correlation with DP (0.48). However, it found a moderate negative correlation between the level of stress and the third subdimension of burnout, PA (0.45), where the increase in the stress level correlated with a decrease in PA of the EMTs.
Conclusion:Burnout might be related to the persistent stress of the EMTs working during the COVID-19 pandemic, considering their work conditions and the socio-demographic variables. The mental health of the first responders is crucial, as it influences their achievement and works satisfaction, and it might affect the quality of the service they provide.
Tables and Figures (optional)
Table 1. Pearson Correlation: Correlation between the Stress and Burnout among the Emergency Medical Technicians (n = 280)

The Induction Team Member Training Course Fitted to the Scope and Background of the Participants: A Case Study of the African Setting
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s86
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Dissemination of Water-Mediated Infections due to Torrential Rainfalls Leading to Havoc Floods: A Dreadful Curve for Pakistan
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 21 October 2022, pp. 856-857
- Print publication:
- December 2022
-
- Article
-
- You have access
- HTML
- Export citation
Temporal Changes in Epinephrine Dosing in Out-of-Hospital Cardiac Arrest: A Review of EMS Protocols across the United States
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 21 October 2022, pp. 832-835
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A Geographical Analysis of Access to Trauma Centers from US National Parks in 2018
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 20 October 2022, pp. 794-799
- Print publication:
- December 2022
-
- Article
- Export citation
Precise Limb Tourniquet Arterial Occlusion Pressure Determination using Real-Time Ultrasonography and a Capacitive-Based Force Sensor
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 18 October 2022, pp. 772-777
- Print publication:
- December 2022
-
- Article
- Export citation
