
10065 results in Prehospital and Disaster Medicine
Deploying the Red Cross Red Crescent Health Information System (RCHIS): A Pilot with the Portuguese Red Cross in a Red Cross Emergency Clinic (RCEC) Equivalent to a Type 1 Fixed Clinic
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s75
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Integrating Management and Operations of Rapid Response Teams and Emergency Medical Teams Globally
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s110
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Thailand EMT Domestic Response During the COVID-19 Outbreak
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s109
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
Thailand Emergency Medical Team (Thailand EMT) was verified by the WHO in 2019 as a Type 1 fixed EMT. The second wave of COVID-19 hit the country in December 2020. Samut Sakhon province was the center of the spread with many migrant workers infected. Several field hospitals were set up, one being situated in the compound of a Buddhist Temple, Wat Krok Krak. Thailand EMT was tasked in setting up and running the operation here in the initial phase.
Objectives:To describe Thailand EMT’s experience in operating a COVID-19 field hospital.
Method/Description:On December 30, 2020, 16 members of the Thailand EMT were deployed to the Wat Krok Krak Field Hospital. The team comprised of doctors, nurses, pharmacists, and emergency medical technicians who also functioned as logistic officers. Patients were admitted in groups every day. Physicians communicated with patients by using a telemedicine system to monitor patients clinically.
Results/Outcomes:From December 31, 2020 through January 6, 2021, 143 COVID-19 patients were admitted. There were 104 female and 39 male patients. Patients were between 16 and 54 years of age, with a mean of 31.5 years. All were foreigner workers from nearby countries. Three patients had to be referred to a tertiary hospital. The rest of the patients were eventually discharged.
Conclusion:Thailand EMT was able to adapt and deployed to operate a COVID-19 field hospital. Collaboration with relevant agencies and local authorities played a key role. This deployment, although within Thailand, was a good learning opportunity for the team to prepare for future operations.
Tables and Figures (optional)


WHO Emergency Medical Teams Minimal Data Set in Conflict-Stricken Ukraine: Comparative Analysis of a New Primary Health Care Coding Tool
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s57
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
The WHO EMT Minimum Data Set (EMT-MDS) was designed for data collection in sudden-onset disasters. Using EMT-MDS in the context of primary health care (PHC) generated large quantities of low granularity data that threatened the successful delivery of UK-Med’s clinical programs in Ukraine. Accordingly, UK-Med developed, piloted, and implemented a new coding tool (PHC-CT) tailored to PHC presentations prevalent in humanitarian settings.
Objectives:To assess the performance of EMT-MDS and PHC-CT in the generation of programmatically-useful diagnostic codes from data collected in mobile PHC clinics in Ukraine during active conflict.
To compare the performance of EMT-MDS and PHC-CT in this setting and to suggest recommendations for data collection tool improvements.
Method/Description:After multiple iterations, the final version of PHC-CT was used to collect clinical data from all UK-Med clinical encounters in Ukraine from March 28, 2022-May 13, 2022. Clinical data using EMT-MDS were collected simultaneously. The prevalence of each diagnostic code was calculated using both EMT-MDS and PHC-CT, expressed as a proportion of the total diagnoses, and compared between the two coding tools.
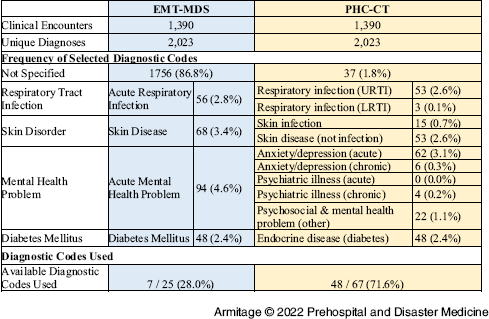
Results/Outcomes:1,390 clinical encounters took place during the study. Data coded using EMT-MDS generated 1,756 diagnoses (86.8% of total diagnoses) categorized as “Other Diagnosis” while the same data coded using PHC-CT generated 37 diagnoses (1.8% of total diagnoses) categorized as “Other Diagnosis.” Only seven of the available 25 diagnostic codes in EMT-MDS were used, while 48 of the 67 available diagnostic codes in PHC-CT were used.
Conclusion:PHC-CT offers substantial benefits beyond those provided by EMT-MDS when utilized in mobile PHC clinics in humanitarian settings.
Tables and Figures (optional)
Table 1. Number of Clinical Encounters, Unique Diagnoses, and Frequency of Selected Diagnostic Codes for EMT-MDS and PHC-CT. (Note: % refers to proportion of diagnoses made)

Cultural Awareness in Emergency Response Teams: Assessment of Cultural Competencies Knowledge and Training
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s91
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Development and Procurement of a National Emergency Medical Team (EMT) Cache for Pacific Island Countries
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s89
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
The Impact of Moral Distress on Clinicians Treating Patients during the COVID-19 Pandemic and the Concurrent Armenian War in 2020: Implications for WHO – EMT Teams
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s114
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Building COVID-19 Capacity with a Simple Tool – “POP-O-MOP” in the Pacific
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s60
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Spinal Immobilization in Disasters: A Systematic Literature Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s73
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Multi-Agency Collaboration Leading to WHO EMT Classification: The Korea Disaster Relief Team
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s98
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
What Helped Support Nurses in the ED at CWM during the COVID-19 Outbreak in Fiji in 2021?
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s105
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Rehabilitation in EMTs: AUSMAT COVID-19 Deployments
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s83
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Introduction of Japan Disaster Medical Assistant Team as a National Emergency Medical Team
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s81
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
A Policy Analysis of the Deployment of International EMT in the WHO African Region during the COVID-19 Pandemic
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s99
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
The Ethical Triage and Management Guidelines of the Entrapped and Mangled Extremity in Resource Scarce Environments: A Systematic Literature Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s69
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Violence Against Health Care in Nigeria and South Sudan: Frontline Health Worker Perspectives on Threats and Solutions
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s55
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Health Care Systems on the Brink of Failure – The Impact of War on the Pattern of Emergency Health Care Visits by Ukrainian Refugees in Poland
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s102
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Use of Mobile Health Units in Conflict Settings - A Scoping Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s62
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Rapid Response Mobile Laboratories (RRML): Standardization as a Tool to Maximize Interoperability
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s68
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Evaluating the Effectiveness of a Small Nomadic Medical Assistance Team to Support Remote Indigenous Communities in Canada during COVID-19 Outbreaks
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s112
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
