
10065 results in Prehospital and Disaster Medicine
Injury-Related Emergency Medical Service Calls, Traffic Accidents, and Crime in Mexico City Before and During the COVID-19 Pandemic
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue 1 / February 2023
- Published online by Cambridge University Press:
- 28 November 2022, pp. 73-80
- Print publication:
- February 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Outbreak of the Ebola Virus: Sudan Strain in Uganda and its Clinical Management
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 15 November 2022, pp. 860-862
- Print publication:
- December 2022
-
- Article
-
- You have access
- HTML
- Export citation
Malaysian Disaster Medicine Research: A Bibliographic Study of Publication Trends
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 14 November 2022, pp. 836-842
- Print publication:
- December 2022
-
- Article
- Export citation
Using a Quality Framework to Explore Air Ambulance Patients’ Journey Outcomes in Central Queensland, Australia
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue 1 / February 2023
- Published online by Cambridge University Press:
- 11 November 2022, pp. 57-64
- Print publication:
- February 2023
-
- Article
- Export citation
The Difficult Airway Redefined
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 09 November 2022, pp. 723-726
- Print publication:
- December 2022
-
- Article
-
- You have access
- HTML
- Export citation
Dispatcher Telephone Assistance on First Aid: An Important but Unexplored Area for Research
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 08 November 2022, pp. 858-859
- Print publication:
- December 2022
-
- Article
-
- You have access
- HTML
- Export citation
Emergency Medical Services Preparedness in Dual Disasters: War in the Era of COVID-19 in Armenia
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 04 November 2022, pp. 749-754
- Print publication:
- December 2022
-
- Article
- Export citation
First Activation of the WHO Emergency Medical Team Minimum Data Set in the 2019 Response to Tropical Cyclone Idai in Mozambique
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 03 November 2022, pp. 727-734
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Coping Strategies for Exposure to Trauma Situations in First Responders: A Systematic Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 03 November 2022, pp. 810-818
- Print publication:
- December 2022
-
- Article
- Export citation
Health Emergency and Disaster Risk Management Workforce Development Strategies: Delphi Consensus Study
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 03 November 2022, pp. 735-748
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Opportunity Cost Analysis for Emergency Medical Teams: A Tool for Policy Making Support
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s106
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
PDM volume 37 issue S2 Cover and Back matter
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, pp. b1-b2
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
International Training on Disaster Medicine - A Peer Education Approach to Disaster Medicine
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s104
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Steps in the Development of a Reliable and Valid National Emergency Unit Readiness Assessment Tool for COVID-19 Outbreak in Iran
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s71
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
An Innovative Database of Clinical Cases to Improve the Realism of Full-Scale Exercises
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s113
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Sharing of Best Practices from an Emergency Medical Team Deployment in Papua New Guinea: Piloting a Health Promotion Program Targeting COVID-19 Vaccine Uptake
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s58
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Building National Emergency Medical Teams in West Africa: Lessons Learnt and Challenges (2017-2022)
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s56
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
A Systematic Literature Review of the Determinants of a Good National Civil-Military Partnership for Rapid Management and Response of Health Emergencies: Lessons for Africa
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s79
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
Enhancing Disaster Response of Emergency Medical Teams through “TEAMS 3.0”-- Does the Multidisciplinary Training Make a Difference?
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s82
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
In the aftermath of disasters, Emergency Medical Teams (EMTs) are dispatched to help local rescue efforts. Although EMTs are recognized to be a critical component of the global health workforce, concerns have emerged over their functioning and effectiveness.1 For example, lack of cooperation and coordination between different EMTs has been a longstanding issue, resulting in fragmented disaster management.2 To enhance the provision of EMT’s field teamwork, the Training for Emergency Medical Teams and European Medical Corps (TEAMS) project was established,3 and later further updated with novel scenarios and exercises (ie, adapting EMT operations to a sudden disaster; becoming a modular team; reflecting on ethical dilemmas) in the complementary “TEAMS 3.0” project where a more comprehensive training package was developed.
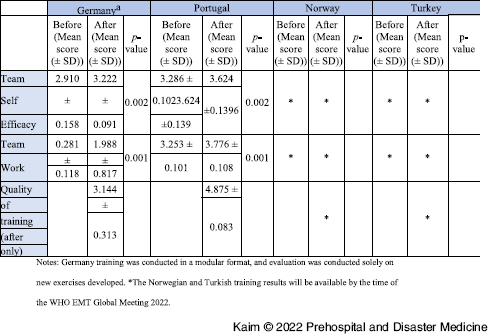
Objectives:The aim of this study was to assess the effectiveness and quality of the TEAMS 3.0 training package in four training programs in Portugal, Germany, Norway, and Turkey.
Method/Description:Participants completed a set of questionnaires designed to assess self-efficacy, teamwork, and quality of training.
Results/Outcomes:The results from the Portugal and German training suggest an improvement for both teams’ self-efficacy and teamwork. The quality of training is regarded as high and deemed as an appropriate tool package for addressing the objectives of the project and the perceived needs of EMT disaster deployment.
Conclusion:Thus far, the TEAMS 3.0 project has demonstrated to be effective in promoting EMT teamwork capacities. The Norwegian and Turkish training results are expected to be available by the time of the WHO EMT Global Meeting 2022.
Tables and Figures (optional)
Table 1. Comparison of Means Before and After the TEAMS 3.0 Training, per Country, for the Team Self-Efficacy Scale, Teamwork Scale, and Quality of Training Scale

Review of the Senegalese Military Emergency Medical Team (EMT) Deployment Following a Tanker Explosion in Freetown, Sierra Leone
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue S2 / November 2022
- Published online by Cambridge University Press:
- 22 November 2022, p. s84
- Print publication:
- November 2022
-
- Article
-
- You have access
- Export citation
