
544 results
Methylation profiles at birth linked to early childhood obesity
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 15 / 2024
- Published online by Cambridge University Press:
- 25 April 2024, e7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prehospital Surgical Cricothyrotomy in a Ground-Based 9-1-1 EMS System: A Retrospective Review
-
- Journal:
- Prehospital and Disaster Medicine , First View
- Published online by Cambridge University Press:
- 23 April 2024, pp. 1-4
-
- Article
- Export citation
The authors’ reply to Jensen et al’s Letter to the Editor
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 16 April 2024, pp. 799-800
- Print publication:
- June 2024
-
- Article
-
- You have access
- HTML
- Export citation
Disinfection of flexible fibre-optic endoscopes out-of-hours: confidential telephone survey of ENT units in England – 20 years on
-
- Journal:
- The Journal of Laryngology & Otology , First View
- Published online by Cambridge University Press:
- 12 February 2024, pp. 1-6
-
- Article
- Export citation
The Pleistocene footprints are younger than we thought: correcting the radiocarbon dates of Ruppia seeds, Tularosa Basin, New Mexico
-
- Journal:
- Quaternary Research / Volume 117 / January 2024
- Published online by Cambridge University Press:
- 10 January 2024, pp. 67-78
-
- Article
- Export citation
Rethinking Transnational Activism through Regional Perspectives: Reflections, Literatures and Cases
-
- Journal:
- Transactions of the Royal Historical Society , First View
- Published online by Cambridge University Press:
- 08 January 2024, pp. 1-27
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Producing and researching podcasts as a reflective medium in English language teaching
-
- Journal:
- Language Teaching / Volume 57 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 09 January 2024, pp. 139-142
- Print publication:
- January 2024
-
- Article
- Export citation
Rapid Dehydroxylation of Nickeliferous Goethite in Lateritic Nickel Ore: X-Ray Diffraction and TEM Investigation
-
- Journal:
- Clays and Clay Minerals / Volume 57 / Issue 6 / December 2009
- Published online by Cambridge University Press:
- 01 January 2024, pp. 751-770
-
- Article
- Export citation
9 Four-Year Practice Effects on the RBANS in a Longitudinal Study of Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 694
-
- Article
-
- You have access
- Export citation
Severe mental illness, race/ethnicity, multimorbidity and mortality following COVID-19 infection: nationally representative cohort study – ADDENDUM
-
- Journal:
- The British Journal of Psychiatry / Volume 224 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 13 December 2023, p. 29
- Print publication:
- January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Developing a framework to improve global estimates of conservation area coverage
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Essential team science skills for biostatisticians on collaborative research teams
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 06 November 2023, e243
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Severe mental illness, race/ethnicity, multimorbidity and mortality following COVID-19 infection: nationally representative cohort study
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 5 / November 2023
- Published online by Cambridge University Press:
- 25 October 2023, pp. 518-525
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Radiofrequency ice dielectric measurements at Summit Station, Greenland
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 09 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$
 –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

Factors associated with loss to follow-up in outpatient parenteral antimicrobial therapy: A retrospective cohort study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 3 / March 2024
- Published online by Cambridge University Press:
- 02 October 2023, pp. 387-389
- Print publication:
- March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
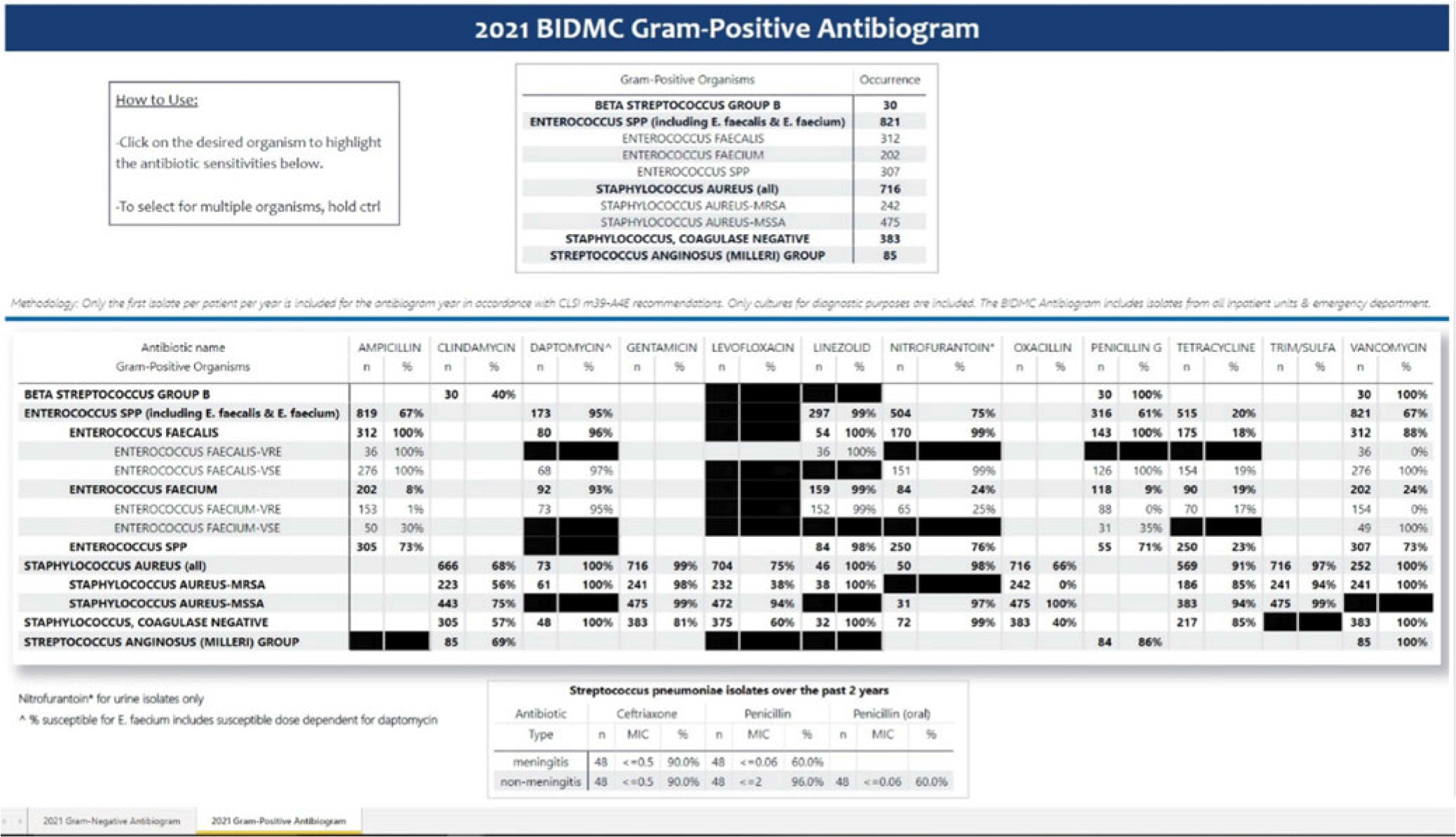
Creating an electronic antibiogram using visualization software: Easily updatable and removes the need for yearly manual review
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s34
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Previously, our hospital manually built a static antibiogram from a surveillance system (VigiLanz) culture report. In 2019, a collaboration between the antimicrobial stewardship team (AST) and the infection control (IC) team set out to leverage data automation to create a dynamic antibiogram. The goal for the antibiogram was the ability to easily distribute and update for hospital staff, with the added ability to perform advanced tracking and surveillance of organism and drug susceptibilities for AST and IC. By having a readily available, accurate, and Clinical and Laboratory Standards Institute (CLSI)–compliant antibiogram, clinicians have the best available data on which to base their empiric antibiotic decisions. Methods: First, assessment of required access to hospital databases and selection of a visualization software (MS Power BI) was performed. Connecting SQL database feeds to Power BI enabled creation of a data model using DAX and M code to comply with the CLSI, generating the first isolate per patient per year. Once a visual antibiogram was created, it was validated against compiled antibiograms using data from the microbiology laboratory middleware (bioMerieux, Observa Integrated Data Management Software). This validation process uncovered some discrepancies between the 2 reference reports due to cascade reporting of susceptibilities. The Observa-derived data were used as the source of truth. The antibiogram prototype was presented to AST/IC members, microbiology laboratory leadership, and other stakeholders to assess functionality. Results: Following feedback and revisions by stakeholders, the new antibiogram was published on a hospital-wide digital platform (Fig. 1). Clinicians may view the antibiogram at any time on desktops from a firewall (or password)–protected intranet. The antibiogram view defaults to the current calendar year and users may interact with the antibiogram rows and columns without disrupting the integrity of the background databases or codes. Each year, simple refreshing of the Power BI antibiogram and changing of the calendar year allows us to easily and accurately update the antibiogram on the hospital-wide digital platform. Conclusions: This interdisciplinary collaboration resulted in a new dynamic, CLSI-compliant antibiogram with improved usability, increased visibility, and straightforward updating. In the future, a mobile version of the antibiogram may further enhance accessibility, bring more useful information to providers, and optimize AST/IC guidelines and education.
Disclosures: None

Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Successful implementation of telehealth visits in the paediatric heart failure and heart transplant population
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 3 / March 2024
- Published online by Cambridge University Press:
- 31 July 2023, pp. 531-534
-
- Article
- Export citation
Outcomes of Pre-Existing Diabetes in People With/without New Onset Severe Mental Illness: A Primary-Secondary Mental Healthcare Linkage in South London, United Kingdom
-
- Journal:
- BJPsych Open / Volume 9 / Issue S1 / July 2023
- Published online by Cambridge University Press:
- 07 July 2023, pp. S2-S3
-
- Article
-
- You have access
- Open access
- Export citation
Chapter 14 - Working with Complex Trauma and Dissociation in Schema Therapy
- from Part III - Applications and Adaptations for Mental Health Presentations
-
- Book:
- Cambridge Guide to Schema Therapy
- Published online:
- 27 July 2023
- Print publication:
- 29 June 2023, pp 266-278
-
- Chapter
- Export citation
