
259 results
Evidence of transmission of New Delhi metallo-β-lactamase-producing Klebsiella pneumoniae through a gastrointestinal endoscope without an elevator channel
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 02 April 2024, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy and safety of a 4-week course of repeated subcutaneous ketamine injections for treatment-resistant depression (KADS study): randomised double-blind active-controlled trial
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 14 July 2023, pp. 533-541
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Epidemiology of resistant gram-negative bacteria in nursing homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 14 March 2023, pp. 1423-1428
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Low function and frequent readmission in nursing home patients with persistent resistant gram-negative bacterial colonization
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s53-s54
-
- Article
-
- You have access
- Open access
- Export citation
-
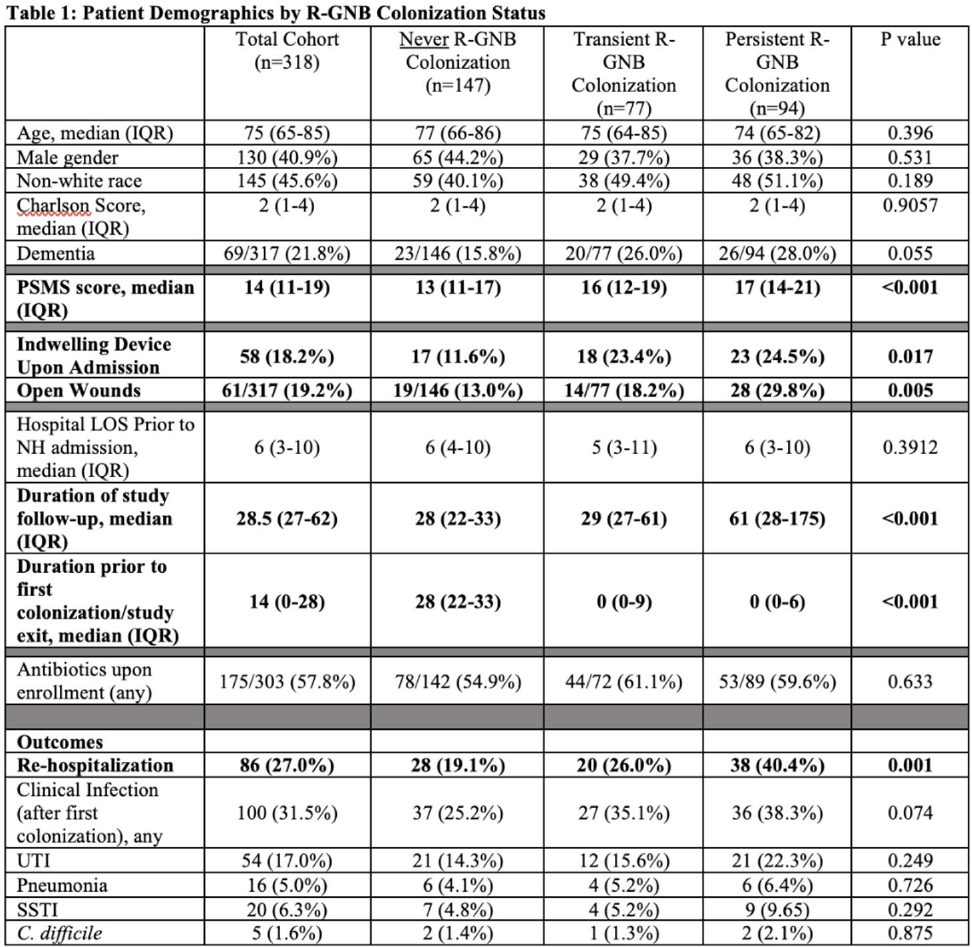
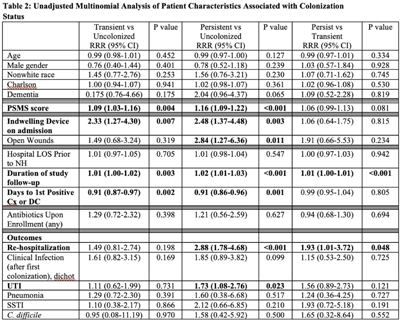
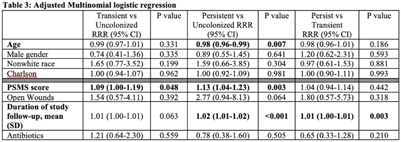
Background: Persistent colonization with resistant gram-negative bacteria (R-GNB) increases risk of clinical infection and intra-facility transmission among nursing home (NH) patients. Limited data exist on the roles of age and function on duration of R-GNB colonization. Methods: Secondary data analysis was performed from a cohort study of patients admitted to 6 Michigan NHs between November 2013 and May 2018. Swabs obtained upon enrollment, day 14, day 30, then monthly until NH discharge from 6 anatomical sites were cultured for GNB. R-GNB were defined as resistant to ciprofloxacin, ceftazidime, or imipenem. Positive R-GNB culture from a single visit followed by negative cultures for the same organism from ≥2 subsequent visits were defined as transient R-GNB colonization. All other patients with positive R-GNB cultures from multiple visits were considered persistently colonized. Demographic data, antibiotic use, device use, and physical self-maintenance scales (PSMSs) were obtained upon enrollment. Characteristics were compared between patients with transient versus persistent R-GNB and uncolonized patients using multinomial logistic regression. Results: We recruited 896 patients (median age, 75 years; 41% male; 46% nonwhite) and followed them for 2,437 total visits. Of 896 patients, 407 (45.4%) were colonized with ≥1 R-GNB during their stay. Of 171 patients with ≥ 2 follow-up visits after R-GNB detection, 94 (55%) remained persistently colonized with the same R-GNB (Table 1). Escherichia coli (30%) and Proteus mirabilis (22%) were the most frequently identified R-GNB. The most common anatomical colonization sites were perirectal (368 [24.3%] of 1,147) groin (340 [14.3%] of 2,046), and hands (115 [4.8%] of 2283). Compared to uncolonized patients, patients with persistent (1.09; 95% CI, 1.00–1.19, P = .048) and transient R-GNB colonization (1.13; 95% CI, 1.04–1.23; P = .003) had lower PSMS (Tables 2 and 3). Compared to uncolonized and transiently colonized patients, patients with persistent R-GNB colonization had prolonged lengths of NH stay (1.01; 95% CI, 1.00–1.01; P = .003). Conclusions: R-GNB colonization in vulnerable NH patients is common (407 [45.5%] of 896 and often persistent (94 [55%] of 171 patients with sufficient follow-up to assess persistence). Patients with persistent R-GNB had lower functional status, longer LOS, and higher readmission rates than those without. R-GNB decolonization should be investigated as a strategy to potentially improve outcomes among NH patients.
Funding: None
Disclosures: None



Comparison of fidaxomicin to oral vancomycin for the treatment of Clostridioides difficile infection in hospitalized patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s72-s73
-
- Article
-
- You have access
- Open access
- Export citation
-
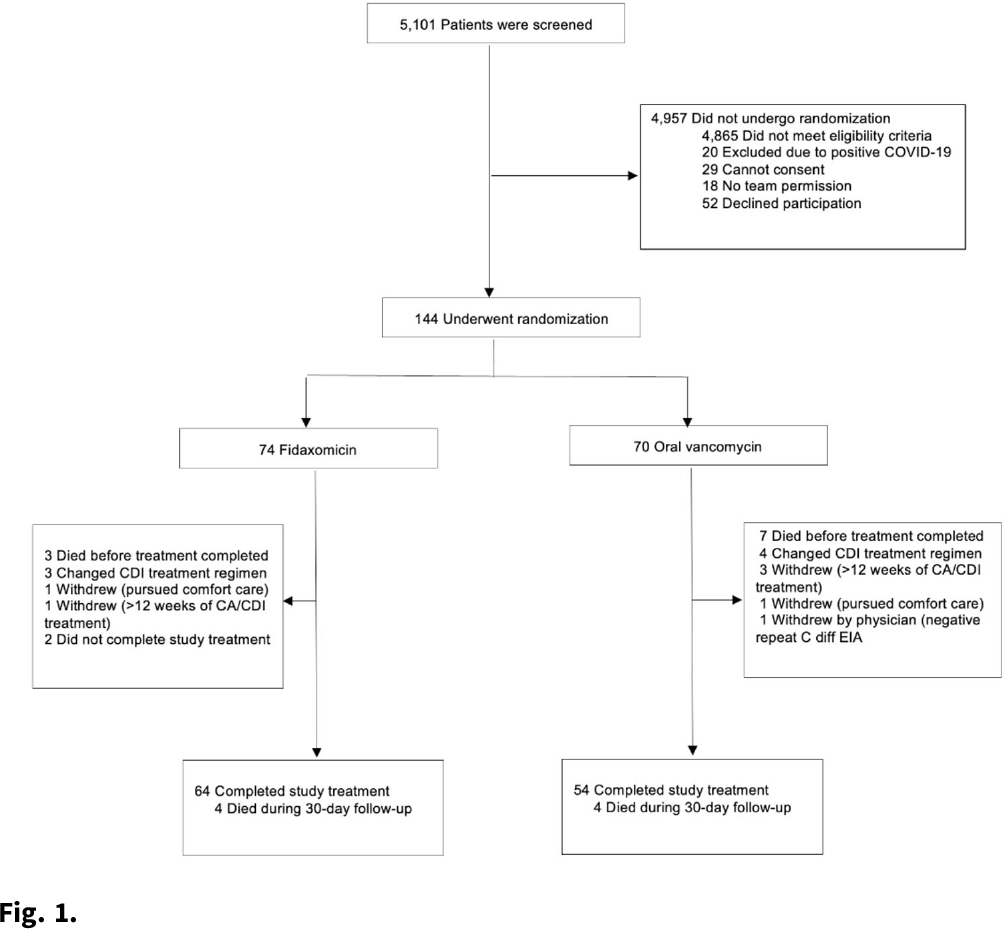
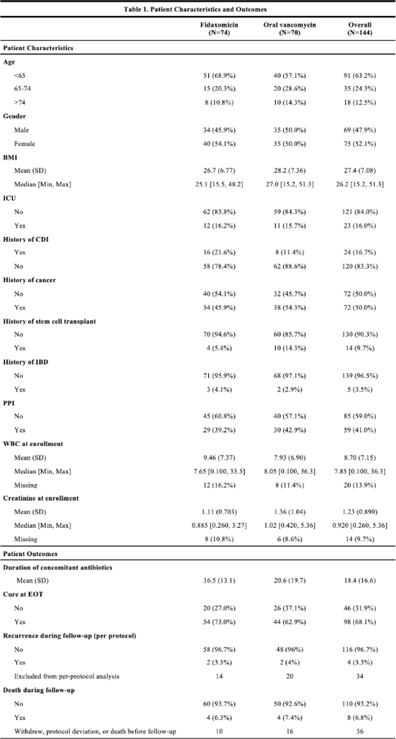
Background:Clostridioides difficile infection (CDI) is a major source of morbidity and mortality. Even after recovery, recurrent CDI (rCDI) occurs frequently, and concomitant antibiotic use for treatment of a concurrent non–C. difficile infection is a major risk factor. Treatment with fidaxomicin versus vancomycin is associated with similar rate of cure and lower recurrence risk. However, the comparative efficacy of these 2 agents remains unclear in those receiving concomitant antibiotics. Methods: We conducted a randomized, controlled, open-label trial at the University of Michigan and St. Joseph Mercy hospitals in Ann Arbor, Michigan. Patients provided written informed consent at enrollment. We included all hospitalized patients aged ≥18 years with a positive test for toxigenic C. difficile, >3 unformed stools per 24 hours, and ≥1 qualifying concomitant antibiotic with a planned treatment of an infection for ≥5 days after enrollment. We excluded patients with complicated CDI, allergy to vancomycin–fidaxomicin, planned adjunctive CDI treatments, CDI treatment for >24 hours prior to enrollment, concomitant laxative use, current or planned colostomy or ileostomy, and/or planned long-term (>12 weeks) concomitant antibiotic use. Clinical cure was defined as resolution of diarrhea for 2 consecutive days maintained until the end of therapy and for 2 days afterward. rCDI was defined as recurrent diarrhea with positive testing within 30 days of initial treatment. Patients were randomized (stratified by ICU status) to fidaxomicin 200 mg twice daily or vancomycin 125 mg orally 4 times daily for 10 days. If concomitant antibiotic treatment continued >10 days, the study drug continued until the concomitant antibiotic ended. Bivariable statistics included t tests and χ2 tests. Results: After screening 5,101 patients for eligibility (May 2017–May 2021), 144 were included and randomized (Fig. 1). Study characteristics and outcomes are noted in Table 1. Baseline characteristics were similar between groups. Most patients were aged <65 years, were on a proton-pump inhibitor (PPI), and were not in the ICU. The mean duration of concomitant antibiotic was 18.4 days. In the intention-to-treat population, clinical cure (73% vs 62.9%; P =.195), and rCDI (3.3% vs 4.0%; P >.99) were similar for fidaxomicin and vancomycin, respectively. Conclusions: In this study of patients with CDI receiving a concomitant antibiotic, a numerically higher proportion were cured with fidaxomicin versus vancomycin, but this result did not reach statistical significance. Overall recurrence was lower than anticipated in both arms compared to previous studies in which duration of CDI treatment was not extended during concomitant antibiotic treatment. Future studies are needed to ascertain whether clinical cure is higher with fidaxomicin than vancomycin during concomitant antibiotic exposure, and whether extending the duration of CDI treatment reduces recurrence.
Funding: Merck & Co.
Disclosures: None


8 - Response to Russell Foster
-
-
- Book:
- The Limits of EUrope
- Published by:
- Bristol University Press
- Published online:
- 13 October 2022
- Print publication:
- 05 April 2022, pp 91-94
-
- Chapter
- Export citation
Optimizing chloroacetamide application timing in dicamba-resistant cotton production systems for control of glyphosate-resistant Palmer amaranth (Amaranthus palmeri)
-
- Journal:
- Weed Technology / Volume 35 / Issue 6 / December 2021
- Published online by Cambridge University Press:
- 09 September 2021, pp. 1007-1013
-
- Article
- Export citation
Multidrug-resistant organism (MDRO) contamination of privacy curtains in nursing homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 5 / May 2022
- Published online by Cambridge University Press:
- 31 May 2021, pp. 666-668
- Print publication:
- May 2022
-
- Article
-
- You have access
- HTML
- Export citation
Native tungsten from the Bol'shaya Pol'ya river valley and Mt Neroyka, Russia
- Part of
-
- Journal:
- Mineralogical Magazine / Volume 85 / Issue 1 / February 2021
- Published online by Cambridge University Press:
- 26 January 2021, pp. 76-81
-
- Article
- Export citation
-
Native tungsten (IMA2011-004), W, is officially described as a new mineral from gold placers in the Bol'shaya Pol'ya river valley, Prepolar Urals, Russia, associated with yttriaite-(Y) and from quartz veins in the Mt Neroyka rock-crystal field, Ust–Puiva, Tyumenskaya Oblast', Russia. Tungsten forms polycrystalline grains and masses, and rarely cubo-octahedra. It is silver white to steel grey in colour, with metallic lustre and grey streak. The calculated density is 19.226 g/cm3. The Vickers hardness (VHN25) is 571.45 kg/mm2. In plane polarised light, tungsten is white with a pale-yellow tint and optically isotropic. Electron microprobe analyses of Bol'shaya Pol'ya river valley material provided W 99.27, Mo 0.06, Mn 0.04, Fe 0.01, total 99.38 wt.%. The five strongest powder X-ray diffraction lines are [dobs Å(I)(hkl)]: 2.2422(100)(110), 1.5835(25)(200), 1.2929(48)(211), 1.0010(23)(310) and 0.8457(24)(321). Tungsten is cubic, Im
 $\bar{3}$m, a = 3.1648(4) Å, V = 31.69(4) Å3 and Z = 2. Some additional occurrences of native tungsten and technogenic tungsten found in Nature are also described.
$\bar{3}$m, a = 3.1648(4) Å, V = 31.69(4) Å3 and Z = 2. Some additional occurrences of native tungsten and technogenic tungsten found in Nature are also described.

Preparing nursing homes for a second wave of coronavirus disease 2019 (COVID-19)
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 10 / October 2021
- Published online by Cambridge University Press:
- 20 October 2020, pp. 1251-1254
- Print publication:
- October 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
CHG Skin Application in Non-ICU Patients with Central Venous Catheters: Impact on CLABSI, MRSA Bacteremia, and LabID Rates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s164-s165
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Profile of Nursing Homes Enrolled in the National Health Safety Network: Focus on Interfacility Communication
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s523-s524
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Incorporating preauthorization into antimicrobial stewardship pharmacist workflow reduces Clostridioides difficile and gastrointestinal panel testing
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 10 / October 2020
- Published online by Cambridge University Press:
- 03 June 2020, pp. 1136-1141
- Print publication:
- October 2020
-
- Article
- Export citation
Psychotic experiences, psychiatric comorbidity and mental health need in the general population: a cross-sectional and cohort study in Southeast London
-
- Journal:
- Psychological Medicine / Volume 51 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 12 November 2019, pp. 147-157
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The devil is in the details: Factors influencing hand hygiene adherence and contamination with antibiotic-resistant organisms among healthcare providers in nursing facilities
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 12 / December 2019
- Published online by Cambridge University Press:
- 24 October 2019, pp. 1394-1399
- Print publication:
- December 2019
-
- Article
- Export citation
Testing and application of a model for snow redistribution (Snow_Blow) in the Ellsworth Mountains, Antarctica
-
- Journal:
- Journal of Glaciology / Volume 65 / Issue 254 / December 2019
- Published online by Cambridge University Press:
- 07 October 2019, pp. 957-970
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The discreditation of oboyerite and a note on the crystal structure of plumbotellurite
-
- Journal:
- Mineralogical Magazine / Volume 83 / Issue 6 / December 2019
- Published online by Cambridge University Press:
- 04 October 2019, pp. 791-797
-
- Article
- Export citation
Hope in Dirt: Report of the Fort Apache Workshop on Forensic Sedimentology Applications to Cultural Property Crime, 15—19 October 2018
-
- Journal:
- International Journal of Cultural Property / Volume 26 / Issue 2 / May 2019
- Published online by Cambridge University Press:
- 20 August 2019, pp. 197-210
-
- Article
- Export citation
Identification of four patients with colistin-resistant Escherichia coli containing the mobile colistin resistance mcr-1 gene from a single health system in Michigan
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 9 / September 2019
- Published online by Cambridge University Press:
- 10 July 2019, pp. 1059-1062
- Print publication:
- September 2019
-
- Article
- Export citation
The effect of cotton growth stage on response to a sublethal concentration of 2,4-D
-
- Journal:
- Weed Technology / Volume 33 / Issue 2 / April 2019
- Published online by Cambridge University Press:
- 14 May 2019, pp. 321-328
-
- Article
- Export citation
