122 results
Stakeholder perspectives of mental healthcare services in Bangladesh, its challenges and opportunities: a qualitative study
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 11 / 2024
- Published online by Cambridge University Press:
- 12 March 2024, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of the conversation tool “I-HARP for COPD” for early identification of palliative care needs in patients with chronic obstructive pulmonary disease
-
- Journal:
- Palliative & Supportive Care , First View
- Published online by Cambridge University Press:
- 16 February 2024, pp. 1-9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Bioclimatic predictors of forest structure, composition and phenology in the Paraguayan Dry Chaco
-
- Journal:
- Journal of Tropical Ecology / Volume 40 / 2024
- Published online by Cambridge University Press:
- 04 January 2024, e1
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
84 Feasibility and Validity of Remote Digital Assessment of Multi-Day Learning in Cognitively Unimpaired Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 487-488
-
- Article
-
- You have access
- Export citation
How old is the Ordovician–Silurian boundary at Dob’s Linn, Scotland? Integrating LA-ICP-MS and CA-ID-TIMS U-Pb zircon dates
-
- Journal:
- Geological Magazine / Volume 160 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 22 November 2023, pp. 1775-1789
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Severe and common mental disorders and risk of emergency hospital admissions for ambulatory care sensitive conditions among the UK Biobank cohort
-
- Journal:
- BJPsych Open / Volume 9 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 07 November 2023, e211
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Radiofrequency ice dielectric measurements at Summit Station, Greenland
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 09 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$
 –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

Risk Factors and outcomes associated with inappropriate empiric broad-spectrum antibiotic use in hospitalized patients with community-acquired pneumonia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s31-s32
-
- Article
-
- You have access
- Open access
- Export citation
-
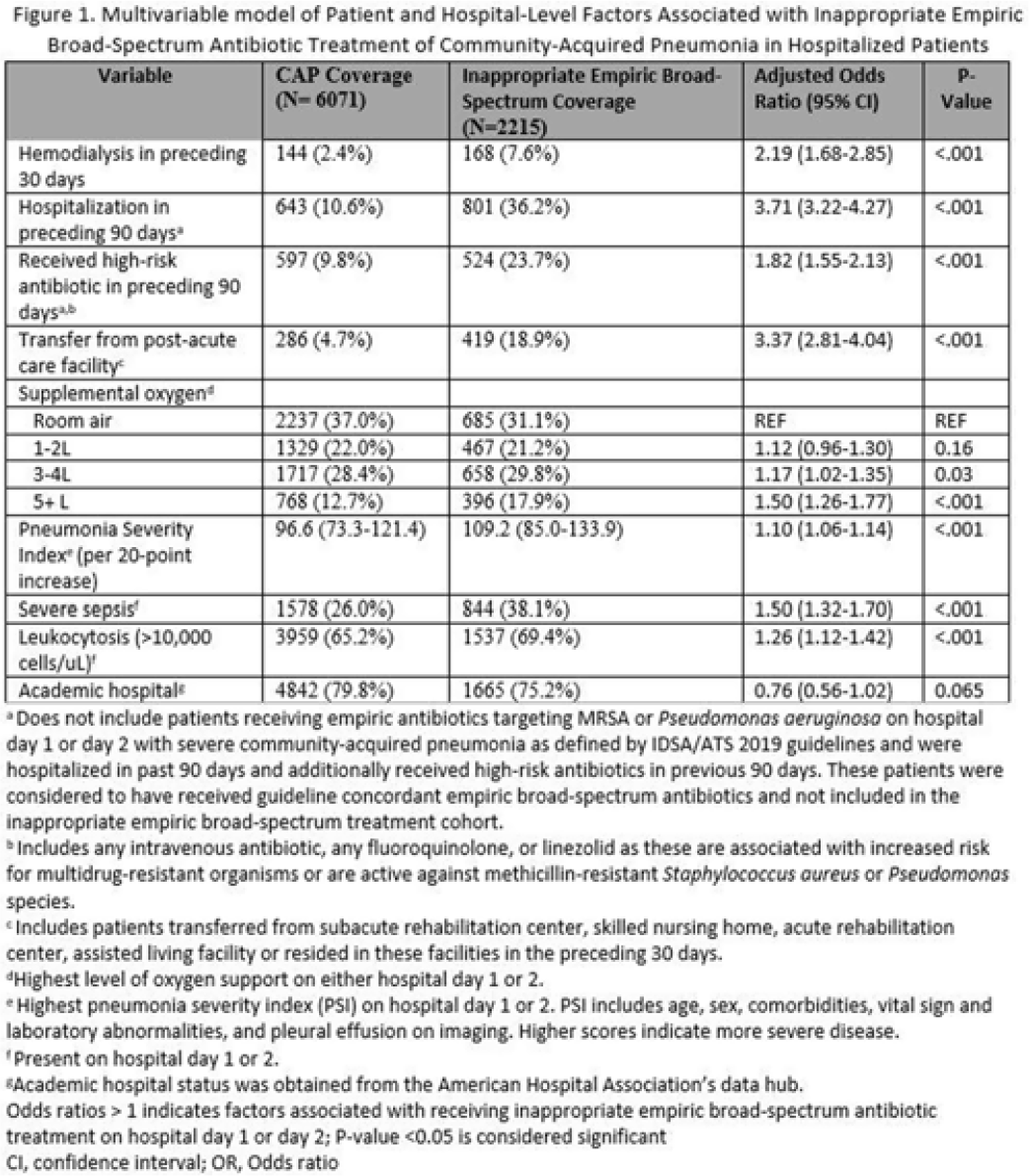
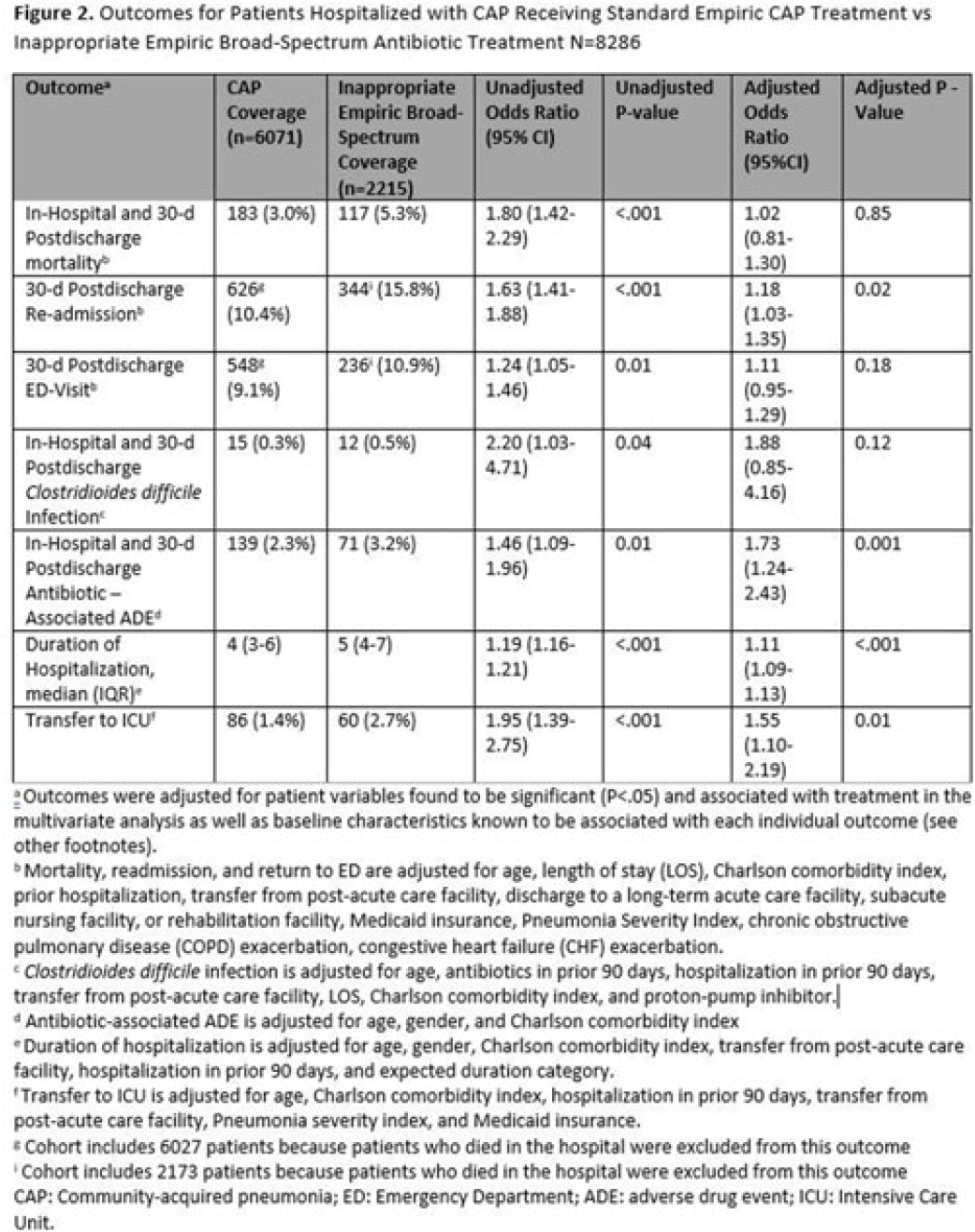
Background: Inappropriate broad-spectrum antibiotic use targeting methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa can result in increased adverse events, antibiotic resistance, and Clostridioides difficile infection. In 2019, revised ATS/IDSA community-acquired pneumonia (CAP) guidelines removed healthcare-associated pneumonia (HCAP) as a clinical entity and modified patient factors warranting empiric broad-spectrum antibiotic (BSA) use. As a result, most patients hospitalized with CAP should receive empiric antibiotics targeting standard CAP pathogens. Based on revised guidelines, we evaluated predictors and outcomes associated with inappropriate BSA use among hospitalized patients with CAP. Methods: Between November 2019 and July 2022, trained abstractors collected data on non-ICU adult medical patients admitted with CAP at 67 Michigan hospitals who received either an inappropriate empiric BSA on hospital day 1 or 2 or a standard CAP regimen. Inappropriate empiric BSA use was defined as use of an anti-MRSA or anti-pseudomonal antibiotic in a patient eligible for standard CAP coverage per IDSA guidelines. Patients with immune compromise, moderate or severe chronic obstructive pulmonary disease (COPD), pulmonary complication, or guideline-concordant treatment with BSA were excluded. Data collected included comorbidities, antibiotic use and hospitalizations in the preceding 90 days, cultures in the preceding year, signs or symptoms of pneumonia, hospital characteristics, and 30-day postdischarge patient outcomes. Data were collected through chart review and patient phone calls. Predictors of inappropriate empiric BSA were evaluated using logistic general estimating equation (GEE) models, accounting for hospital-level clustering. We assessed the effect of inappropriate empiric BSA (vs standard CAP therapy) on 30-day patient outcomes using logistic GEE models controlling for predictors associated with the outcome and probability of treatment. Results: Of 8,286 included patients with CAP, 2,215 (26.7%) were empirically treated with inappropriate BSA. The median BSA treatment was 3 days (IQR, 2.5). After adjustments, factors associated with inappropriate empiric BSA treatment included hospitalization or treatment with high-risk antibiotics in preceding 90 days, transfer from a postacute care facility, hemodialysis, support with ≥3 L supplemental oxygen, severe sepsis, leukocytosis, and higher pneumonia severity index (Fig. 1). After adjustments, patients with inappropriate empiric BSA treatment had higher readmissions 30 days after discharge, more transfers to the intensive care unit, more antibiotic-associated adverse events, and longer hospitalizations (Fig. 2). Conclusions: Patients hospitalized with CAP often received inappropriate BSA as empiric coverage, and this inappropriate antibiotic selection was associated with worse patient outcomes. To improve patient outcomes, stewardship efforts should focus on reducing inappropriate BSA use in patients hospitalized for CAP with historic HCAP risk factors or severe CAP without other guideline-directed indications for BSA.
Financial support. H.M.S. initiative is underwritten by Blue Cross and Blue Shield of Michigan.
Disclosures: None


Patterns, predictors, and patient-reported reasons for antidepressant discontinuation in the WHO World Mental Health Surveys
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 14 September 2023, pp. 67-78
-
- Article
- Export citation
Effectiveness and long-term stability of outpatient cognitive behavioural therapy (CBT) for children and adolescents with anxiety and depressive disorders under routine care conditions
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 13 March 2023, pp. 320-334
- Print publication:
- July 2023
-
- Article
- Export citation
Examining the relation between bilingualism and age of symptom onset in frontotemporal dementia
-
- Journal:
- Bilingualism: Language and Cognition / Volume 27 / Issue 2 / March 2024
- Published online by Cambridge University Press:
- 09 March 2023, pp. 274-286
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Non-suicidal self-injury and emotional burden among university students during the COVID-19 pandemic: cross-sectional online survey
-
- Journal:
- BJPsych Open / Volume 9 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 01 December 2022, e1
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between job role and coronavirus disease 2019 (COVID-19) among healthcare personnel, Iowa, 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 01 December 2022, e188
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Milk yield and composition in dairy goats fed extruded flaxseed or a high-palmitic acid fat supplement
-
- Journal:
- Journal of Dairy Research / Volume 89 / Issue 4 / November 2022
- Published online by Cambridge University Press:
- 13 December 2022, pp. 355-366
- Print publication:
- November 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characterizing Emergency Supply Kit Possession in the United States During the COVID-19 Pandemic: 2020–2021
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 17 October 2022, e283
-
- Article
- Export citation
Developing and sustaining a community advisory committee to support, inform, and translate biomedical research
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 11 October 2022, e20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Governments commit to forest restoration, but what does it take to restore forests?
-
- Journal:
- Environmental Conservation / Volume 49 / Issue 4 / December 2022
- Published online by Cambridge University Press:
- 09 September 2022, pp. 206-214
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sex and age differences in the proportion of experienced symptoms by SARS-CoV-2 serostatus in a community-based cross-sectional study
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 10 August 2022, e157
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Coronavirus disease 2019 (COVID-19) among nonphysician healthcare personnel by work location at a tertiary-care center, Iowa, 2020–2021
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 02 June 2022, pp. 1351-1354
- Print publication:
- August 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19 incidence among nonphysician healthcare workers at a tertiary care center–Iowa, 2020–2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s6-s7
-
- Article
-
- You have access
- Open access
- Export citation
-
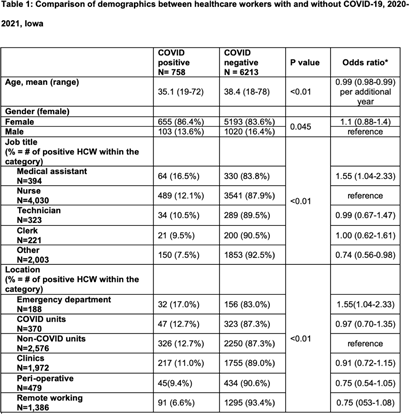
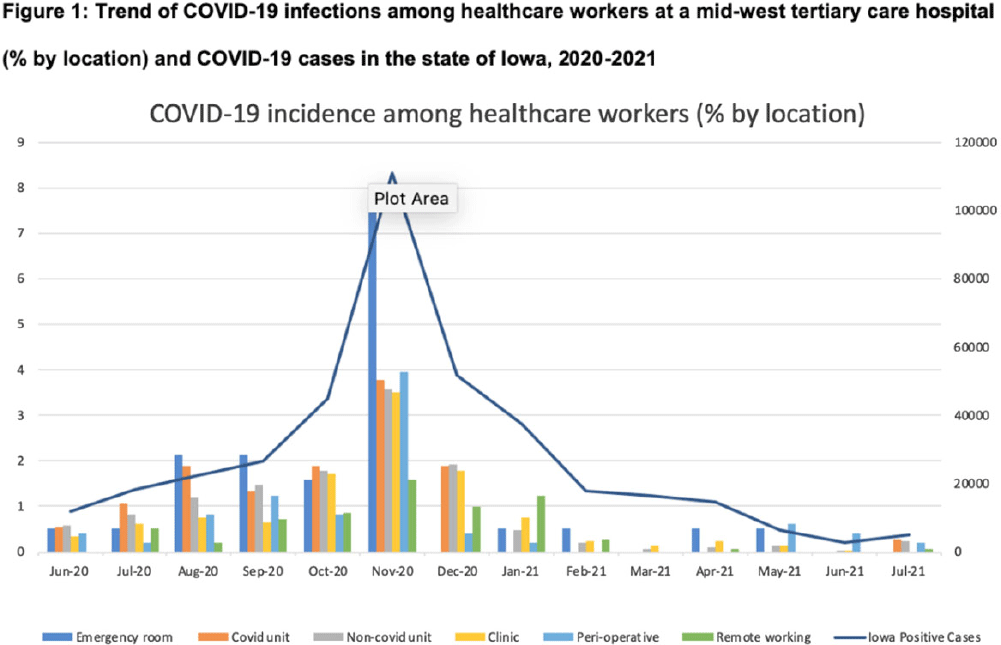
Background: Whether working on COVID-19 designated units put healthcare workers (HCWs) at higher risk of acquiring COVID-19 is not fully understood. We report trends of COVID-19 incidence among nonphysician HCWs and the association between the risk of acquiring COVID-19 and work location in the hospital. Methods: The University of Iowa Hospitals & Clinics (UIHC) is an 811-bed, academic medical center serving as a referral center for Iowa. We retrospectively collected COVID-19–associated data for nonphysician HCWs from Employee Health Clinic between June 1st 2020 and July 31th 2021. The data we abstracted included age, sex, job title, working location, history of COVID-19, and date of positive COVID-19 test if they had a history of COVID-19. We excluded HCWs who did not have a designated working location and those who worked on multiple units during the same shift (eg, medicine resident, hospitalist, etc) to assess the association between COVID-19 infections and working location. Job titles were divided into the following 5 categories: (1) nurse, (2) medical assistant (MA), (3) technician, (4) clerk, and (5) others (eg patient access, billing office, etc). Working locations were divided into the following 6 categories: (1) emergency department (ED), (2) COVID-19 unit, (3) non–COVID-19 unit, (4) Clinic, (5) perioperative units, and (6) remote work. Results: We identified 6,971 HCWs with work locations recorded. During the study period, 758 HCWs (10.8%) reported being diagnosed with COVID-19. Of these 758 COVID-19 cases, 658 (86.8%) were diagnosed before vaccines became available. The location with the highest COVID-19 incidence was the ED (17%), followed by both COVID-19 and non–COVID-19 units (12.7%), clinics (11.0%), perioperative units (9.4%) and remote work stations (6.6%, p Conclusions: Strict and special infection control strategies may be needed for HCWs in the ED, especially where vaccine uptake is low. The administrative control of HCWs working remotely may be associated with a lower incidence of COVID-19. Given that the difference in COVID-19 incidence among HCWs by location was lower and comparable after the availability of COVID-19 vaccines, facilities should make COVID-19 vaccination mandatory as a condition of employment for all HCWs, especially in areas where the COVID-19 incidence is high.
Funding: None
Disclosures: None