
174 results
Psychometric and adherence considerations for high-frequency, smartphone-based cognitive screening protocols in older adults
-
- Journal:
- Journal of the International Neuropsychological Society , First View
- Published online by Cambridge University Press:
- 20 September 2024, pp. 1-9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Risks in Renaissance Art
- Production, Purchase, and Reception
-
- Published online:
- 11 January 2024
- Print publication:
- 21 March 2024
-
- Element
- Export citation
Bloodstream infection burden among cancer clinic patients with PICC Lines: A prospective, observational study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s49
-
- Article
-
- You have access
- Open access
- Export citation
-
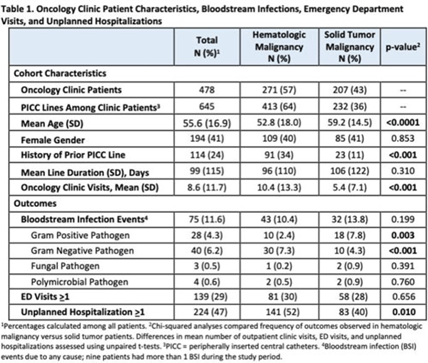
Background: Oncology patients are at high risk for bloodstream infection (BSI) due to immunosuppression and frequent use of central venous catheters. Surveillance in this population is largely relegated to inpatient settings and limited data are available describing community burden. We evaluated rates of BSI, clinic or emergency department (ED) visits, and hospitalizations in a large cohort of oncology outpatients with peripherally inserted central catheters (PICCs). Methods: In this prospective, observational study, we followed a convenience sample of adults (age>18) with PICCs at a large academic outpatient oncology clinic for 35 months between July 2015 and November 2018. We assessed demographics, malignancy type, PICC insertion and removal dates, history of prior PICC, and line duration. Outcomes included BSI events (defined as >1 positive blood cultures or >2 positive blood cultures if coagulase-negative Staphylococcus), ED visits (without hospitalization), and unplanned hospitalizations (excluding scheduled chemotherapy hospitalizations). We used χ2 analyses to compare the frequency of categorical outcomes, and we used unpaired t tests to assess differences in means of continuous variable in hematologic versus solid-tumor malignancy patients. We used generalized linear mixed-effects models to assess differences in BSI (clustered by patient) separately for gram-positive and gram-negative BSI outcomes. Results: Among 478 patients with 658 unique PICC lines and 64,190 line days, 271 patients (413 lines) had hematologic malignancy and 207 patients (232 lines) had solid-tumor malignancy. Cohort characteristics and outcomes stratified by malignancy type are shown in Table 1. Compared to those with hematologic malignancy, solid-tumor patients were older, had 47% fewer clinic visits, and had 32% lower frequency of prior PICC lines. Overall, there were 75 BSI events (12%; 1.2 per 1,000 catheter days). We detected no significant difference in BSI rates when comparing solid-tumor versus hematologic malignancies (P = 0.20); BSIs with gram-positive pathogen were 69% higher in patients with solid tumors. Gram-negative BSIs were 41% higher in patients with hematologic malignancy. Solid-tumor malignancy was associated with 4.5-fold higher odds of developing BSI with gram-positive pathogen (OR, 4.48; 95% CI, 1.60–12.60; P = .005) compared to those with hematologic malignancy, after adjusting for age, sex, history of prior PICC, and line duration. Differences in gram-negative BSI were not significant on multivariate analysis. Conclusions: The burden of all-cause BSIs in cancer clinic adults with PICC lines was 12% or 1.2 per 1,000 catheter days, as high as nationally reported inpatient BSI rates. Higher risk of gram-positive BSIs in solid-tumor patients suggests the need for targeted infection prevention activities in this population, such as improvements in central-line monitoring, outpatient care, and maintenance of lines and/or dressings, as well as chlorhexidine bathing to reduce skin bioburden.
Disclosures: None

Raccoon rabies control and elimination in the northeastern USA and southern Québec, Canada
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, e62
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
Rabies virus (RABV) is a deadly zoonosis that circulates in wild carnivore populations in North America. Intensive management within the USA and Canada has been conducted to control the spread of the raccoon (Procyon lotor) variant of RABV and work towards elimination. We examined RABV occurrence across the northeastern USA and southeastern Québec, Canada during 2008–2018 using a multi-method, dynamic occupancy model. Using a 10 km × 10 km grid overlaid on the landscape, we examined the probability that a grid cell was occupied with RABV and relationships with management activities (oral rabies vaccination (ORV) and trap-vaccinate-release efforts), habitat, neighbour effects and temporal trends. We compared raccoon RABV detection probabilities between different surveillance samples (e.g. animals that are strange acting, road-kill, public health samples). The management of RABV through ORV was found to be the greatest driver in reducing the occurrence of rabies on the landscape. Additionally, RABV occupancy declined further with increasing duration of ORV baiting programmes. Grid cells north of ORV management were at or near elimination ($\hat{\psi }_{{\rm north}}$
 = 0.00, s.e. = 0.15), managed areas had low RABV occupancy ($\hat{\psi }_{{\rm managed}}$
= 0.00, s.e. = 0.15), managed areas had low RABV occupancy ($\hat{\psi }_{{\rm managed}}$ = 0.20, s.e. = 0.29) and enzootic areas had the highest level of RABV occupancy ($\hat{\psi }_{{\rm south}}$
= 0.20, s.e. = 0.29) and enzootic areas had the highest level of RABV occupancy ($\hat{\psi }_{{\rm south}}$ = 0.83, s.e. = 0.06). These results provide evidence that past management actions have been being successful at the goals of reducing and controlling the raccoon variant of RABV. At a finer scale we also found that vaccine bait type and bait density impacted RABV occupancy. Detection probabilities varied; samples from strange acting animals and public health had the highest detection rates. Our results support the movement of the ORV zone south within the USA due to high elimination probabilities along the US border with Québec. Additional enhanced rabies surveillance is still needed to ensure elimination is maintained.
= 0.83, s.e. = 0.06). These results provide evidence that past management actions have been being successful at the goals of reducing and controlling the raccoon variant of RABV. At a finer scale we also found that vaccine bait type and bait density impacted RABV occupancy. Detection probabilities varied; samples from strange acting animals and public health had the highest detection rates. Our results support the movement of the ORV zone south within the USA due to high elimination probabilities along the US border with Québec. Additional enhanced rabies surveillance is still needed to ensure elimination is maintained.



Archives of Idi Amin
-
- Journal:
- History in Africa / Volume 48 / June 2021
- Published online by Cambridge University Press:
- 11 February 2022, pp. 413-427
-
- Article
- Export citation
A Veterans’ Healthcare Administration (VHA) antibiotic stewardship intervention to improve outpatient antibiotic use for acute respiratory infections: A cost-effectiveness analysis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 29 September 2021, pp. 1389-1395
- Print publication:
- October 2022
-
- Article
- Export citation
Characterisation of age and polarity at onset in bipolar disorder
-
- Journal:
- The British Journal of Psychiatry / Volume 219 / Issue 6 / December 2021
- Published online by Cambridge University Press:
- 25 August 2021, pp. 659-669
- Print publication:
- December 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nonventilator hospital-acquired pneumonia: A call to action: Recommendations from the National Organization to Prevent Hospital-Acquired Pneumonia (NOHAP) among nonventilated patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 8 / August 2021
- Published online by Cambridge University Press:
- 09 June 2021, pp. 991-996
- Print publication:
- August 2021
-
- Article
- Export citation
Reporting uncertainty in results—Response to article on copper cold-spray technology
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 4 / April 2022
- Published online by Cambridge University Press:
- 18 May 2021, p. 537
- Print publication:
- April 2022
-
- Article
-
- You have access
- HTML
- Export citation
The Unseen Archive of Idi Amin: Making History in a Tight Corner
-
- Journal:
- Comparative Studies in Society and History / Volume 63 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 14 January 2021, pp. 5-40
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Enhancing Infection Prevention and Control Capacity in Health Facilities Following the 2019 Ebola Outbreak in Kasese, Uganda
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s471
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
VA Antibiotic Stewardship Intervention to Improve Outpatient Antibiotic Use for ARIs: A Cost-Effectiveness Analysis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s55
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Validation of the SHEA/IDSA severity criteria to predict poor outcomes among inpatients and outpatients with Clostridioides difficile infection
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 5 / May 2020
- Published online by Cambridge University Press:
- 30 January 2020, pp. 510-516
- Print publication:
- May 2020
-
- Article
- Export citation
Response of ‘Russet Burbank’ Seed Tubers Containing Dicamba and Glyphosate
-
- Journal:
- Weed Technology / Volume 33 / Issue 1 / February 2019
- Published online by Cambridge University Press:
- 07 December 2018, pp. 9-16
-
- Article
- Export citation
Multi-Trait Analysis of GWAS and Biological Insights Into Cognition: A Response to Hill (2018)
-
- Journal:
- Twin Research and Human Genetics / Volume 21 / Issue 5 / October 2018
- Published online by Cambridge University Press:
- 13 July 2018, pp. 394-397
-
- Article
-
- You have access
- HTML
- Export citation
12 - When Do Religious Accommodations Burden Others?
- from Part III - Objecting to Antidiscrimination Laws in the Name of Mainstream Religious Convictions
-
-
- Book:
- The Conscience Wars
- Published online:
- 20 June 2018
- Print publication:
- 05 July 2018, pp 328-346
-
- Chapter
- Export citation
Contents
-
- Book:
- Modern Evolutionary Economics
- Published online:
- 21 April 2018
- Print publication:
- 03 May 2018, pp v-vi
-
- Chapter
- Export citation
Index
-
- Book:
- Modern Evolutionary Economics
- Published online:
- 21 April 2018
- Print publication:
- 03 May 2018, pp 263-272
-
- Chapter
- Export citation
Copyright page
-
- Book:
- Modern Evolutionary Economics
- Published online:
- 21 April 2018
- Print publication:
- 03 May 2018, pp iv-iv
-
- Chapter
- Export citation
