
50 results
Investigating the impact of the COVID-19 pandemic on recovery colleges: multi-site qualitative study
-
- Journal:
- BJPsych Open / Volume 10 / Issue 3 / May 2024
- Published online by Cambridge University Press:
- 16 May 2024, e113
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Deferring to Expertise whilst Maintaining Autonomy
-
- Journal:
- Episteme , First View
- Published online by Cambridge University Press:
- 15 February 2024, pp. 1-20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The predictive role of symptoms in COVID-19 diagnostic models: A longitudinal insight
-
- Journal:
- Epidemiology & Infection / Volume 152 / 2024
- Published online by Cambridge University Press:
- 22 January 2024, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
48 Associations Between Cognitive Function and Social Networks in Older Adults: Quality and not Quantity?
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 834-835
-
- Article
-
- You have access
- Export citation
25 Specific Facets of Trait Mindfulness Show Differences in Associations with Affective and Cognitive Measures in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 338
-
- Article
-
- You have access
- Export citation
52 Association Between COVID-19 Coping Strategies and Cognitive Function in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 360
-
- Article
-
- You have access
- Export citation
6 Now or Later? Decision-Making Preferences in Community-Dwelling Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 321-322
-
- Article
-
- You have access
- Export citation
Evaluation of a menu box delivery service for Australian long-day care services to improve food provision and child intake: a cluster randomised controlled trial
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 13 October 2023, pp. 3122-3133
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
“More effective” is not necessarily “better”: Some ethical considerations when influencing individual behaviour
-
- Journal:
- Behavioral and Brain Sciences / Volume 46 / 2023
- Published online by Cambridge University Press:
- 30 August 2023, e151
-
- Article
-
- You have access
- HTML
- Export citation
Characteristics of healthcare personnel who reported concerns related to PPE use during care of COVID-19 patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s8-s9
-
- Article
-
- You have access
- Open access
- Export citation
-
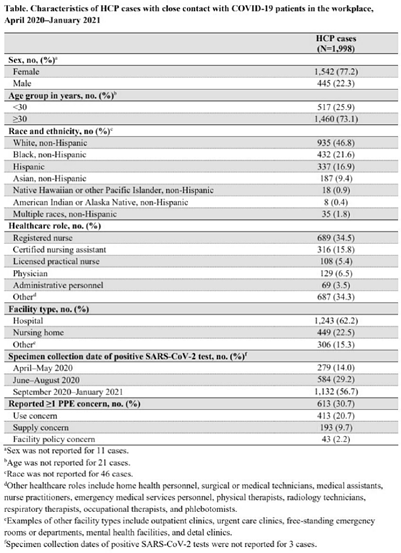
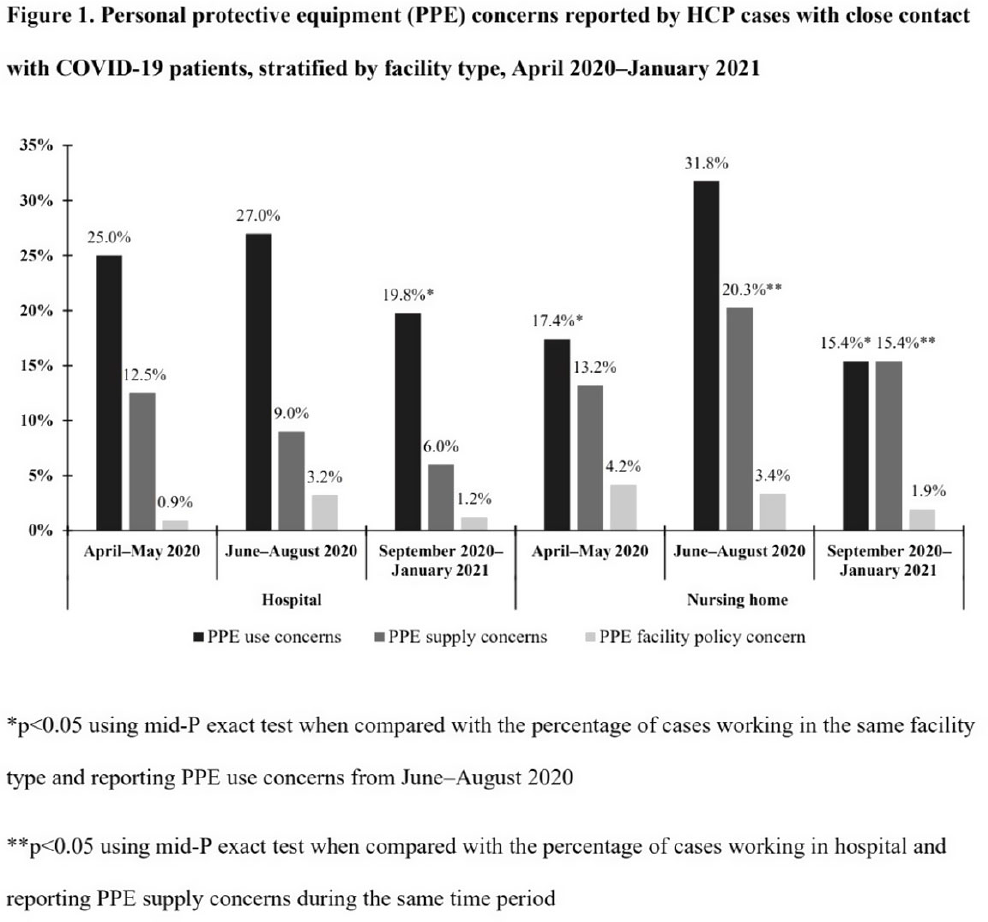
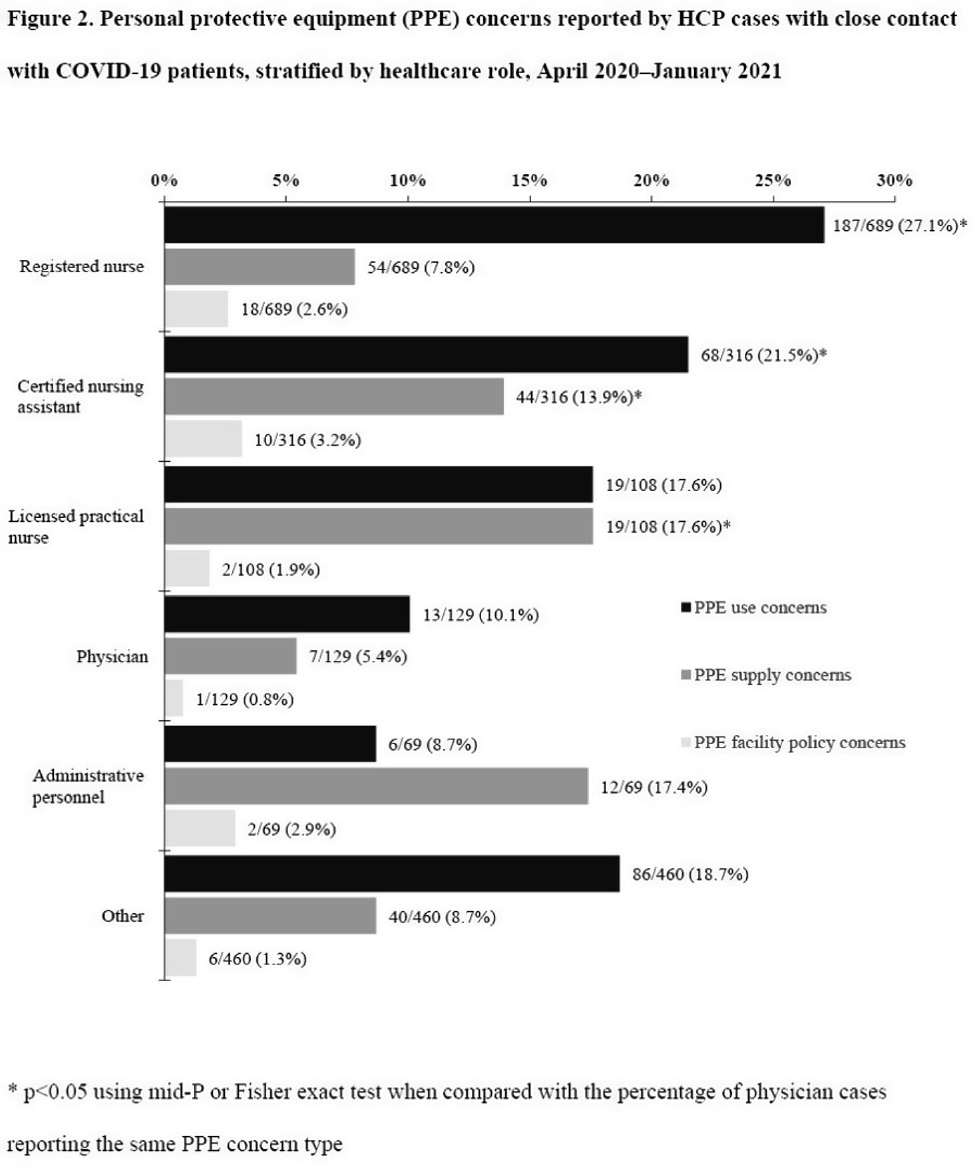
Background: Healthcare facilities have experienced many challenges during the COVID-19 pandemic, including limited personal protective equipment (PPE) supplies. Healthcare personnel (HCP) rely on PPE, vaccines, and other infection control measures to prevent SARS-CoV-2 infections. We describe PPE concerns reported by HCP who had close contact with COVID-19 patients in the workplace and tested positive for SARS-CoV-2. Method: The CDC collaborated with Emerging Infections Program (EIP) sites in 10 states to conduct surveillance for SARS-CoV-2 infections in HCP. EIP staff interviewed HCP with positive SARS-CoV-2 viral tests (ie, cases) to collect data on demographics, healthcare roles, exposures, PPE use, and concerns about their PPE use during COVID-19 patient care in the 14 days before the HCP’s SARS-CoV-2 positive test. PPE concerns were qualitatively coded as being related to supply (eg, low quality, shortages); use (eg, extended use, reuse, lack of fit test); or facility policy (eg, lack of guidance). We calculated and compared the percentages of cases reporting each concern type during the initial phase of the pandemic (April–May 2020), during the first US peak of daily COVID-19 cases (June–August 2020), and during the second US peak (September 2020–January 2021). We compared percentages using mid-P or Fisher exact tests (α = 0.05). Results: Among 1,998 HCP cases occurring during April 2020–January 2021 who had close contact with COVID-19 patients, 613 (30.7%) reported ≥1 PPE concern (Table 1). The percentage of cases reporting supply or use concerns was higher during the first peak period than the second peak period (supply concerns: 12.5% vs 7.5%; use concerns: 25.5% vs 18.2%; p Conclusions: Although lower percentages of HCP cases overall reported PPE concerns after the first US peak, our results highlight the importance of developing capacity to produce and distribute PPE during times of increased demand. The difference we observed among selected groups of cases may indicate that PPE access and use were more challenging for some, such as nonphysicians and nursing home HCP. These findings underscore the need to ensure that PPE is accessible and used correctly by HCP for whom use is recommended.
Funding: None
Disclosures: None



Revisiting ‘Toledo, Rome, and the Legacy of Gaul’: new evidence from the Divine Office
-
- Journal:
- Plainsong & Medieval Music / Volume 31 / Issue 1 / April 2022
- Published online by Cambridge University Press:
- 07 April 2022, pp. 1-35
- Print publication:
- April 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
10 - The Developmental Science of Politics
- from Part I - Foundations of Political Psychology
-
-
- Book:
- The Cambridge Handbook of Political Psychology
- Published online:
- 17 February 2022
- Print publication:
- 24 February 2022, pp 159-174
-
- Chapter
- Export citation
Parents’ decision-making for their foetus or neonate with a severe congenital heart defect
-
- Journal:
- Cardiology in the Young / Volume 32 / Issue 6 / June 2022
- Published online by Cambridge University Press:
- 19 August 2021, pp. 896-903
-
- Article
- Export citation
Virtual balint group experience due to the COVID-19 pandemic
-
- Journal:
- BJPsych Open / Volume 7 / Issue S1 / June 2021
- Published online by Cambridge University Press:
- 18 June 2021, pp. S127-S128
-
- Article
-
- You have access
- Open access
- Export citation
Trends in referrals to liaison psychiatry teams from UK emergency departments for patients over 65
-
- Journal:
- BJPsych Open / Volume 7 / Issue S1 / June 2021
- Published online by Cambridge University Press:
- 18 June 2021, pp. S311-S312
-
- Article
-
- You have access
- Open access
- Export citation
Practices and activities among healthcare personnel with severe acute respiratory coronavirus virus 2 (SARS-CoV-2) infection working in different healthcare settings—ten Emerging Infections Program sites, April–November 2020
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 02 June 2021, pp. 1058-1062
- Print publication:
- August 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
4281 Developing a predictive tool to detect peripheral artery disease (PAD): Examining patient-reported symptoms in ischemic versus non-ischemic conditions (PREDICT PAD)
-
- Journal:
- Journal of Clinical and Translational Science / Volume 4 / Issue s1 / June 2020
- Published online by Cambridge University Press:
- 29 July 2020, p. 27
-
- Article
-
- You have access
- Open access
- Export citation
Text Messaging and Disaster Preparedness Aids Engagement, Re-Engagement, Retention, and Communication Among Puerto Rican Participants in a Human Immunodeficiency Virus (HIV) Self-Testing Study After Hurricanes Irma and Maria
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 08 April 2020, e2
-
- Article
- Export citation
In vitro screening of 51 birdsfoot trefoil (Lotus corniculatus L.; Fabaceae) strains for anti-parasitic effects against Haemonchus contortus
-
- Journal:
- Parasitology / Volume 146 / Issue 6 / May 2019
- Published online by Cambridge University Press:
- 14 January 2019, pp. 828-836
-
- Article
- Export citation
2085: MyResearchHome@Duke—launch and adoption of a portal for the research community
-
- Journal:
- Journal of Clinical and Translational Science / Volume 1 / Issue S1 / September 2017
- Published online by Cambridge University Press:
- 10 May 2018, p. 11
-
- Article
-
- You have access
- Open access
- Export citation
