373 results
Interrelationships of Physical and Chemical Properties of Kaolinites
-
- Journal:
- Clays and Clay Minerals / Volume 14 / February 1966
- Published online by Cambridge University Press:
- 01 July 2024, pp. 331-346
-
- Article
- Export citation
Mineralogy and Geology of the Maungaparerua Halloysite Deposit in New Zealand
-
- Journal:
- Clays and Clay Minerals / Volume 25 / Issue 1 / February 1977
- Published online by Cambridge University Press:
- 01 July 2024, pp. 1-5
-
- Article
- Export citation
Childhood adversity and mental health admission patterns prior to young person suicide (CHASE): a case-control 36 year linked hospital data study, Scotland UK 1981–2017
-
- Journal:
- BJPsych Open / Volume 10 / Issue 4 / July 2024
- Published online by Cambridge University Press:
- 03 June 2024, e124
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies used for the COVID-OUT decentralized trial of outpatient treatment of SARS-CoV-2
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 07 November 2023, e242
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Climate, Weather Extremes and Health: Latest WHO-WMO Resources and Tools for Health Emergency Managers
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, p. s64
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Parole, where psychiatry meets public protection
-
- Journal:
- BJPsych Advances / Volume 30 / Issue 2 / March 2024
- Published online by Cambridge University Press:
- 23 March 2023, pp. 97-105
- Print publication:
- March 2024
-
- Article
- Export citation
Cannabis use and psychotic disorders in diverse settings in the Global South: findings from INTREPID II
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 23 March 2023, pp. 7062-7069
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Expanding mental health services in low- and middle-income countries: A task-shifting framework for delivery of comprehensive, collaborative, and community-based care
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 10 / 2023
- Published online by Cambridge University Press:
- 27 February 2023, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Urbanicity and rates of untreated psychotic disorders in three diverse settings in the Global South
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 14 / October 2023
- Published online by Cambridge University Press:
- 16 January 2023, pp. 6459-6467
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Collective bargaining for paid parental leave in Australia 2005–2010: A complex context effect
-
- Journal:
- The Economic and Labour Relations Review / Volume 25 / Issue 1 / March 2014
- Published online by Cambridge University Press:
- 01 January 2023, pp. 47-62
-
- Article
- Export citation
Financialisation and inequality in Australia
-
- Journal:
- The Economic and Labour Relations Review / Volume 28 / Issue 4 / December 2017
- Published online by Cambridge University Press:
- 01 January 2023, pp. 519-537
-
- Article
- Export citation
Life events and psychosis: case–control study from India, Nigeria, and Trinidad and Tobago
-
- Journal:
- BJPsych Open / Volume 8 / Issue 5 / September 2022
- Published online by Cambridge University Press:
- 16 September 2022, e168
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 21 - A Dynamical Systems Perspective on Thalamic Circuit Function
- from Section 9: - Computation
-
-
- Book:
- The Thalamus
- Published online:
- 12 August 2022
- Print publication:
- 01 September 2022, pp 401-415
-
- Chapter
- Export citation
GASKAP-HI Pilot Survey Science III: An unbiased view of cold gas in the Small Magellanic Cloud
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 39 / 2022
- Published online by Cambridge University Press:
- 05 August 2022, e034
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We present the first unbiased survey of neutral hydrogen absorption in the Small Magellanic Cloud. The survey utilises pilot neutral hydrogen observations with the Australian Square Kilometre Array Pathfinder telescope as part of the Galactic Australian Square Kilometre Array Pathfinder neutral hydrogen project whose dataset has been processed with the Galactic Australian Square Kilometre Array Pathfinder-HI absorption pipeline, also described here. This dataset provides absorption spectra towards 229 continuum sources, a 275% increase in the number of continuum sources previously published in the Small Magellanic Cloud region, as well as an improvement in the quality of absorption spectra over previous surveys of the Small Magellanic Cloud. Our unbiased view, combined with the closely matched beam size between emission and absorption, reveals a lower cold gas faction (11%) than the 2019 ATCA survey of the Small Magellanic Cloud and is more representative of the Small Magellanic Cloud as a whole. We also find that the optical depth varies greatly between the Small Magellanic Cloud’s bar and wing regions. In the bar we find that the optical depth is generally low (correction factor to the optically thin column density assumption of
 $\mathcal{R}_{\mathrm{HI}} \sim 1.04$
) but increases linearly with column density. In the wing however, there is a wide scatter in optical depth despite a tighter range of column densities.
$\mathcal{R}_{\mathrm{HI}} \sim 1.04$
) but increases linearly with column density. In the wing however, there is a wide scatter in optical depth despite a tighter range of column densities.

Epidemiology and genomics of a slow outbreak of methicillin-resistant Staphyloccus aureus (MRSA) in a neonatal intensive care unit: Successful chronic decolonization of MRSA-positive healthcare personnel
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 16 June 2022, pp. 589-596
- Print publication:
- April 2023
-
- Article
- Export citation
6 - Macroeconomics before Microeconomics
-
-
- Book:
- Pasinetti and the Classical Keynesians
- Published online:
- 17 February 2022
- Print publication:
- 24 February 2022, pp 157-186
-
- Chapter
- Export citation
Deep ancestry of collapsing networks of nomadic hunter–gatherers in Borneo
-
- Journal:
- Evolutionary Human Sciences / Volume 4 / 2022
- Published online by Cambridge University Press:
- 21 February 2022, e9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The influence of tart cherries (Prunus Cerasus) on vascular function and the urinary metabolome: a randomised placebo-controlled pilot study
-
- Journal:
- Journal of Nutritional Science / Volume 10 / 2021
- Published online by Cambridge University Press:
- 13 September 2021, e73
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Successful Treatment of Invasive MRSA Infections in Children Using Area Under the Vancomycin Concentration-Time Curve Divided by the Minimum Inhibitory Concentration (AUC/MIC) to Measure Vancomycin Exposure
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s31
-
- Article
-
- You have access
- Open access
- Export citation
-
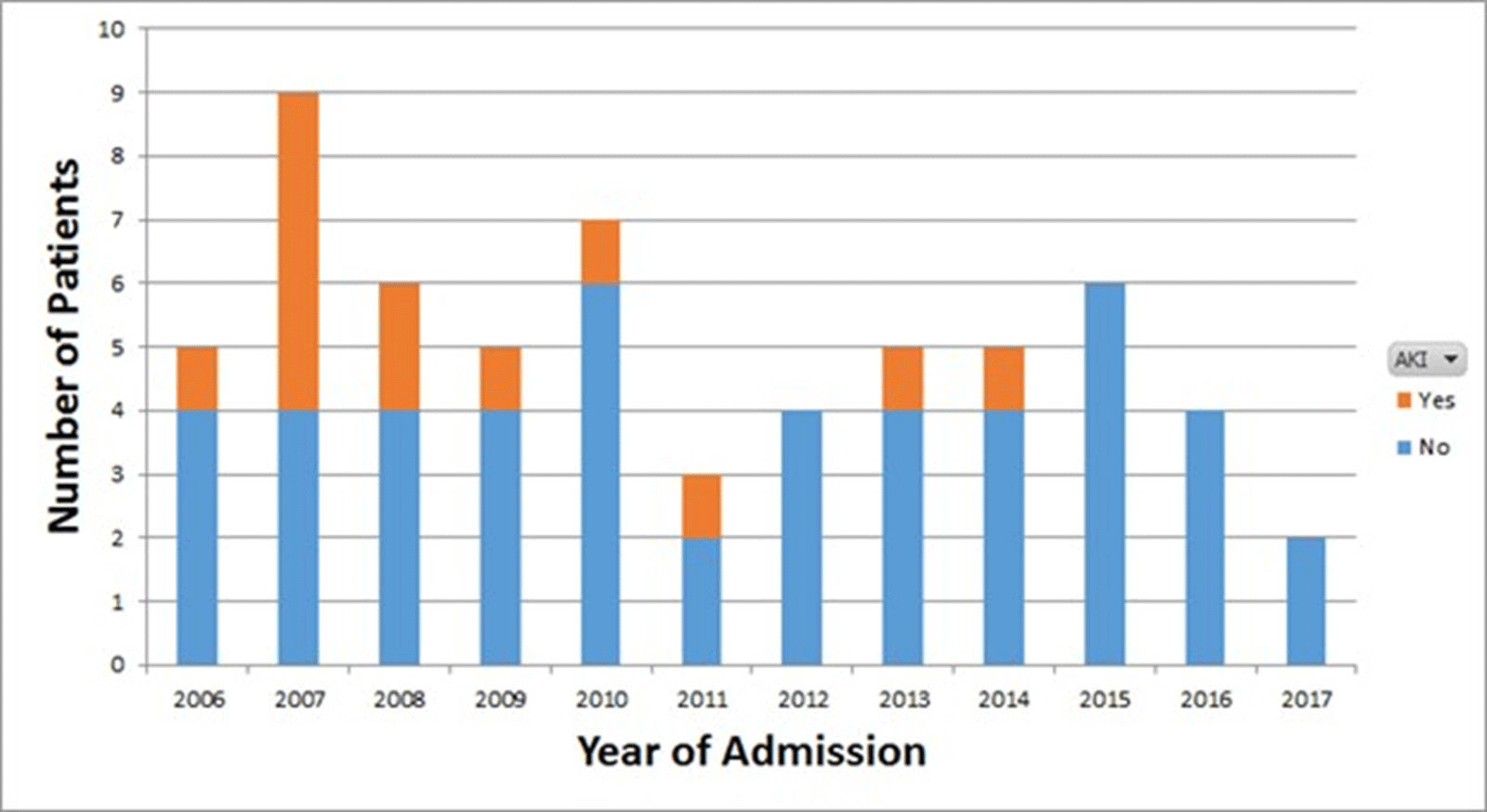
Background: Vancomycin is the treatment of choice for invasive methicillin-resistant Staphylococcus aureus (MRSA) infections. Previous guidelines issued by the Infectious Diseases Society of America (IDSA) recommended targeting vancomycin serum trough concentrations of 15–20 mg/L; however, troughs <15 mg/L are also associated with increased odds of renal toxicity. To minimize toxicity, recently updated ASHP/IDSA/PIDS vancomycin dosing guidelines recommend the use of an area under the vancomycin concentration-time curve divided by the minimum inhibitory concentration (AUC/MIC) pharmacodynamic index to measure vancomycin exposure, with an AUC/MIC ratio >400 correlating with clinical efficacy. However, data on vancomycin therapeutic drug monitoring (TDM) in children are limited. Our institutional practice since January 2009 has been to use AUC/MIC, rather than serum trough concentrations, to guide vancomycin dosing. In this study, we describe clinical outcomes in vancomycin-treated children with invasive MRSA infections using this dosing method. Methods: We performed a retrospective chart review of children hospitalized with invasive MRSA infections between 2006 and 2019 at Rady Children’s Hospital in San Diego, California. Clinical, microbiologic, and pharmacologic data including the site of MRSA infection, clinical failure or cure, occurrence of acute kidney injury (AKI), vancomycin MIC, vancomycin AUC, and serum trough concentrations were collected. Results: In total, 61 invasive MRSA cases were reviewed: 20 were admitted January 2016 through December 2008, and 41 were admitted January 2009 through June 2019 (Figure 1). Most patients did not have medical comorbidities. The most common types of infections were primary bacteremia (34%) and osteomyelitis (32%). Of 61 children, 50 (82%) had positive clinical outcomes regardless of vancomycin dosing method. Of 20 patients, 8 (40%) admitted prior to January 2009 developed AKI, compared with 5 (12%) of 41 patients admitted after January 2009. Conclusions: In our retrospective review, most patients had clinically successful outcomes regardless of which dosing strategy was used. We found higher rates of renal toxicity in patients who were admitted prior to 2009, with TDM based on measuring peak and trough concentrations, compared with those using AUC/MIC for TDM. Our findings suggest that AUC/MIC TDM for invasive MRSA infections may be associated with lower rates of renal toxicity.
Funding: No
Disclosures: None
Figure 1.

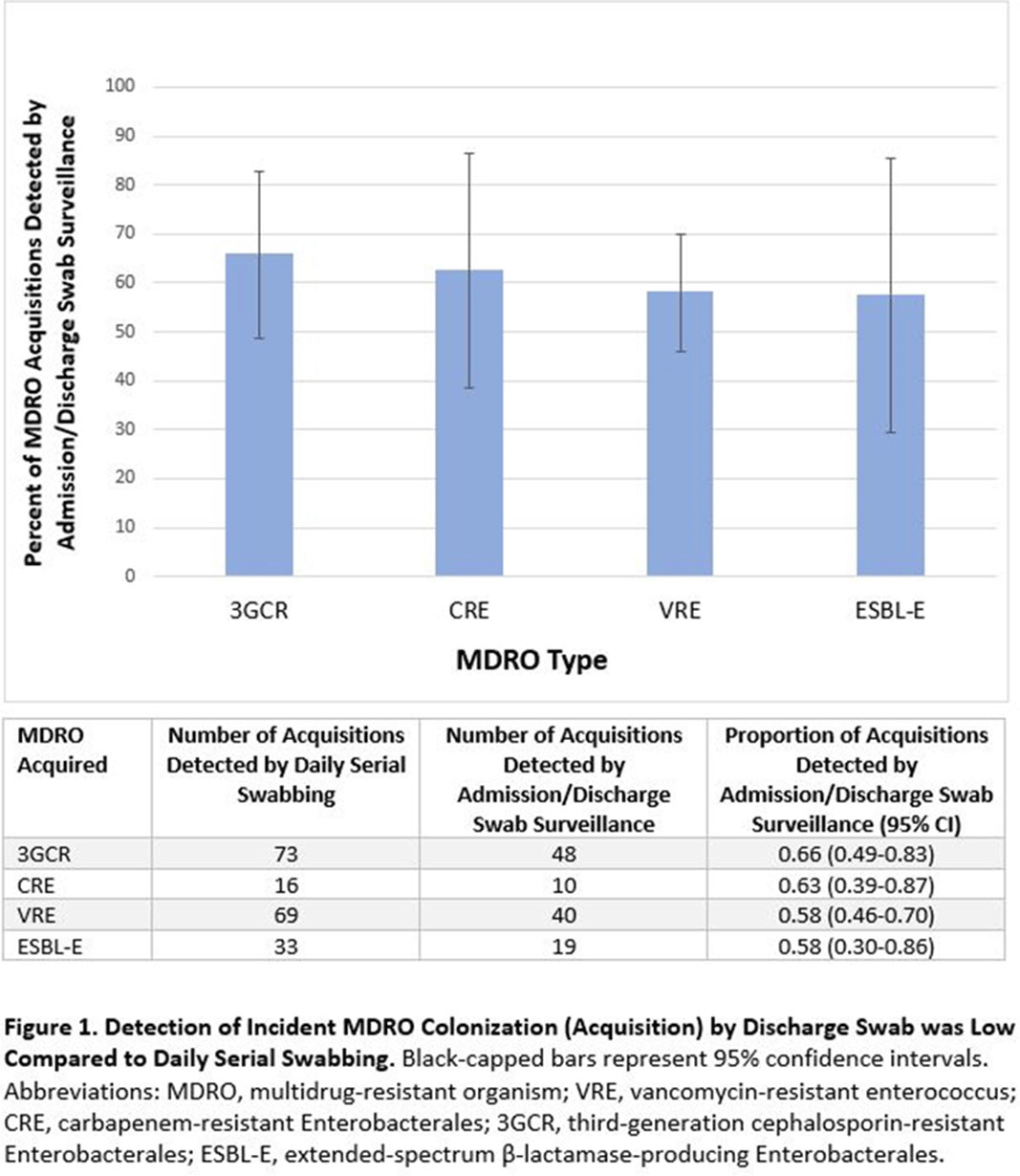
Admission and Discharge Sampling Underestimates Multidrug-Resistant Organism (MDRO) Acquisition in an Intensive Care Unit
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Identification of hospitalized patients with enteric multidrug-resistant organism (MDRO) carriage, combined with implementation of targeted infection control interventions, may help reduce MDRO transmission. However, the optimal surveillance approach has not been defined. We sought to determine whether daily serial rectal surveillance for MDROs detects more incident cases (acquisition) of MDRO colonization in medical intensive care unit (MICU) patients than admission and discharge surveillance alone. Methods: Prospective longitudinal observational single-center study from January 11, 2017, to January 11, 2018. Inclusion criteria were ≥3 consecutive MICU days and ≥2 rectal or stool swabs per MICU admission. Daily rectal or stool swabs were collected from patients and cultured for MDROs, including vancomycin-resistant Enterococcus (VRE), carbapenem-resistant Enterobacterales (CRE), third-generation cephalosporin-resistant Enterobacterales (3GCR), and extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E) (as a subset of 3GCR). MDRO detection at any time during the MICU stay was used to calculate prevalent colonization. Incident colonization (acquisition) was defined as new detection of an MDRO after at least 1 prior negative swab. We then determined the proportion of prevalent and incident cases detected by daily testing that were also detected when only first swabs (admission) and last swabs (discharge) were tested. Data were analyzed using SAS version 9.4 software. Results: In total, 939 MICU stays of 842 patients were analyzed. Patient characteristics were median age 64 years (interquartile range [IQR], 51–74), median MICU length of stay 5 days (IQR, 3–8), median number of samples per admission 3 (IQR, 2–5), and median Charlson index 4 (IQR, 2–7). Prevalent colonization with any MDRO was detected by daily swabbing in 401 stays (42.7%). Compared to daily serial swabbing, an admission- and discharge-only approach detected ≥86% of MDRO cases (ie, overall prevalent MDRO colonization). Detection of incident MDRO colonization by an admission- or discharge-only approach would have detected fewer cases than daily swabbing (Figure 1); ≥34% of total MDRO acquisitions would have been missed. Conclusions: Testing patients upon admission and discharge to an MICU may fail to detect MDRO acquisition in more than one-third of patients, thereby reducing the effectiveness of MDRO control programs that are targeted against known MDRO carriers. The poor performance of a single discharge swab may be due to intermittent or low-level MDRO shedding, inadequate sampling, or transient MDRO colonization. Additional research is needed to determine the optimal surveillance approach of enteric MDRO carriage.
Funding: No
Disclosures: None
Figure 1.