
102 results
Implementing a continuous quality-improvement framework for tuberculosis infection prevention and control in healthcare facilities in China, 2017–2019
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 25 January 2024, pp. 651-657
- Print publication:
- May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Northward migration of Red Knots Calidris canutus rufa and environment connectivity of southern Brazil to Canada
-
- Journal:
- Bird Conservation International / Volume 34 / 2024
- Published online by Cambridge University Press:
- 16 January 2024, e2
-
- Article
- Export citation
Severe and common mental disorders and risk of emergency hospital admissions for ambulatory care sensitive conditions among the UK Biobank cohort
-
- Journal:
- BJPsych Open / Volume 9 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 07 November 2023, e211
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Radiofrequency ice dielectric measurements at Summit Station, Greenland
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 09 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$
 –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

Impact of COVID-19 on healthcare-associated infections in Canadian acute-care hospitals: Interrupted time series (2018–2021)
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s112-s113
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Data regarding the effects of the SARS-COV-2 (COVID-19) pandemic on healthcare-associated infections (HAIs) in Canadian acute-care hospitals are limited. We examined the impact of the COVID-19 pandemic on HAIs and antimicrobial resistant organisms in hospitals participating in the Canadian Nosocomial Infection Surveillance Program. Methods: We analyzed 13,406 HAIs including adult mixed intensive care unit (ICU) central-line–associated bloodstream infections (CLABSIs), and healthcare-associated (HA) Clostridioides difficile infection (CDI), methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections (BSI), vancomycin-resistant Enterococcus (VRE) BSI, and carbapenemase-producing Enterobacterales (CPE) infections collected using standardized case definitions and questionnaires from 29–64 hospitals participating in the Canadian Nosocomial Infection Surveillance Program (CNISP) from January 2018 to December 2021. We used a generalized linear mixed model with quasi-Poisson distribution to assess step and slope changes in monthly HAI rates between the pre–COVID-19 pandemic period (January 1, 2018–February 29, 2020; 26 time points) and the COVID-19 pandemic period (March 1, 2020–December 31, 2021; 22 time points). Results were reported as incidence rate ratios (IRRs) with 95% confidence intervals (CIs) and adjusted for seasonality, hospital clustering, and hospital characteristics of interest. Results: In the CNISP network, 7,352 (55%) HAIs were reported in the prepandemic period and 6,054 (45%) in the pandemic period. Median age was significantly younger during the pandemic period compared to the prepandemic period among patients with HA-CDI, HA-MRSA BSI, and adult mixed ICU CLABSIs, and more than half of cases among all reported HAIs were male (range, 52%–65%). The 30-day all-cause in-hospital mortality rate did not significantly change between the prepandemic and pandemic periods for all reported HAIs and was highest among HA-VRE BSIs (34%). Modeling results indicated that the COVID-19 pandemic was associated with an immediate increase in HA-CDI and adult mixed ICU CLABSI rates whereas HA-MRSA BSI, HA-CPE and HA-VRE BSI rates immediately decreased. However, pandemic status did not have a statistically significant lasting impact on monthly rate trends for all reported HAIs after adjusting for seasonality, clustering, and hospital covariates (Fig. 1 and 2). Adjusted IRRs for all HAIs ranged from 1.00 to 1.01 (95% CI, 0.94–0.99 to 1.01–1.05).
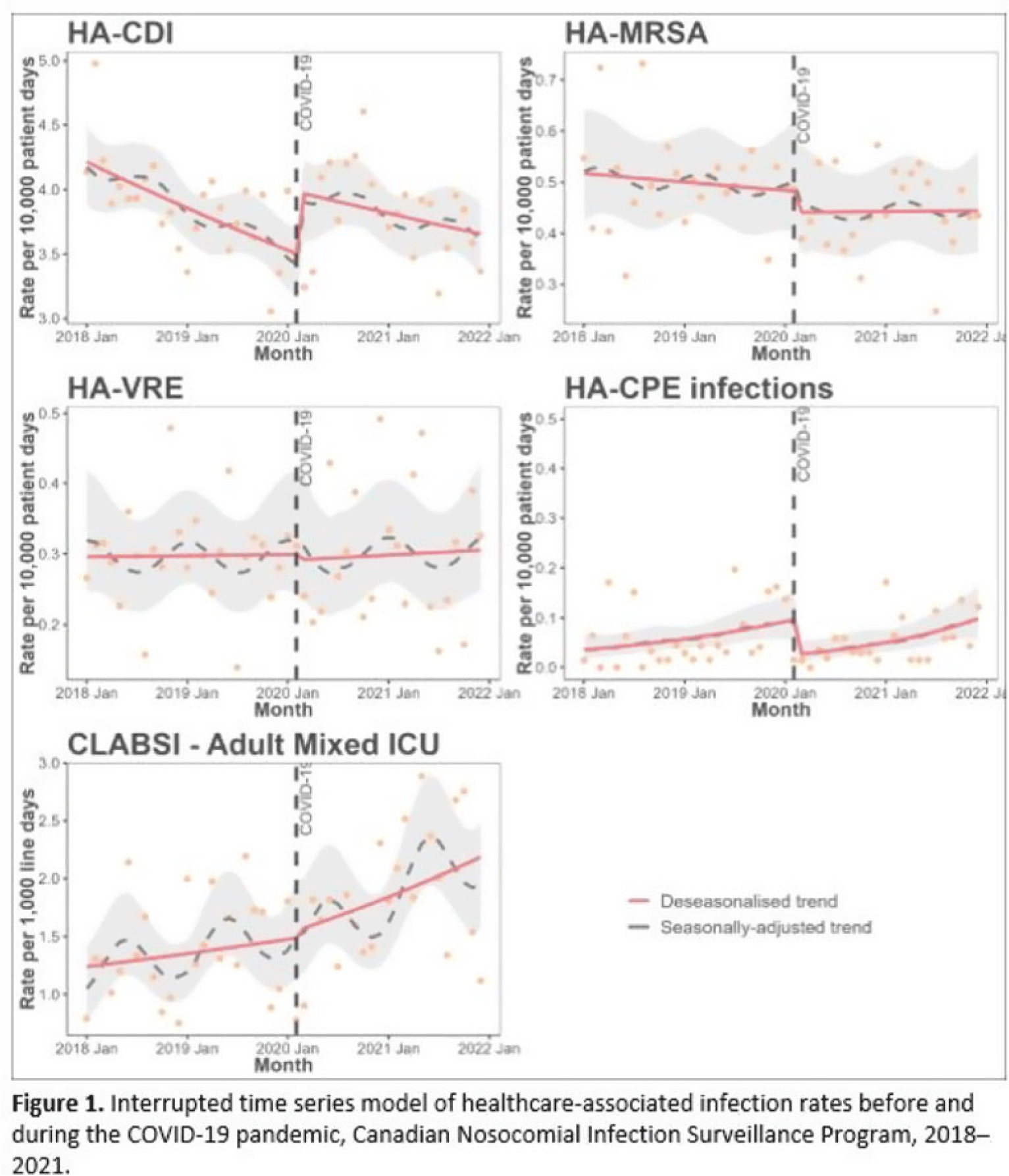
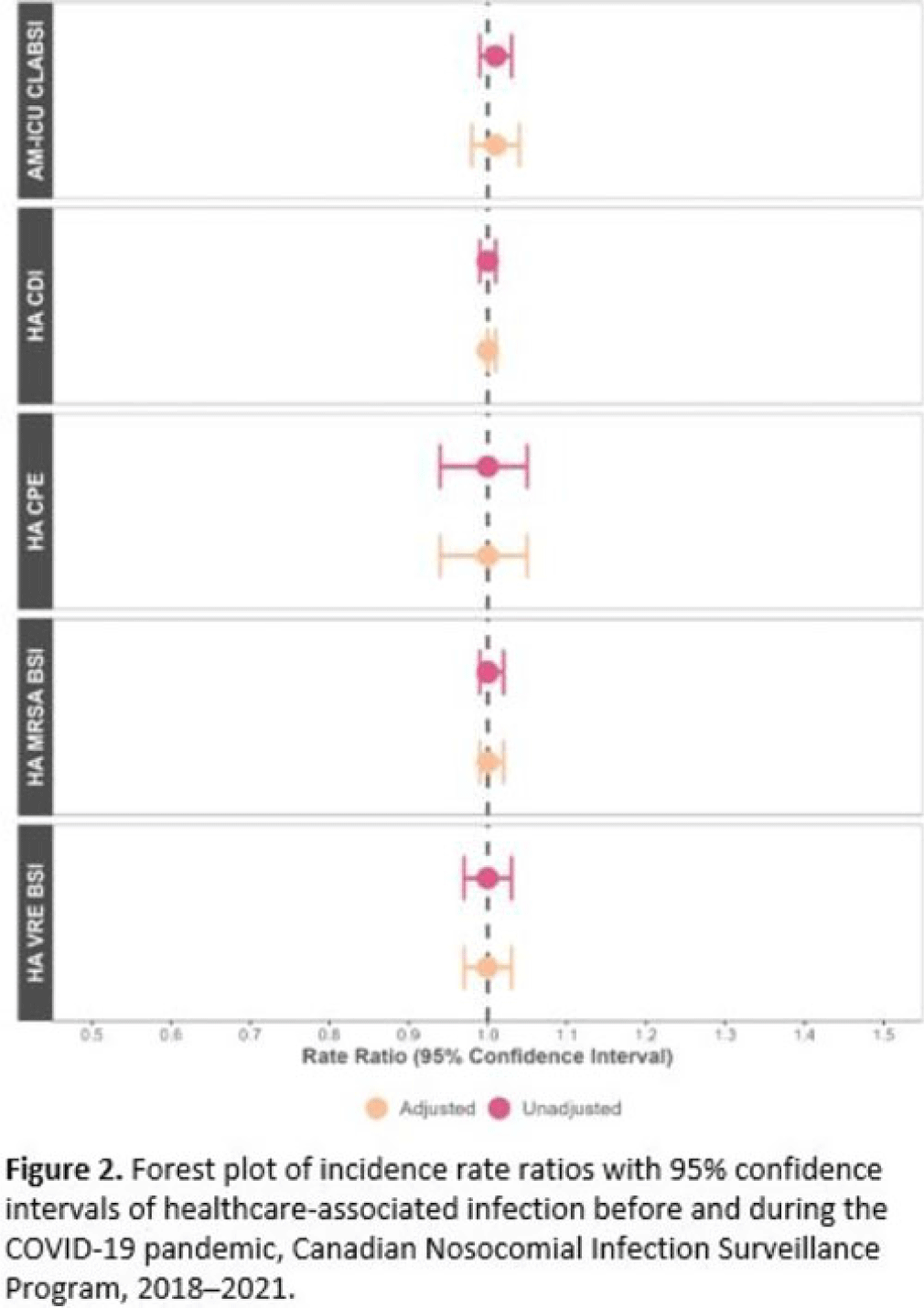 Conclusions: Although the COVID-19 pandemic placed a significant burden on the Canadian healthcare system, the immediate impact on monthly rates of HAIs in Canadian acute-care hospitals was not sustained over time. Understanding the epidemiological effects of the COVID-19 pandemic in the context of changing patient populations, and clinical and infection control practices, are essential to inform the continued management and prevention of HAIs in Canadian acute-care settings.
Conclusions: Although the COVID-19 pandemic placed a significant burden on the Canadian healthcare system, the immediate impact on monthly rates of HAIs in Canadian acute-care hospitals was not sustained over time. Understanding the epidemiological effects of the COVID-19 pandemic in the context of changing patient populations, and clinical and infection control practices, are essential to inform the continued management and prevention of HAIs in Canadian acute-care settings.Disclosures: None


Epidemiology of central-line–associated bloodstream infection mortality in Canadian NICUs before and after 2017
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
How does the antimicrobial stewardship provider role affect prospective audit and feedback acceptance for restricted antibiotics in a Canadian tertiary-care center?
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 18 August 2023, pp. 234-236
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
19 - Temperament, Family Context, and the Development of Coping
- from Part V - Social Contexts and the Development of Coping
-
-
- Book:
- The Cambridge Handbook of the Development of Coping
- Published online:
- 22 June 2023
- Print publication:
- 06 July 2023, pp 468-488
-
- Chapter
- Export citation
Complex cardiac implantable electronic device infections in Alberta, Canada: An epidemiologic cohort study of validated administrative data
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 15 May 2023, pp. 1607-1613
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
294 Identification of MCAK Inhibitors that Induce Aneuploidy in Triple Negative Breast Cancer Models
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, p. 88
-
- Article
-
- You have access
- Open access
- Export citation
What Do You Do When You Can Do No More? Limited Resources, Unimaginable Environments, Personal Danger: What Have Previous Disasters Taught Us About Moral and Ethical Challenges?
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 11 April 2023, e373
-
- Article
- Export citation
Developmental care pathway for hospitalised infants with CHD: on behalf of the Cardiac Newborn Neuroprotective Network, a Special Interest Group of the Cardiac Neurodevelopmental Outcome Collaborative
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 30 March 2023, pp. 2521-2538
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Expanding mental health services in low- and middle-income countries: A task-shifting framework for delivery of comprehensive, collaborative, and community-based care
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 10 / 2023
- Published online by Cambridge University Press:
- 27 February 2023, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
10 - Parenting That Promotes Positive Social, Emotional and Behavioral Development in Middle Childhood
- from Part II - Parenting across Development: Social, Emotional, and Cognitive Influences
-
-
- Book:
- The Cambridge Handbook of Parenting
- Published online:
- 01 December 2022
- Print publication:
- 15 December 2022, pp 213-235
-
- Chapter
- Export citation
Relationship building in pediatric research recruitment: Insights from qualitative interviews with research staff
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 03 October 2022, e138
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Mobilizing digital technology to implement a population-based psychological support response during the COVID-19 pandemic in Lima, Peru
-
- Journal:
- Global Mental Health / Volume 9 / 2022
- Published online by Cambridge University Press:
- 28 July 2022, pp. 355-365
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Participation in cost-offset community-supported agriculture by low-income households in the USA is associated with community characteristics and operational practices
-
- Journal:
- Public Health Nutrition / Volume 25 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 13 April 2022, pp. 2277-2287
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Acceptability and experience of a personalised proteomic risk intervention for type 2 diabetes in primary care: qualitative interview study with patients and healthcare providers
-
- Journal:
- Primary Health Care Research & Development / Volume 23 / 2022
- Published online by Cambridge University Press:
- 01 April 2022, e24
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Vancomycin-resistant Enterococcus sequence type 1478 spread across hospitals participating in the Canadian Nosocomial Infection Surveillance Program from 2013 to 2018
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 10 March 2022, pp. 17-23
- Print publication:
- January 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comparison of the performance of a clinical classification tree versus clinical gestalt in predicting sepsis with extended-spectrum beta-lactamase–producing gram-negative rods
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 07 March 2022, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
