
55 results
Deep neural networks are not a single hypothesis but a language for expressing computational hypotheses
-
- Journal:
- Behavioral and Brain Sciences / Volume 46 / 2023
- Published online by Cambridge University Press:
- 06 December 2023, e392
-
- Article
- Export citation
How Divided Is Britain? Symbolic Boundaries and Social Cohesion in Post-Brexit Britain
-
- Journal:
- PS: Political Science & Politics / Volume 56 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 10 August 2023, pp. 553-559
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Factor structure of the Harmonized Cognitive Assessment Protocol neuropsychological battery in the Health and Retirement Study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 14 July 2023, pp. 47-55
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Significantly improved outcomes – both in retention and CGI scores - using Long Acting Buprenorphine (LAB-Buvidal) versus treatment as usual for Opioid Dependence in Wales during the Pandemic
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S814
-
- Article
-
- You have access
- Open access
- Export citation
Using gamification to enhance clinical trial start-up activities
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 19 May 2022, e75
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
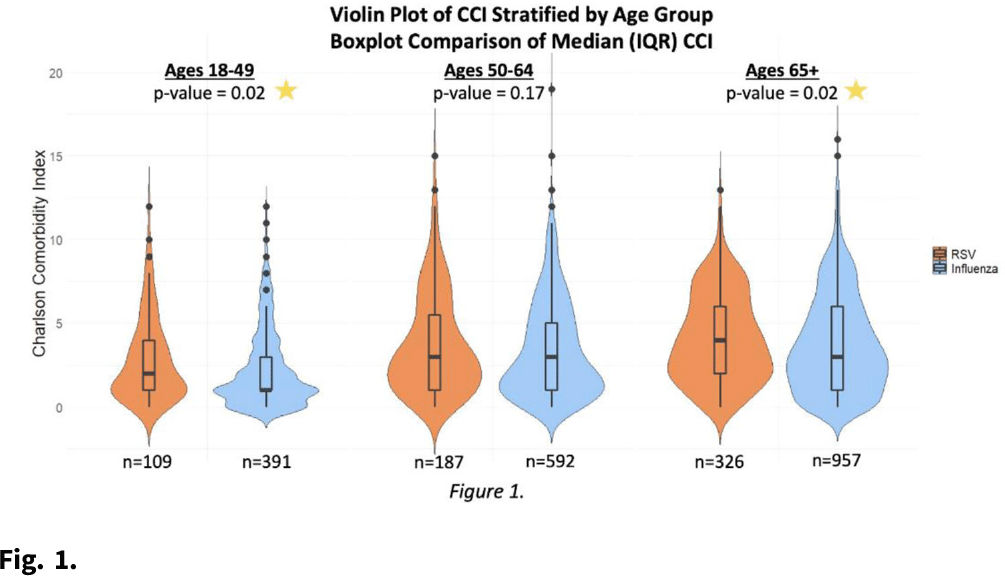
Relevance of RSV in hospitalized adults and the need for continued testing
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s62
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: RSV is underrecognized in hospitalized adults. A better understanding of RSV in this population could help prioritize targeted viral-testing resources. Hospitalization and in-hospital outcomes are widely accepted as markers of clinical severity with respect to acute respiratory illness (ARI). We compared characteristics and clinical outcomes between adults hospitalized with ARI from October 2016 through May 2019. Methods: All hospitalized adults (≥ 18 years) who met a standardized case definition of ARI were prospectively enrolled across 3 respiratory seasons from 9 hospitals participating in the US Hospitalized Adult Influenza Vaccine Effectiveness Network (HAIVEN). Demographic data were collected during enrollment interviews, and electronic medical records (EMRs) were reviewed to extract comorbidity data. Throat and nasal swabs collected at enrollment were tested for ARI pathogens using real-time PCR assays at respective HAIVEN research laboratory sites. Characteristics and clinical outcomes of participants were compared using χ2 or nonparametric tests where appropriate. Multivariable logistic regression models were used to test associations between infection status, characteristics, and clinical outcomes, adjusting for age, sex, race, Charlson comorbidity index (CCI), body mass index (BMI), site, season, and days to admission. Results: In total, 10,311 adults were included, 22.3% (n = 2,300) were aged 18–49 years, 33.2% (n = 3,423) were aged 50–64 years, and 44.5% (n = 4,588) were aged ≥65 years. Moreover, 6% of adults tested positive for RSV (n = 622), 18.8% positive for influenza (n = 1,940), and 75.1% negative for both (n = 7,749). Obesity and age ≥65 years were significantly associated with RSV detection when compared with participants negative for both RSV and influenza. Patients aged 18–49 years and ≥65 years with RSV had significantly higher median CCI scores compared to patients with influenza (Fig. 1.). The proportion of adults with CHF or COPD was significantly (p-value Conclusions: Severe RSV illness may differ from severe influenza illness, and those infected with RSV may have different characteristics than those infected with influenza. Hospitalized adults with RSV infection were more likely to have underlying cardiopulmonary comorbidities and higher CCI scores as well as experience an extended length of hospital stay and need for mechanical ventilation. These data highlight the importance of retaining testing for RSV in older adults hospitalized with ARI.
Funding: None
Disclosures: None

Investigating Space Weathering Effects on Carbonaceous Asteroids Using High-flux and Low-flux Ion Irradiation of the Murchison Meteorite
-
- Journal:
- Microscopy and Microanalysis / Volume 27 / Issue S1 / August 2021
- Published online by Cambridge University Press:
- 30 July 2021, pp. 2538-2541
- Print publication:
- August 2021
-
- Article
-
- You have access
- Export citation
Prevalence and 1-year incidence of HIV-associated neurocognitive disorder (HAND) in adults aged ≥50 years attending standard HIV clinical care in Kilimanjaro, Tanzania
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 24 March 2021, pp. 339-350
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Deep hypothermic circulatory arrest in cyanotic piglets is associated with increased neuronal necrosis
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 23 December 2020, pp. 769-774
-
- Article
- Export citation
Pilot study of a combined genomic and epidemiologic surveillance program for hospital-acquired multidrug-resistant pathogens across multiple hospital networks in Australia
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 26 November 2020, pp. 573-581
- Print publication:
- May 2021
-
- Article
-
- You have access
- HTML
- Export citation
Reduction in Stroke After Transient Ischemic Attack in a Province-Wide Cohort Between 2003 and 2015
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 48 / Issue 3 / May 2021
- Published online by Cambridge University Press:
- 22 September 2020, pp. 335-343
-
- Article
-
- You have access
- HTML
- Export citation
Investigating Space Weathering Effects Using Coordinated Analysis of a H+- and He+-Irradiated Carbonaceous Chondrite
-
- Journal:
- Microscopy and Microanalysis / Volume 26 / Issue S2 / August 2020
- Published online by Cambridge University Press:
- 30 July 2020, pp. 2598-2601
- Print publication:
- August 2020
-
- Article
-
- You have access
- Export citation
Call 911: Lower Ambulance Utilization Among Young Adults, Especially Women, with Stroke
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 47 / Issue 6 / November 2020
- Published online by Cambridge University Press:
- 08 June 2020, pp. 764-769
-
- Article
-
- You have access
- HTML
- Export citation
Implementing a 2019 coronavirus disease airway management strategy for a provincial critical care and ground transport program
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 22 / Issue S2 / September 2020
- Published online by Cambridge University Press:
- 03 June 2020, pp. S104-S107
- Print publication:
- September 2020
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Comprehensive Assessment of Neurodegeneration and Dementia: Canadian Cohort Study
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 46 / Issue 5 / September 2019
- Published online by Cambridge University Press:
- 16 July 2019, pp. 499-511
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characterizing the Effects of Sex, APOE ɛ4, and Literacy on Mid-life Cognitive Trajectories: Application of Information-Theoretic Model Averaging and Multi-model Inference Techniques to the Wisconsin Registry for Alzheimer’s Prevention Study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 25 / Issue 2 / February 2019
- Published online by Cambridge University Press:
- 07 December 2018, pp. 119-133
-
- Article
- Export citation
Longitudinal Standards for Mid-life Cognitive Performance: Identifying Abnormal Within-Person Changes in the Wisconsin Registry for Alzheimer’s Prevention
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 25 / Issue 1 / January 2019
- Published online by Cambridge University Press:
- 28 November 2018, pp. 1-14
-
- Article
- Export citation
Coordinated Analyses of the Chemical and Microstructural Effects of Progressive Space Weathering of a Carbonaceous Chondrite
-
- Journal:
- Microscopy and Microanalysis / Volume 24 / Issue S1 / August 2018
- Published online by Cambridge University Press:
- 01 August 2018, pp. 2118-2119
- Print publication:
- August 2018
-
- Article
-
- You have access
- Export citation
Outcomes in Hospitalized Ischemic Stroke Patients with Dementia on Admission: A Population-Based Cohort Study
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 45 / Issue 3 / May 2018
- Published online by Cambridge University Press:
- 16 April 2018, pp. 290-294
-
- Article
-
- You have access
- HTML
- Export citation
9 - Urban Areas in Coastal Zones
- from Part II - Urban Ecosystems and Human Services
-
-
- Book:
- Climate Change and Cities
- Published online:
- 12 April 2018
- Print publication:
- 29 March 2018, pp 319-362
-
- Chapter
- Export citation
