
546 results
Clinical and Genomic Characteristics of Candida auris in Central Ohio: An Insight into Epidemiological Surveillance
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s93
-
- Article
-
- You have access
- Open access
- Export citation
-
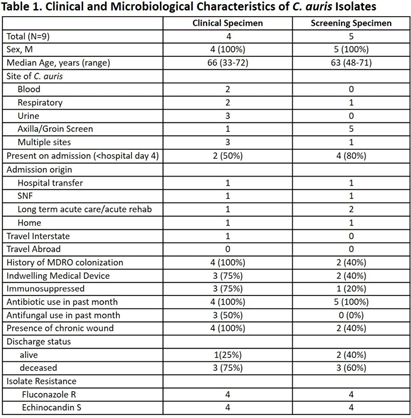
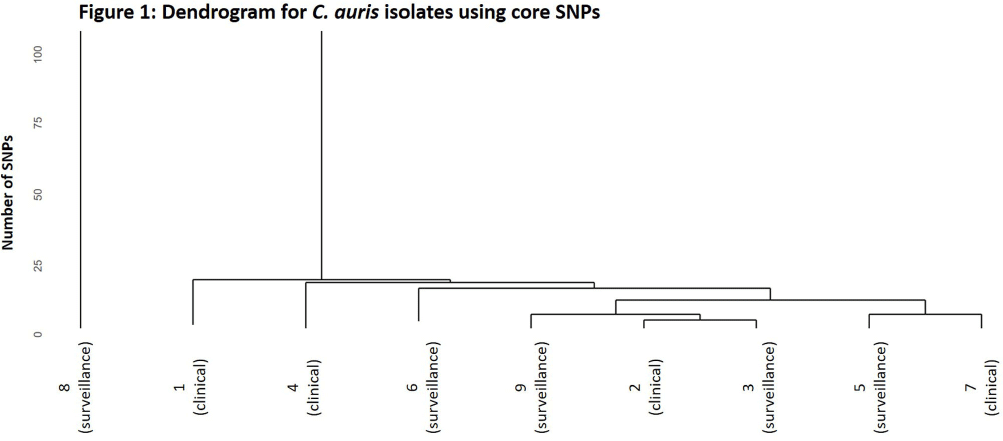
Background: Candida auris is an emerging threat to hospitalized patients and invasive disease is associated with high mortality. This study describes clinical and microbiological characteristics of nine patients identified with C. auris at Ohio State Wexner Medical Center discovered through active surveillance or clinical investigation and uses whole genome sequencing (WGS) to compare isolates. Methods: In November 2022, an active C. auris surveillance program was implemented to screen patients admitted to high-risk units (intensive care units and progressive care units). Bilateral axilla and groin swabs were obtained upon unit admission and, if positive, were submitted for C. auris polymerase chain reaction (PCR) with culture and sensitivity testing. Patients with a positive screening or clinical isolate from November 2022 to November 2023 underwent chart review for clinical characteristics, microbiologic data, and index admission information. For each isolate, DNA was extracted and WGS was performed. Core single nucleotide polymorphism (SNP) variation identified from the sequence data was used to infer genetic relationships among the isolates. Results: Nine patients were identified between November 2022 and November 2023. The clinical and microbiologic characteristics are summarized in Table 1. All patients were hospitalized at various acute care facilities across the state at least once in the preceding 12 months. C. auris was determined to be present on admission for 6 patients. For 5 of these patients, it was their first interaction with our healthcare system. Three patients were not in contact isolation for >3 days before C. auris was identified. Unit wide point-prevalence screening was completed in these cases and no evidence of transmission was found. WGS showed eight of the nine isolates were related with 28 or less core SNP differences between isolates (Figure 1). One isolate (8) was genetically distinct with >45000 core SNP differences. Five isolates were highly related with a range of 4-15 SNP differences. No temporal or spatial overlap at our institution was identified among these five patients. Conclusions: The active surveillance program identified several patients colonized with C. auris in addition to those found through clinical testing. Multiple risk factors for C. auris were identified with high patient mortality (67%). Majority of the isolates were closely related without association with a known outbreak or epidemiologic link, suggesting a possible diffuse common reservoir. Next steps with surveillance in acute care and long-term care facilities will be critical for early detection to halt transmission of this organism.


A short proof of the Hanlon-Hicks-Lazarev Theorem
- Part of
-
- Journal:
- Forum of Mathematics, Sigma / Volume 12 / 2024
- Published online by Cambridge University Press:
- 10 May 2024, e56
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
3 - ‘A traitor to the kingdom’: Robert Bruce and the Use of Treason in Fourteenth-Century Scotland
-
-
- Book:
- Rethinking the Renaissance and Reformation in Scotland
- Published by:
- Boydell & Brewer
- Published online:
- 16 May 2024
- Print publication:
- 05 March 2024, pp 61-80
-
- Chapter
- Export citation
EMU/GAMA: A technique for detecting active galactic nuclei in low mass systems
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 41 / 2024
- Published online by Cambridge University Press:
- 21 February 2024, e016
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We propose a new method for identifying active galactic nuclei (AGN) in low mass (
 $\mathrm{M}_*\leq10^{10}\mathrm{M}_\odot$) galaxies. This method relies on spectral energy distribution (SED) fitting to identify galaxies whose radio flux density has an excess over that expected from star formation alone. Combining data in the Galaxy and Mass Assembly (GAMA) G23 region from GAMA, Evolutionary Map of the Universe (EMU) early science observations, and Wide-field Infrared Survey Explorer (WISE), we compare this technique with a selection of different AGN diagnostics to explore the similarities and differences in AGN classification. We find that diagnostics based on optical and near-infrared criteria (the standard BPT diagram, the WISE colour criterion, and the mass-excitation, or MEx diagram) tend to favour detection of AGN in high mass, high luminosity systems, while the “ProSpect” SED fitting tool can identify AGN efficiently in low mass systems. We investigate an explanation for this result in the context of proportionally lower mass black holes in lower mass galaxies compared to higher mass galaxies and differing proportions of emission from AGN and star formation dominating the light at optical and infrared wavelengths as a function of galaxy stellar mass. We conclude that SED-derived AGN classification is an efficient approach to identify low mass hosts with low radio luminosity AGN.
$\mathrm{M}_*\leq10^{10}\mathrm{M}_\odot$) galaxies. This method relies on spectral energy distribution (SED) fitting to identify galaxies whose radio flux density has an excess over that expected from star formation alone. Combining data in the Galaxy and Mass Assembly (GAMA) G23 region from GAMA, Evolutionary Map of the Universe (EMU) early science observations, and Wide-field Infrared Survey Explorer (WISE), we compare this technique with a selection of different AGN diagnostics to explore the similarities and differences in AGN classification. We find that diagnostics based on optical and near-infrared criteria (the standard BPT diagram, the WISE colour criterion, and the mass-excitation, or MEx diagram) tend to favour detection of AGN in high mass, high luminosity systems, while the “ProSpect” SED fitting tool can identify AGN efficiently in low mass systems. We investigate an explanation for this result in the context of proportionally lower mass black holes in lower mass galaxies compared to higher mass galaxies and differing proportions of emission from AGN and star formation dominating the light at optical and infrared wavelengths as a function of galaxy stellar mass. We conclude that SED-derived AGN classification is an efficient approach to identify low mass hosts with low radio luminosity AGN.

Predictors of primary care psychological therapy outcomes for depression and anxiety in people living with dementia: evidence from national healthcare records in England
-
- Journal:
- The British Journal of Psychiatry / Volume 224 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 08 February 2024, pp. 205-212
- Print publication:
- June 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Creating shared goals and experiences as a pathway to peace
-
- Journal:
- Behavioral and Brain Sciences / Volume 47 / 2024
- Published online by Cambridge University Press:
- 15 January 2024, e5
-
- Article
-
- You have access
- HTML
- Export citation
Incidence and risk factors for catheter-associated urinary tract infection in 623 intensive care units throughout 37 Asian, African, Eastern European, Latin American, and Middle Eastern nations: A multinational prospective research of INICC
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 04 January 2024, pp. 567-575
- Print publication:
- May 2024
-
- Article
-
- You have access
- HTML
- Export citation
8 A Feasibility Study of a Virtually-Delivered Ecologically-Oriented Neurorehabilitation of Memory (EON-MEM) Protocol in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 886-887
-
- Article
-
- You have access
- Export citation
Radio continuum from the most massive early-type galaxies detected with ASKAP RACS
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 41 / 2024
- Published online by Cambridge University Press:
- 15 December 2023, e004
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
All very massive early-type galaxies contain supermassive blackholes, but are these blackholes all sufficiently active to produce detectable radio continuum sources? We have used the 887.5 MHz Rapid ASKAP Continuum Survey DR1 to measure the radio emission from morphological early-type galaxies brighter than
 $K_S=9.5$ selected from the 2MASS Redshift Survey, HyperLEDA, and RC3. In line with previous studies, we find median radio power increases with infrared luminosity, with
$K_S=9.5$ selected from the 2MASS Redshift Survey, HyperLEDA, and RC3. In line with previous studies, we find median radio power increases with infrared luminosity, with  $P_{1.4} \propto L_K^{2.2}$, although the scatter about this relation spans several orders of magnitude. All 40 of the
$P_{1.4} \propto L_K^{2.2}$, although the scatter about this relation spans several orders of magnitude. All 40 of the  $M_K<-25.7$ early-type galaxies in our sample have measured radio flux densities that are more than
$M_K<-25.7$ early-type galaxies in our sample have measured radio flux densities that are more than  $2\sigma$ above the background noise, with
$2\sigma$ above the background noise, with  $1.4\,{\rm GHz}$ radio powers spanning
$1.4\,{\rm GHz}$ radio powers spanning  ${\sim} 3 \times 10^{20}$ to
${\sim} 3 \times 10^{20}$ to  ${\sim} 3\times 10^{25}\,{\rm W/Hz^{-1}}$. Cross-matching our sample with integral field spectroscopy of early-type galaxies reveals that the most powerful radio sources preferentially reside in galaxies with relatively low angular momentum (i.e. slow rotators). While the infrared colours of most galaxies in our early-type sample are consistent with passive galaxies with negligible star formation and the radio emission produced by active galactic nuclei or AGN remnants, very low levels of star formation could power the weakest radio sources with little effect on many other star formation rate tracers.
${\sim} 3\times 10^{25}\,{\rm W/Hz^{-1}}$. Cross-matching our sample with integral field spectroscopy of early-type galaxies reveals that the most powerful radio sources preferentially reside in galaxies with relatively low angular momentum (i.e. slow rotators). While the infrared colours of most galaxies in our early-type sample are consistent with passive galaxies with negligible star formation and the radio emission produced by active galactic nuclei or AGN remnants, very low levels of star formation could power the weakest radio sources with little effect on many other star formation rate tracers.







Perceptions, barriers and enablers on salt reduction in the out-of-home sectors in Malaysia (MySaltOH) from the perspective of street food vendors, caterers and consumers
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 15 December 2023, e12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A POSSIBLE PARTHIAN-ERA ANAHITA SANCTUARY AT RABANA IN THE KURDISTAN REGION OF IRAQ
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Depression is associated with reduced outcome sensitivity in a dual valence, magnitude learning task – ADDENDUM
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 3 / February 2024
- Published online by Cambridge University Press:
- 24 November 2023, p. 637
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Pilot study of a ketogenic diet in bipolar disorder
-
- Journal:
- BJPsych Open / Volume 9 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 10 October 2023, e176
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Depression is associated with reduced outcome sensitivity in a dual valence, magnitude learning task
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 3 / February 2024
- Published online by Cambridge University Press:
- 14 September 2023, pp. 631-636
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
ON THE EXPECTED UNIFORM ERROR OF BROWNIAN MOTION APPROXIMATED BY THE LÉVY–CIESIELSKI CONSTRUCTION
- Part of
-
- Journal:
- Bulletin of the Australian Mathematical Society / Volume 109 / Issue 3 / June 2024
- Published online by Cambridge University Press:
- 24 August 2023, pp. 581-593
- Print publication:
- June 2024
-
- Article
-
- You have access
- HTML
- Export citation
-
The Brownian bridge or Lévy–Ciesielski construction of Brownian paths almost surely converges uniformly to the true Brownian path. We focus on the uniform error. In particular, we show constructively that at level N, at which there are
 $d=2^N$ points evaluated on the Brownian path, the uniform error and its square, and the uniform error of geometric Brownian motion, have upper bounds of order
$d=2^N$ points evaluated on the Brownian path, the uniform error and its square, and the uniform error of geometric Brownian motion, have upper bounds of order  $\mathcal {O}(\sqrt {\ln d/d})$, matching the known orders. We apply the results to an option pricing example.
$\mathcal {O}(\sqrt {\ln d/d})$, matching the known orders. We apply the results to an option pricing example.


Assessing enrollment of eligible infants in the national pediatric cardiology quality improvement collaborative (NPC-QIC) through linkage to the pediatric cardiac critical care consortium (PC4) registry
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 12 July 2023, pp. 373-379
-
- Article
-
- You have access
- HTML
- Export citation
Race, Property, and Erasure in the Rust Belt: Viewing Urban Changes through a Binocular Colonial Lens
-
- Journal:
- Du Bois Review: Social Science Research on Race / Volume 20 / Issue 2 / Fall 2023
- Published online by Cambridge University Press:
- 08 May 2023, pp. 311-332
-
- Article
-
- You have access
- HTML
- Export citation
249 Addressing Structural Racism Using Community Based System Dynamics
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, pp. 76-77
-
- Article
-
- You have access
- Open access
- Export citation
Searching for the “native” speaker: A preregistered conceptual replication and extension of Reid, Trofimovich, and O’Brien (2019)
-
- Journal:
- Applied Psycholinguistics / Volume 44 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 March 2023, pp. 475-494
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sister Space: Collective Descriptive Representation and Black Women in Legislative Caucuses
-
- Journal:
- Politics & Gender / Volume 19 / Issue 4 / December 2023
- Published online by Cambridge University Press:
- 15 March 2023, pp. 1234-1238
-
- Article
-
- You have access
- HTML
- Export citation
