
71 results
Associations between disturbed sleep and attenuated psychotic experiences in people at clinical high risk for psychosis
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 07 March 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Endocannabinoid levels in plasma and neurotransmitters in the brain: a preliminary report on patients with a psychotic disorder and healthy individuals
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 23 February 2024, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cannabis use as a potential mediator between childhood adversity and first-episode psychosis: results from the EU-GEI case–control study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 04 May 2023, pp. 7375-7384
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Tobacco use in first-episode psychosis, a multinational EU-GEI study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 26 April 2023, pp. 7265-7276
-
- Article
- Export citation
Genetic and psychosocial stressors have independent effects on the level of subclinical psychosis: findings from the multinational EU-GEI study
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 31 / 2022
- Published online by Cambridge University Press:
- 27 September 2022, e68
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Predictive biomarkers for negative symptoms in schizophrenia
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S132-S133
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Increasing evidence shows that impaired neuroplasticity and high inflammation play a crucial role in the pathophysiology of schizophrenia. Prospective studies demonstrated that patients with high inflammation usually have a poor treatment response and clinical practice learns that negative symptoms are challenging to treat. The predictive value of biomarkers for negative symptoms in patients with schizophrenia has sparsely been explored.
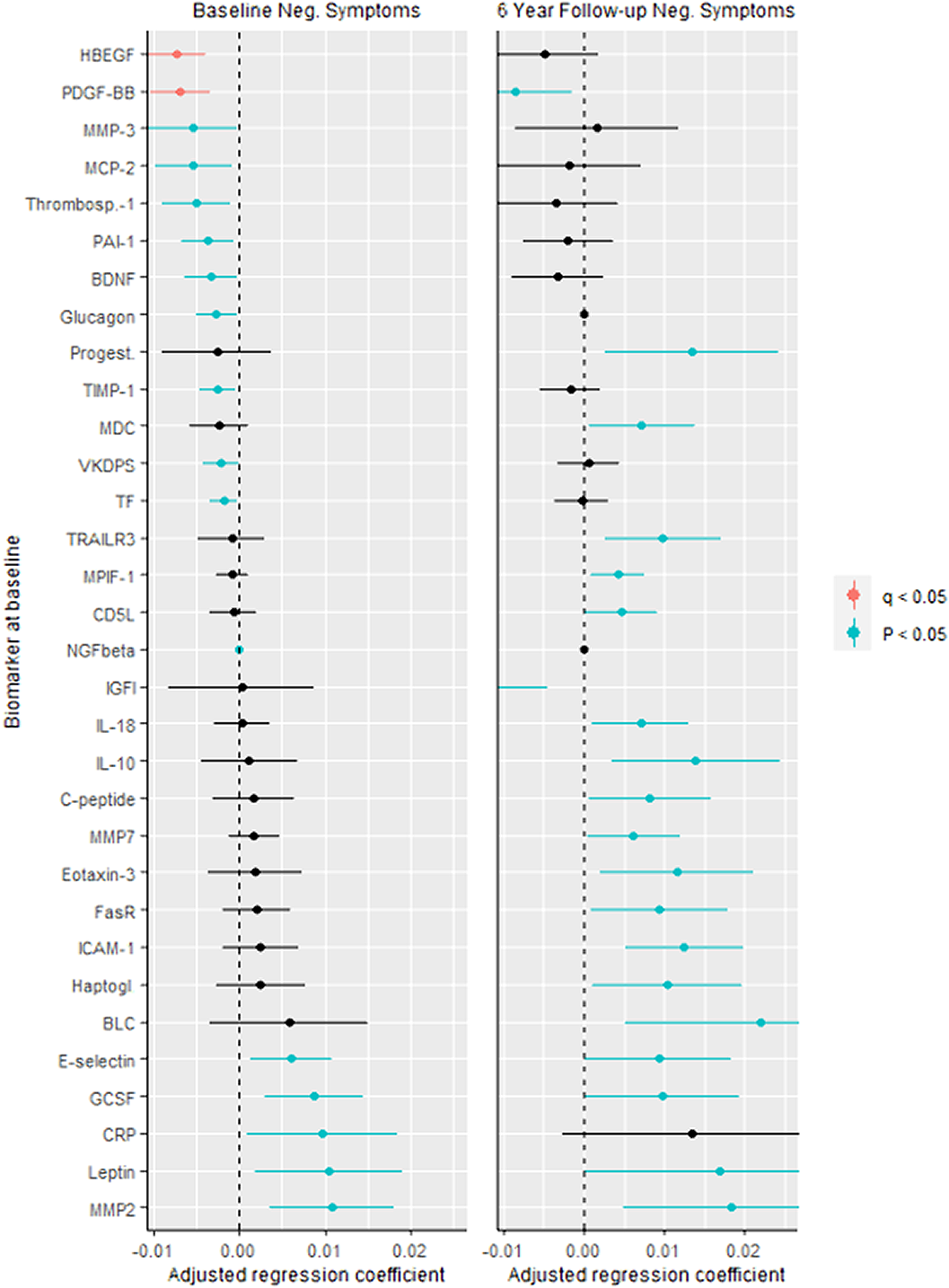
ObjectivesHere, we investigated whether biomarkers are associated with negative symptoms at baseline, and whether biomarkers could predict negative symptoms after six years in patients with schizophrenia.
MethodsWe investigated serum biomarkers in an epidemiological study on schizophrenia (N, baseline=110; N, follow-up=65). Negative symptoms were measured using the Positive and Negative Syndrome Scale. Biomarkers (N=189) were measured with a multi-analyte profiling platform and analysed using linear regression models, adjusted for site, age, gender, ethnicity, anti-inflammatory agents, smoking, cardiovascular disease and diabetes, and adjusted for multiple comparisons (q, Benjamini-Hochberg procedure).
ResultsIn particular, decreased platelet-derived growth factor (PDGF) (responsible for proliferation of oligodendrocytes) was associated with more negative symptoms at baseline and follow-up (figure). Several other biomarkers associated with inflammation, neuroplasticity and metabolism correlated with the severity of negative symptoms cross-sectionally and/or prospectively. Figure. Biomarkers for Negative Symptoms in Schizophrenia.
 Conclusions
ConclusionsAlthough our sample size at follow-up was limited, we feel that these analyses contribute to further research of possible predictive biomarkers for negative symptoms in schizophrenia. During the conference we will elaborate our findings with applied machine learning techniques which might shed more light on the predictive value of biomarkers for negative symptoms in schizophrenia.
DisclosureNo significant relationships.

Stress reactivity as a putative mechanism linking childhood trauma with clinical outcomes in individuals at ultra-high-risk for psychosis: Findings from the EU-GEI High Risk Study
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 30 / 2021
- Published online by Cambridge University Press:
- 28 May 2021, e40
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Changes in peripheral blood compounds following psychopharmacological treatment in drug-naïve first-episode patients with either schizophrenia or major depressive disorder: a meta-analysis
-
- Journal:
- Psychological Medicine / Volume 51 / Issue 4 / March 2021
- Published online by Cambridge University Press:
- 03 March 2021, pp. 538-549
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Imagery rescripting and eye movement desensitisation and reprocessing as treatment for adults with post-traumatic stress disorder from childhood trauma: randomised clinical trial
-
- Journal:
- The British Journal of Psychiatry / Volume 217 / Issue 5 / November 2020
- Published online by Cambridge University Press:
- 07 September 2020, pp. 609-615
- Print publication:
- November 2020
-
- Article
-
- You have access
- HTML
- Export citation
Verbal fluency as a possible predictor for psychosis
-
- Journal:
- European Psychiatry / Volume 25 / Issue 2 / March 2010
- Published online by Cambridge University Press:
- 16 April 2020, pp. 105-110
-
- Article
- Export citation
Priorities and satisfaction on the help needed and provided in a first episode of psychosis. A survey in five European Family Associations☆
-
- Journal:
- European Psychiatry / Volume 17 / Issue 8 / December 2002
- Published online by Cambridge University Press:
- 16 April 2020, pp. 425-433
-
- Article
- Export citation
Duration of untreated psychosis and the long-term course of schizophrenia
-
- Journal:
- European Psychiatry / Volume 15 / Issue 4 / June 2000
- Published online by Cambridge University Press:
- 16 April 2020, pp. 264-267
-
- Article
- Export citation
Preferences for treatment during a first psychotic episode
-
- Journal:
- European Psychiatry / Volume 16 / Issue 2 / March 2001
- Published online by Cambridge University Press:
- 16 April 2020, pp. 83-89
-
- Article
- Export citation
Opinions of mothers on the first psychotic episode and the start of treatment of their child
-
- Journal:
- European Psychiatry / Volume 19 / Issue 4 / June 2004
- Published online by Cambridge University Press:
- 16 April 2020, pp. 226-229
-
- Article
- Export citation
Long-term Outcome in Schizophrenia: a Six-year Follow-up in over 1000 Patients
-
- Journal:
- European Psychiatry / Volume 30 / Issue S1 / March 2015
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
1595 – The Effects Of Mixing Alcohol With Caffeinated Beverages On Subjective Intoxication
-
- Journal:
- European Psychiatry / Volume 28 / Issue S1 / 2013
- Published online by Cambridge University Press:
- 15 April 2020, 28-E881
-
- Article
-
- You have access
- Export citation
Interventions to improve adherence to antipsychotic medication in patients with schizophrenia–A review of the past decade
-
- Journal:
- European Psychiatry / Volume 27 / Issue 1 / January 2012
- Published online by Cambridge University Press:
- 15 April 2020, pp. 9-18
-
- Article
- Export citation
EPA-0767 – Plasma Oxytocin and Testosterone Levels in Patients with Psychotic Disorder, Their Unaffected Siblings and Healthy Controls: Results from the EU-GEI Project
-
- Journal:
- European Psychiatry / Volume 29 / Issue S1 / 2014
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
Transdiagnostic Exploration of the Association of Toxoplasma Gondii with Psychiatric Disorders. a Systematic Review and Meta Analysis
-
- Journal:
- European Psychiatry / Volume 30 / Issue S1 / March 2015
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
Association of treatment delay, migration and urbanicity in psychosis
-
- Journal:
- European Psychiatry / Volume 27 / Issue 7 / October 2012
- Published online by Cambridge University Press:
- 15 April 2020, pp. 500-505
-
- Article
- Export citation
