
145 results
The Crusades, the Latin East and Medieval History-Writing: An Introduction
-
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp 1-33
-
- Chapter
- Export citation
List of Illustrations
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp vii-vii
-
- Chapter
- Export citation
Notes on Contributors
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp ix-xii
-
- Chapter
- Export citation
Frontmatter
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp i-iv
-
- Chapter
- Export citation

Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
-
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024
List of Abbreviations
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp xiii-xiv
-
- Chapter
- Export citation
Acknowledgements
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp viii-viii
-
- Chapter
- Export citation
Index
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp 289-298
-
- Chapter
- Export citation
Contents
-
- Book:
- Crusade, Settlement and Historical Writing in the Latin East and Latin West, c. 1100-c. 1300
- Published by:
- Boydell & Brewer
- Published online:
- 22 February 2024
- Print publication:
- 02 January 2024, pp v-vi
-
- Chapter
- Export citation
Iodine intakes in school age girls aged 5–18 years in Ireland
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE4 / 2023
- Published online by Cambridge University Press:
- 05 September 2023, E272
-
- Article
-
- You have access
- HTML
- Export citation
Pharmacovigilance analysis of the Vigibase on antidepressants-related withdrawal syndrome in adults and adolescents
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S95-S96
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Antidepressant discontinuation may cause withdrawal syndrome in some cases. However, evidence on this syndrome related to individual antidepressants is limited, as well as about individual risk factors for severe reactions.
ObjectivesTo ascertain whether each individual antidepressant is associated with an increased reporting of withdrawal syndrome as compared with other medications, and to examine clinical risk factors for severe reactions.
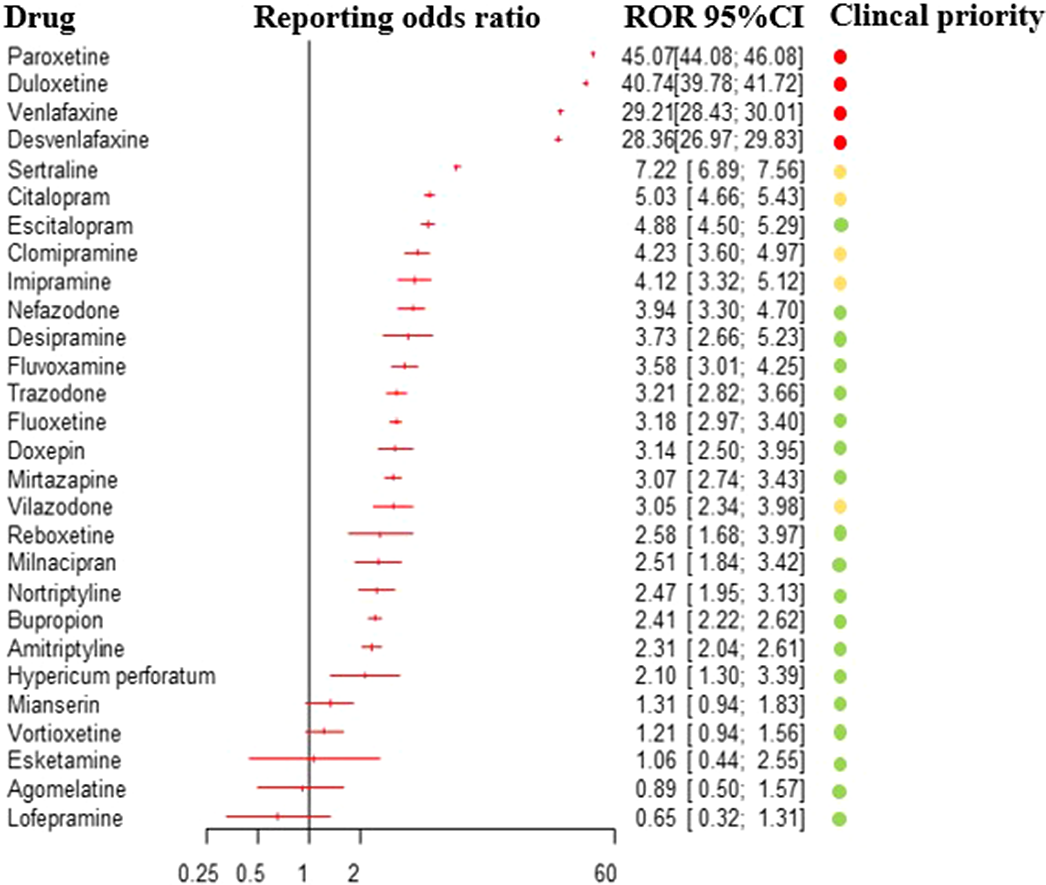
MethodsWe conducted a pharmacovigilance study, with a case/non-case design. We included reports of antidepressant-related withdrawal syndrome from the VigiBase, the WHO global database of individual case safety reports of suspected adverse drug reactions. We performed a disproportionality analysis (calculating reporting odds ratio (ROR) and the Bayesian information component (IC)) of reports of antidepressant-related withdrawal syndrome, comparing antidepressants to all other drugs and to buprenorphine (as a positive control). Antidepressants with significant disproportionate reporting were ranked in terms of clinical priority. We compared serious versus non-serious reactions to determine clinical risk factors for severe reactions.
ResultsBased on 31,688 reports of antidepressant-related withdrawal syndrome, we detected a disproportionate reporting for 23 antidepressants. The ROR for antidepressants altogether, compared to all other drugs, was 14.26 (95%CI:14.08-14.45), 17.01 for other antidepressants (95%CI:16.73-17.29), 13.65 for SSRIs (95%CI:13.41-13.90) and 2.8 for tricyclics (95%CI:2.59-3.02). Based on clinical priority ranking, the strongest signals were found for paroxetine, duloxetine, venlafaxine and desvenlafaxine (figure 1), being comparable to buprenorphine. Severe reactions were more frequently reported in males, adolescents, persons with multiple medications, and with longer treatment duration.
Image:
 Conclusions
ConclusionsAntidepressants are associated with increased reporting of withdrawal syndrome compared with other medications, with differences between individual antidepressants. Clinicians should be aware of such differences, when prescribing and discontinuing these drugs, as well as of the risk to experience more severe withdrawal symptoms in specific cases.
Disclosure of InterestC. Gastaldon: None Declared, G. Schoretsanitis Consultant of: Dr. Schoretsanitis has served as a consultant for HLS Therapeutics, E. Arzenton : None Declared, E. Raschi : None Declared, D. Papola: None Declared, G. Ostuzzi: None Declared, U. Moretti: None Declared, E. Seifritz Grant / Research support from: Dr. Seifritz has received educational grants, consulting fees and lecture honoraria from Janssen Cilag, Lundbeck, Angelini, Otsuka, Servier, Ricordati, Vifor, Sunovion, Schwabe and Mepha, Consultant of: Dr. Seifritz has received educational grants, consulting fees and lecture honoraria from Janssen Cilag, Lundbeck, Angelini, Otsuka, Servier, Ricordati, Vifor, Sunovion, Schwabe and Mepha, J. Kane Shareolder of: LB Pharmaceuticals and Vanguard Research Group, Consultant of: Dr. Kane has been a consultant and/or advisor for or has received honoraria from Alkermes, Allergan, LB Pharmaceuticals, H. Lundbeck, Intracellular Therapies, Janssen Pharmaceuticals, Johnson and Johnson, Merck, Minerva, Neurocrine, Newron, Otsuka, Pierre Fabre, Reviva, Roche, Sumitomo Dainippon, Sunovion, Takeda, Teva and UpToDate, G. Trifirò Grant / Research support from: he was the scientific director of a Master program on pharmacovigilance, pharmacoepidemiology and real-world evidence which has received non-conditional grant from various pharmaceutical companies; he coordinated a pharmacoepidemiology team at the University of Messina until Oct 2020, which has received funding for conducting observational studies from various pharmaceutical companies (Boehringer Ingelheim, Daichii Sankyo, PTC Pharmaceuticals). He is also scientific coordinator of the academic spin-off “INSPIRE srl” which has received funding for conducting observational studies from contract research organizations (RTI Health Solutions, Pharmo Institute N.V.)., Consultant of: Dr. Trifirò has served in the last three years on advisory boards/seminars funded by SANOFI, Eli Lilly, AstraZeneca, Abbvie, Servier, Mylan, Gilead, Amgen;, Speakers bureau of: Dr. Trifirò has served in the last three years on advisory boards/seminars funded by SANOFI, Eli Lilly, AstraZeneca, Abbvie, Servier, Mylan, Gilead, Amgen;, C. Barbui: None Declared

7 - Attention, Affect, and Creativity, from Mindfulness to Mind-Wandering
- from Part II - The Development of Creativity
-
-
- Book:
- The Cambridge Handbook of Creativity and Emotions
- Published online:
- 16 February 2023
- Print publication:
- 23 February 2023, pp 130-148
-
- Chapter
- Export citation
Do Clinicians Need to Rethink Antipsychotic Maintenance Treatment?: Pro
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S6
-
- Article
-
- You have access
- Open access
- Export citation
Co-occurrence of clozapine-related DRESS syndrome core clinical manifestations: results of a systematic review
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S719
-
- Article
-
- You have access
- Open access
- Export citation
Laboratory-Based 3D X-ray Imaging of Neutron-Irradiated Ceramic Particle Nuclear Fuel
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2038-2039
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Understanding Fission Gas Bubble Distribution and Zirconium Redistribution in Neutron-irradiated U-Zr Metallic Fuel Using Machine Learning
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 82-83
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Advanced Crack Analytics on 3D X-ray Tomography of Irradiated Silicon Carbide Claddings
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 208-210
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Implementation of personalised medicine policies in mental healthcare: results from a stated preference study in the UK
-
- Journal:
- BJPsych Open / Volume 8 / Issue 2 / March 2022
- Published online by Cambridge University Press:
- 03 February 2022, e40
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Contraception Deserts: The Effects of Title X Rule Changes on Access to Reproductive Health Care Resources
-
- Journal:
- Politics & Gender / Volume 18 / Issue 3 / September 2022
- Published online by Cambridge University Press:
- 03 February 2022, pp. 672-707
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Iodine intakes in Irish children aged 5–12 years
-
- Journal:
- Proceedings of the Nutrition Society / Volume 80 / Issue OCE3 / 2021
- Published online by Cambridge University Press:
- 17 August 2021, E123
-
- Article
-
- You have access
- HTML
- Export citation
