
329 results
Association of Early Tracheostomy with Length of Stay and Mortality in Critically Ill Patients
-
- Journal:
- The Journal of Laryngology & Otology / Accepted manuscript
- Published online by Cambridge University Press:
- 22 April 2024, pp. 1-22
-
- Article
- Export citation
391 Value estimation of the Diabetes Prevention Program: How well does clinical trial-based cost-effectiveness apply to the real world?
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 116
-
- Article
-
- You have access
- Open access
- Export citation
Emotions and behaviours of child and adolescent psychiatric patients during the COVID-19 pandemic
-
- Journal:
- BJPsych Open / Volume 10 / Issue 2 / March 2024
- Published online by Cambridge University Press:
- 16 February 2024, e47
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring symptom clusters in mild cognitive impairment and dementia with the NIH Toolbox
-
- Journal:
- Journal of the International Neuropsychological Society , First View
- Published online by Cambridge University Press:
- 16 February 2024, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
61 Network Segregation Predicts Processing Speed in the Cognitively Healthy Oldest-old
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 367-368
-
- Article
-
- You have access
- Export citation
Impact of intensified prevention measures on the rate of hospital-acquired bloodstream infections among mechanically ventilated COVID-19 patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 14 December 2023, e235
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies used for the COVID-OUT decentralized trial of outpatient treatment of SARS-CoV-2
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 07 November 2023, e242
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Integrated safety analysis of phase 3 studies for investigational microbiome therapeutic, SER-109, in recurrent CDI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s44-s45
-
- Article
-
- You have access
- Open access
- Export citation
Contribution of active surveillance cultures to the control of hospital-acquired carbapenem-resistant Acinetobacter baumannii in an endemic hospital setting
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 20 September 2023, pp. 188-195
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Understanding Shield Laws
-
- Journal:
- Journal of Law, Medicine & Ethics / Volume 51 / Issue 3 / Fall 2023
- Published online by Cambridge University Press:
- 13 December 2023, pp. 584-591
- Print publication:
- Fall 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Advocacy at the Eighth World Congress of Pediatric Cardiology and Cardiac Surgery
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 24 August 2023, pp. 1277-1287
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cardiac magnetic resonance predictors for successful primary biventricular repair of unbalanced complete common atrioventricular canal
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 18 July 2023, pp. 387-394
-
- Article
- Export citation
Chapter 20 - Anesthesia for Endocrine Diseases
-
-
- Book:
- Cambridge Handbook of Anesthesiology
- Published online:
- 24 May 2023
- Print publication:
- 08 June 2023, pp 314-337
-
- Chapter
- Export citation
68 Metformin prevents the diagnosis of Long Covid in phase 3 trial of early treatment.
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, pp. 18-19
-
- Article
-
- You have access
- Open access
- Export citation
Processing of social and monetary rewards in autism spectrum disorders
-
- Journal:
- The British Journal of Psychiatry / Volume 222 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 26 January 2023, pp. 100-111
- Print publication:
- March 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Validity of the NIH toolbox cognitive battery in a healthy oldest-old 85+ sample
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue 6 / July 2023
- Published online by Cambridge University Press:
- 14 October 2022, pp. 605-614
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy and moderators of cognitive therapy versus behavioural activation for adults with depression: study protocol of a systematic review and meta-analysis of individual participant data
-
- Journal:
- BJPsych Open / Volume 8 / Issue 5 / September 2022
- Published online by Cambridge University Press:
- 10 August 2022, e154
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
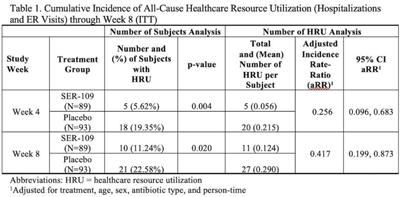
Healthcare resource utilization in a phase 3 trial of SER-109 in patients with recurrent Clostridioides difficile infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s73
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The estimated economic cost of Clostridioides difficile infection (CDI) is $5.4 billion annually, primarily attributed to acute-care costs. We previously reported data from ECOSPOR III that SER-109, an investigational oral microbiome therapeutic, was superior to placebo in reducing recurrent CDI (rCDI) in adults at 8 weeks after treatment, with a 68% relative risk reduction. Adults with rCDI have more hospitalizations and emergency room (ER) visits (defined herein as healthcare resource utilization, HRU) compared to those without recurrence. Thus, we evaluated incidence of HRU. Methods: Adults with rCDI (≥3 episodes in 12 months) were screened at 56 US and Canadian sites and were randomized 1:1 to SER-109 (4 capsules × 3 days) or placebo following resolution of CDI with standard-of-care CDI antibiotics. The primary end point was rCDI at 8 weeks. Exploratory end points included cumulative incidence of hospitalizations through 24 weeks after treatment. Here, we report cumulative incidence of all-cause HRU through 8 weeks after treatment. Results: In total, 281 patients were screened and 182 were randomized (59.9% female; mean age 65.5 years; 98.9% outpatient). Overall, 31 patients (17%) had 38 hospitalizations or ER visits through week 8 (11 events in 10 SER-109 patients and 27 events in 21 placebo patients) (Table 1). The cumulative incidence of HRU was lower in SER-109–treated patients compared to placebo at both weeks 4 and 8 with most events (65.8%) recorded within 4 weeks after treatment. The adjusted HRU incidence rate (by person time, age, sex, and antibiotic use) was also lower in SER-109–treated patients compared to placebo at weeks 4 and 8 (0.256 [95% CI, 0.096–0.683] versus 0.417 [95% CI, 0.199–0.873], respectively). Conclusions: SER-109–treated patients had less HRU compared to placebo patients through 8 weeks after treatment in this mostly outpatient population. These data suggest a potential benefit of SER-109 in reducing HRU, thus lowering the healthcare burden of rCDI.
Funding: Seres Therapeutics
Disclosures: None

Autism and autistic traits in those who died by suicide in England
-
- Journal:
- The British Journal of Psychiatry / Volume 221 / Issue 5 / November 2022
- Published online by Cambridge University Press:
- 15 February 2022, pp. 683-691
- Print publication:
- November 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Risk factors for Veteran food insecurity: findings from a National US Department of Veterans Affairs Food Insecurity Screener
-
- Journal:
- Public Health Nutrition / Volume 25 / Issue 4 / April 2022
- Published online by Cambridge University Press:
- 08 November 2021, pp. 819-828
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
