



Adolescence is the most appropriate time to develop positive health behaviours that can continue throughout life. At the same time, it is the most vulnerable period in terms of development of diseases that can be seen in adulthood(Reference Akman, Tuzun and Unalan1,Reference Carrara and Schulz2) .
Adolescents encounter many factors that threaten their health during their growth and development stages. One of these factors, malnutrition, adversely affects both the physical and mental development of adolescents(Reference Carrara and Schulz2,3) . The main nutritional problems of adolescents living in developing countries are malnutrition, obesity and other chronic diseases, and inadequate/unhealthy eating habits and lifestyle(Reference Aksoydan and Cakır4–Reference Sarkar, Manna and Sinha6). Amongst the most common problems associated with malnutrition in adolescents in Turkey are thinness, obesity, malnutrition, avitaminosis, dental caries, simple goitre and anaemia. Additionally, inadequate and unbalanced nutrition is reported to reduce adolescents’ perception and attention spans, to increase learning disabilities, behavioural disorders and school absenteeism and to cause a decrease in school achievement(Reference Kulturoglu, Mentesoglu and Memis7).
According to the Global Nutrition Report, while school-age children, adolescents and adults consume excessive refined grains and sugar-added foods and beverages, they do not consume health-improving foods such as fruits, vegetables, legumes and whole grains. About a third of school-age children (30·3 %) do not eat fruit daily; nevertheless, 43·7 % consume carbonated beverages daily(Reference Fanzo, Hawkes and Udomkesmalee8). In adolescence, excess weight and obesity resulting from an unhealthy diet and inadequate physical activity, and non-communicable diseases including diabetes, hypertension, CHD, stroke, some cancers and obstructive sleep apnoea pose a risk for future health(3). Anaemia has been reported to be a persistent problem in women aged between 15 and 49 years with a prevalence of 32·8 %. Thinness among adolescent females increased from 5·5 % in 2000 to 5·7 % in 2016. Data from 200 countries show that obesity rates have been increasing annually in both male and female adolescents (10–19-year-olds) and that it reached 6·5 and 4·7 %, respectively, in 2016(Reference Fanzo, Hawkes and Udomkesmalee8). Also, a meta-analysis study on the prevalence of obesity in children and young adults in Turkey reports that the prevalence of obesity increased from 0·6 to 7·3 % by 11·6 times increase between 1990–1995 and 2011–2015. In the same study, the prevalence was reported to increase in both genders; however, boys are more likely to be obese than girls(Reference Alper, Ercan and Uncu9).
The diet quality of children and adolescents has deteriorated worldwide in recent years. Current dietary data show that young people do not comply with dietary recommendations, especially regarding fruit and vegetable consumption. Also, the consumption of processed food, oil and sugar-added drinks has increased(Reference Tallon, Dias and Costa10). Adolescents are increasingly exposed to unhealthy food environments and marketing of unhealthy foods (on television (TV), movies, social media and point-of-sale advertisements). They consume larger amounts of inexpensive, energy-dense, nutrient-poor foods that are rich in sugar, Na and fat (including processed and ultra-processed foods). They do not have access to affordable fresh fruits and vegetables, and they may not have control of resources, nutritional knowledge or skills to purchase and prepare foods necessary for a healthy diet(3).
To prevent nutritional problems or develop healthy eating behaviours, first of all, it is necessary to determine the food habits (FH) and amend the negative behaviours. For a healthy diet, the adolescent needs to consume basic nutrients in a sufficient and balanced way and make this a habit(Reference Brooks and Begley11). Promoting nutrition literacy (NL) is usually highlighted in prevention programmes for basic nutritional problems(Reference Brooks and Begley11,Reference Thomas and Irwin12) . Many factors, such as the effective role of nutrition in a healthy life, an increased diversity in nutrients and an increase in out-of-home nutrient consumption, have made NL an important issue(Reference Keser, Cıracıoglu, Yıldırım and Keser13). Training programmes intending to develop skills to achieve and use the right foods are considered as part of NL(Reference Kimura14). NL is the degree to which individuals gain nutritional skills and read and understand the nutritional information necessary to make appropriate nutritional decisions(Reference Demir Ozdenk and Ozcebe15–Reference Velardo18). To reduce the increasing prevalence of nutritional health problems, it is of great importance to increase the knowledge level of individuals and society about nutrition and to develop healthy nutrition skills and behaviours(Reference Gibbs and Chapman-Novakofski19). Evidence is needed to draw attention to the NL level of adolescents and to promote nutritional education and quality. National studies on NL are limited compared with the existing international ones. For this reason, the current study aimed to investigate the relationship between NL and the FH of adolescents studying at high schools in the west of Turkey and the factors affecting them. Accordingly, the study sought answers to the following research questions.
Research questions
RQ1. What are the NL and FH levels of adolescents?
RQ2. Is there a relationship between mean Adolescent Nutrition Literacy Scale (ANLS) and the Adolescent Food Habit Checklist (AFHC) total scores?
RQ3. Is there a relationship between some characteristics of adolescents and the mean ANLS total score?
RQ4. Is there a relationship between some characteristics of adolescents and the mean AFHC total score?
Methods
Design and participants
The study used a cross-sectional design and was conducted from September 2018 to February 2019. The universe of the study consisted of a total of 1500 adolescents studying in three high schools located in the west of Turkey. The study sample was calculated as 306 using the known population sampling formula (N = N·t 2·p·q/d 2(N – 1) + t 2·p·q), assuming that the standard deviation would be 5 % and the probability of occurrence would be 50 % because the probability of occurrence of the case that was investigated in light of the relevant literature could not be reached. As there might be losses in the sample during the study process, we planned to include 367 adolescents in the study, which was 20 % more than the number of subjects already calculated(Reference Sümbüloğlu and Sümbüloğlu20). A total of 467 adolescents were included in the study. A total of 467 adolescents, except for those who had school absenteeism, who did not deliver a written parental consent or who were not willing, participated in the study.
Measurement tools
The socio-demographic characteristics information form
Designed by the researchers, this form consists of questions for the collection of information about adolescents, including age, grade, gender, height, weight, BMI, family type, education level of parents, family income level, sports activity, daily sleep time, study time outside school, daily time spent using a computer and watching TV, frequency and consumption of fast food (hamburger, pizza, chips, cake, biscuit, cracker, chocolate, cookies, ice cream, etc.), number of meals, skipping meals and snacks.
Adolescent nutrition literacy scale
This scale was developed by Bari(Reference Bari21) to determine the NL level of adolescents. The Turkish validity and reliability study of the scale was conducted by Sonay Turkmen et al. (Reference Sonay Turkmen, Kalkan and Filiz17). It is a five-point Likert-type scale, which consists of twenty-two items and three sub-dimensions. The minimum and maximum scores that can be obtained from the scale are 22 and 110, respectively. The three sub-dimensions are as follows:
Functional Nutrition Literacy (FNL): This sub-dimension determines the status of adolescents to follow national and international sources of information on nutritional issues. The minimum and maximum scores that can be obtained from this sub-dimension are 7 and 35, respectively.
Interactive Nutrition Literacy (INL): This sub-dimension identifies the extent to which adolescents modify their nutritional habits through the information they have obtained. The minimum and maximum scores that can be obtained from this sub-dimension are 6 and 30, respectively.
Critical Nutrition Literacy (CNL): This sub-dimension identifies whether adolescents play an active role in nutritional issues. The minimum and maximum scores from this sub-dimension vary from 9 to 45.
Cronbach’s α value for the total scale score is 0·80, and it ranges from 0·66 to 0·84 for the sub-dimensions. An increase in the score of adolescents shows an increase in the level of NL.
Adolescent food habit checklist
The scale developed by Johnson et al. (Reference Johnson, Wardle and Griffith22) to measure healthy eating behaviours in adolescents consists of twenty-three items, and each correct answer for healthy eating is assigned 1 point (Cronbach’s α 0·83, test−retest r 0·90, P < 0·001). The Turkish adapted version of the scale by Arikan et al. (Reference Arikan, Aksu and Metintas23) consists of nineteen items (Cronbach’s α 0·72). The highest score that can be obtained from the scale is 19. Increased scores obtained from the scale show that adolescents have healthy eating behaviours(Reference Arikan, Aksu and Metintas23).
Data collection
After the ethics committee and institution approval processes were completed, the researchers made a one-to-one visit to all classes in three schools and informed the adolescents about the study. Volunteer students took the parental consent forms to their parents. After the parents read and signed the informed written consent, they sent this form back to the researchers. After the researchers received the signed informed consent forms from the parents, the questionnaires were distributed to the adolescents in the classroom environment without disturbing the course of the ongoing lessons, and then the completed forms were collected. The researchers took the height and weight measurements of the students. While taking the measurements, students removed extra clothing and their shoes to obtain more accurate data. For getting weight measurements, a conventional scale was used; an inelastic tape measure was used to obtain height measurements. All measurements were taken with participants standing in an upright position. To find the BMI value, the following equation was used: BMI = weight (kg)/height (m2), and the WHO standards were used for BMI classifications(24). Application of the data collection tools took approximately 20 min for each student.
Statistical methods
The IBM SPSS Statistics 22.0 (IBM) software was used for the statistical analysis. Socio-demographic characteristics were analysed with descriptive statistics (numbers, percentages, mean and standard deviationsd values). The fit of the variables to normal distribution was evaluated using skewness and kurtosis values and the Shapiro−Wilk test. The Student’s t test, Mann–Whitney U test and one-way ANOVA were employed for the comparison between adolescents’ descriptive characteristics and their mean scores from the ANLS and AFHC. Multiple comparisons of these variables used Tukey’s honestly significant difference, least significant difference, Hochberg’s GT2 and Gabriel tests when the variances were equal and Tamhane’s T2 test if not equal. The relationship between ANLS and AFHCC scores was analysed using correlation analysis, while linear regression analysis was employed to predict the change in the NL of adolescents at the level of FH. Significance level was accepted as P < 0·05.
Results
The mean age, height, weight and BMI of the adolescents were 15·54 (sd 1·13) years, 1·68 (sd 0·08) m, 61·97 (sd 13·53) kg and 21·65 (sd 3·94) kg/m2, respectively. Of the total participants, 56·5 % were female. As for BMI classifications, 21·4 % of the participants were underweight, 62·1 % were normal weight and 16·5 % were overweight. Also, 50 % were ninth graders, 89·5 % had a nuclear family, 43·9 and 37·5 % of the mothers and fathers were elementary school graduates, respectively, and the family income of 65·5 % was found to be equal to the expenses.
When daily lifestyle behaviours were examined, 54 % were found to not do any sports activities, 62·3 % slept 7–12 h daily, 74·9 % studied 1–3 h outside of school, 28·7 % watched TV for >1 h a day, 31·9 % spent >1 h using a computer, 88·2 % consumed fast food, 21·8 % consumed fast food more than three times a day, 22·5 % consumed four or more meals a day, 51·4 % skipped meals during the day, 31·3 % usually skipped breakfast and 70·9 % usually consumed fast food as a snack (Table 1).
Table 1 Daily life style behaviours of adolescents (n 467)

The mean scores of the adolescents were 72·28 (sd 9·53) for ANLS; 25·63 (sd 4·98), 17·59 (sd 5·29), 29·04 (sd 4·42) for FNL, INL and CNL sub-dimensions, respectively; and 9·77 (sd 3·31) for FH. The examination of the socio-demographic characteristics of adolescents indicated that ANLS and INL scores were significantly higher in females. Adolescents with low BMI values were found to have significantly higher CNL scores than healthy and overweight subjects. ANLS and FNL scores of eleventh graders were significantly higher compared with those of the ninth graders, and the scores of those whose fathers were university graduates were found to be significantly higher than those of the students whose fathers were elementary or high school graduates (P < 0·05). No statistically significant difference was found between the scores from ANLS and its sub-dimensions and the factors of family type, education level of the mother and family income, nor was there any statistically significant difference between AFHC and socio-demographic characteristics of adolescents (P > 0·05) (Table 2).
Table 2 Socio-demographic factors affecting nutrition literacy and food habits of adolescents (n 467)*

ANLS, Adolescent Nutrition Literacy Scale; FNL, Functional Nutrition Literacy; INL, Interactive Nutrition Literacy; CNL, Critical Nutrition Literacy; AFHC, Adolescent Food Habit Checklist; t, Student’s t test; U, Mann–Whitney U.
Statistically significant values are given in bold.
* P value > 0·05 was considered to show a statistically significant result.
F, one-way ANOVA (when an overall significance was observed, pairwise post hoc tests were performed using †Hochberg’s GT2 and ‡Tukey).
When the daily lifestyles of adolescents were examined, ANLS, INL and CNL scores were found to be significantly lower in students engaging in any sports activities, while FNL scores were significantly lower in those who skipped meals during the day (P < 0·05). ANLS, FNL and INL scores of those who watched TV <1 h/d were found to be significantly higher than those of the students who spent more time watching TV. ANLS and FNL scores of adolescents who consumed fewer than three fast-food items a day were significantly higher than those who consumed more than three fast-food items a day (P < 0·05). ANLS and FNL scores of adolescents who skipped dinners were lower than those who did not skip any meals and those who skipped lunch. Also, the INL score of those who skipped dinner was significantly lower than those who skipped lunch (P < 0·05). There was no statistically significant difference between ANLS and sub-dimension scores of adolescents and their fast-food consumption, daily sleep time, study time outside school, daily time spent using computers and daily meal counts (P > 0·05). The AFHC score was found to be significantly lower in adolescents who did not do any sports, who consumed fast food and who skipped meals within the day (P < 0·05). However, this score was significantly higher in adolescents who slept 7–12 h/d compared with those who slept <6 h/d (P < 0·05). The AFHC score of adolescents who studied 4–6 h outside school times was significantly higher than both those who did not study at all and those who spent 1–3 h/d studying lessons (P < 0·05), while the AFHC score of students who spent 1–3 h/d studying was significantly higher than those of the students who did not study at all (P < 0·05). Also, the AFHC score of adolescents who consumed more than three fast-food items a day was found to be significantly lower than those of the adolescents who consumed less or no fast food at all. Also, the AFHC score of adolescents who did not consume fast food was significantly higher than those who consumed fewer than three fast-food items (P < 0·05). Moreover, the AFHC score of adolescents who consumed fewer than three fast-food items a day was found to be significantly higher compared with those consuming fewer than three (P < 0·05). The AFHC score of adolescents skipping dinner was found to be significantly lower than those who did not skip dinner and those who skipped breakfast (P < 0·05; Table 3).
Table 3 Daily life style behaviours affecting nutrition literacy and food habits of adolescents (n 467)*
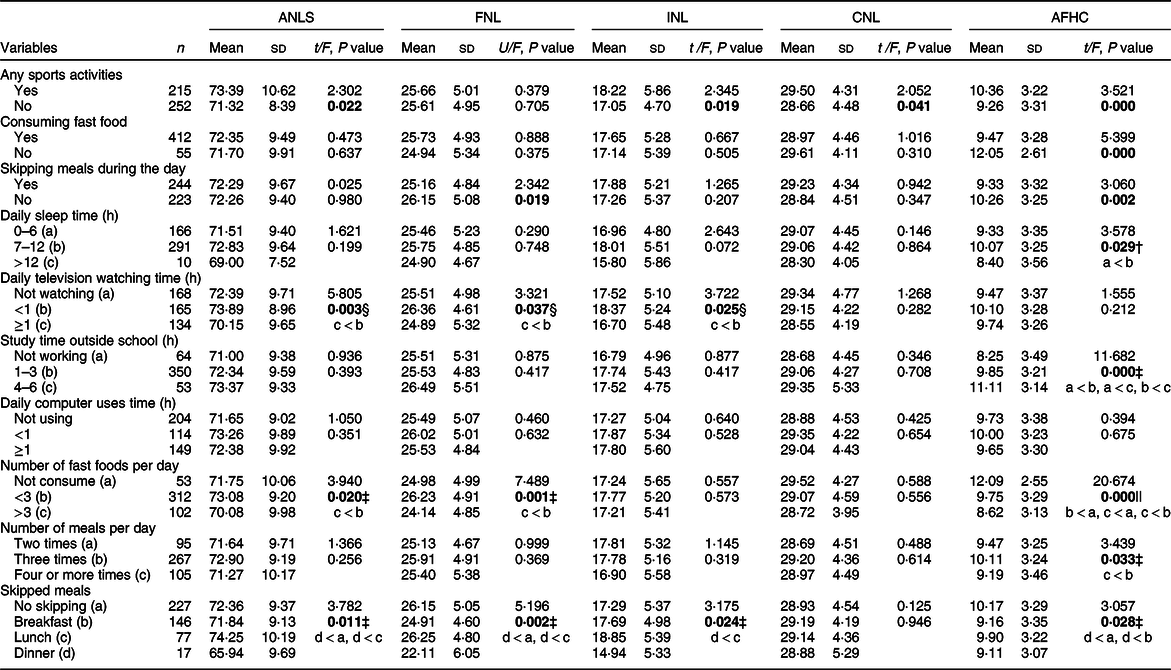
ANLS, Adolescent Nutrition Literacy Scale; FNL, Functional Nutrition Literacy; INL, Interactive Nutrition Literacy; CNL, Critical Nutrition Literacy; AFHC, Adolescent Food Habit Checklist; t, Student’s t test; U, Mann–Whitney U.
Statistically significant values are given in bold.
* P value > 0·05 was considered to show a statistically significant result.
F, one-way ANOVA (when an overall significance was observed, pairwise post hoc tests were performed using †LSD, ‡Hochberg’s GT2, §Gabriel and ||Tamhane’s T2).
There was a positive and significant relationship between adolescents’ AFHC and ANLS scores (Pearson’s correlation r 0·357; P = 0·000), and amongst FNL scores (Spearman’s Rho r 0·133; P = 0·004), INL scores (Pearson’s correlation r 0·341; P = 0·000) and CNL scores (Pearson’s correlation r 0·216; P = 0·000). As ANLS scores increased, AFHC scores were found to increase as well (significant at 0·01).
In linear regression analysis, four models were established according to the relationship between variables. When the significance level corresponding to the F-value for the model was analysed, the established model was found to be statistically significant. Each of the subscales in the ANLS was specified as a separate model. On the other hand, in the last model, the effect of the total score of the ANLS on nutritional habits was determined. The NL status increases as the total score obtained from the ANLS increases. In the first model, the functional nutrition subscale of the NL scale was found to affect 1·7 % of the nutritional habits of adolescents, while the increase in functional NL was determined to increase nutritional habits 0·129 (β = 0·129) times. In the second model, while the interactive nutrition subscale of the NL scale was observed to impact 11·7 % of adolescents’ nutritional habits, the increase in interactive NL was found to increase nutritional habits 0·341 (β = 0·341) times. In the third model, while the critical nutrition subscale of the NL scale was determined to influence 4·7 % of adolescents’ nutritional habits, the increase in critical NL increased nutritional habits 0·216 (β = 0·216) times. In the fourth model, the NL scale with its functional, interactive and critical nutrition subscales was determined to impact 12·8 % of adolescents’ nutritional habits, and the increase in NL increased nutritional habits by 0·357 (β = 0·357). All factors were found to have a statistically significant effect on the nutritional habits of adolescents (P < 0·05; Table 4).
Table 4 The effect of nutrition literacy of adolescents on their food habits (n 467)

ANLS, Adolescent Nutrition Literacy Scale; F, ANOVA value; R, correlation coefficient; DW, Durbin–Watson.
* Dependent variable.
† Standardised β.
‡ Significant at P < 0·05.
Discussion
Nutritional health problems have increased in recent years and have become a significant public health problem. The relationship between NL and the FH of adolescents studying in high schools in a city in the west of Turkey was discussed in line with the literature in the current study. In the current study, a statistically significant relationship was found between adolescents’ gender, father education, class, BMI values, daily lifestyle behaviours variables and NL. Increased NL levels of adolescents were found to have a positive effect on their FH.
Various individual and environmental factors affect food choices and eating behaviours during adolescence. Amongst the individual characteristics, adolescents’ level of knowledge about nutrition holds an important place(Reference Kabaran and Mercanligil25). NL is the capacity to acquire and understand nutritional information, as well as having the necessary skills to make the right decisions for suitable nutrition(Reference Sonay Turkmen, Kalkan and Filiz17,Reference Bari21) . Individuals with sufficient NL levels have basic nutritional knowledge and can understand enough information about food items and food groups to read the food label and to control portions(Reference Demir Ozdenk and Ozcebe15). In the current study, NL was found to be at a good level in adolescents. In other studies, NL was stated to be at the middle level in adolescents, and this result was reported to be below the expected level(Reference Bari21,Reference Ayer26) . Investigating NL status and its relationship with the amount and quality of dietary intake among young people can help improve nutritional health among this critical age group and adopt effective strategies(Reference Joulaei, Keshani and Kaveh27). In a study, it was reported that adolescents should know and follow the dietary guidelines for various reasons such as following a healthy lifestyle, making informed decisions or keeping fit and/or not getting fat. However, the majority of the adolescents were reported to not choose or prepare foods appropriately because they did not know how to apply the dietary guidelines. Also, they stated that they did not read the food labels because they believed that food labels were only for people with special dietary requirements, and they were not interested and/or were very hungry at the time of purchase or did not know what information they needed to look for. On the other hand, adolescents who read food labels were reported to be looking for information about sugar, carbohydrates, energies or kilojoules, portions, saturated fats and/or total fat(Reference Ronto, Lauren and Donna28).
Given the growth and development characteristics of adolescents, current technological advances, ease of access to information and the health promotion projects carried out in schools, NL can be expected to be at a good level in adolescents. Considering all these factors in our study, good levels of NL in adolescents are an expected result. The reason why this result is different from that of other studies may be due to regional or socio-cultural characteristics.
The food choices of adolescents are also influenced by gender. In the current study, NL and INL scores of the girls were found to be high. In a similar study, a difference was found between female and male adolescents in terms of NL and the score of female students was observed to be higher(Reference Bari21,Reference Guttersrud and Petterson29) . In another study, females were determined to give more importance to eating healthy food or a healthy diet than males(Reference Lee, Liao and Lai5). In the study in which Joulaei et al. (Reference Joulaei, Keshani and Kaveh27) examined the effect of adolescents’ NL on their diet, more than half of the adolescents were reported to seek information about diet or food and that their sources mostly included the Internet, family and books. An increase in NL, INL and CNL scores was shown to improve dietary quality in males. According to another study, there was a strong consensus among girls about consuming healthy foods and they obtained nutritional and health information from many sources, including teachers, family members and indirectly from the media(Reference Lee, Liao and Lai5). Another study revealed that knowledge alone was not enough to change individual behaviours such as dietary choices(Reference Vaitkeviciute, Ball and Harris30). Similarly, according to the study of Ronto et al. (Reference Ronto, Lauren and Donna28), the portion sizes of female adolescents were not important for healthy foods, compared with males, but were certainly important for unhealthy foods. ‘The source of a given food’ was reported to be rated as more important for healthy nutrition among females compared with males.
According to the results of our study, when the biopsychosocial development characteristics of adolescents are considered, the importance they attach to nutrition is thought to increase. Adolescents tried to reach various sources for appropriate nutrition, and this showed that they made positive changes in their diets as their NL increases.
BMI is the most useful and practical indicator of overweight and obesity at the social level and gives an indirect measurement of body fat(24). Today, the world faces an epidemic of obesity, and adolescents consume more energies from less nutritious foods(Reference Chung31). Increasing nutritional knowledge and skills through improved NL is an interdisciplinary approach to reducing BMI in children and a preventive measure to reduce overweight and obesity in adulthood(Reference D’Amato-Kubiet32).
In one study, no statistically significant relationship was found between BMI and NL(Reference Ayer26). In our study, adolescents with poor BMI values had higher CNL scores. With the change in physical appearance and the increase in cognitive abilities, adolescents often engage their minds by commenting on their bodies. If people do not perceive themselves as overweight or obese, they may not try to lose weight and may not think that obesity-related nutritional messages are directed towards them(Reference Cetinkaya, Tayhan and Ozmen33). According to the results of our study, adolescents with poor BMI values were careful about using the right nutrition sources, they were open to any advice about nutrition given by family and friends and they were more willing to pass on the information they learned about healthy food consumption to their relatives and to take part in healthy nutrition activities in school.
In parallel with the increase in the level of education, adolescents have become more conscious consumers and, thus, can make more effective food choice decisions(Reference Ayer26,Reference Incedal Sonkaya, Balci and Ayar34) . In this study, ANLS and FNL scores increased as class levels increased. However, this score was found to decrease in senior high school students. A positive relationship was found between NL level and education level in a study(Reference Patel, Panaich and Steinberg35). Similarly, the results of our study suggested that as the grade level of the adolescents increased, their ability to access and interpret nutritional information increased as well.
In our study, the ANLS and FNL scores of adolescents were found to increase as the education level of the father increased. Family FH have a significant effect on children’s FH and food choices(Reference Kabaran and Mercanligil25). Parents with a higher level of education are aware of the relationship between nutrition and health and, thus, prefer healthy and low energy-intensive foods for their child’s nutrition(Reference Galvan-Portillo, Sanchez and Cardenas-Cardenas36). Studies have shown that NL is an important factor explaining the differences in dietary habits. Studies also reported that there are healthier nutrition practices that are positively associated with higher NL skills(Reference Carbone and Zoellner37). In one study, a significant and positive relationship was observed between parental NL and child dietary quality and a 1 % increase in parental NL level was determined to increase the dietary quality of the child by 0·51 points(Reference Gibbs, Kennett and Kerling38). Another study reported that some adolescents consumed healthier foods while eating with their family, but that others had no control over food choices as they depended on parents’ choices, and they had to eat whatever was given to them by their parents although they knew the food was unhealthy(Reference Ronto, Lauren and Donna28).
In fact, parents’ food choices are the most important factors that determine the FH of adolescents(Reference Akman, Tuzun and Unalan1). In particular, fathers are usually a source of funding to buy snacks(Reference Lee, Liao and Lai5).
According to the results of the current study, the parent who can convert the right information about nutrition to health behaviours should be considered as a correct role model, especially for their children.
In adolescence, physical activity is known to be related to both physical and mental aspects of health. Research has shown that obesity is associated with unhealthy behaviours, such as inadequate physical activity and increased sedentary behaviour(Reference Farahani, Amiri and Chin39). Studies reported that there is a positive development in nutrition habits along with the increase in physical activity(Reference Keskin, Alpkaya and Cubuk40,Reference Yabanci and Pekcan41) . In our study, the majority of adolescents were found to not do any sport. The ANLS, INL, CNL and AFHC scores of the adolescents who engaged in any sports were higher and they showed healthy eating behaviours. As a result of our study, a positive development was observed in the healthy FH and NL of adolescents doing sports. In one study, physical activity level was stated to affect the level of individual NL(Reference Guttersrud and Petterson29). In another study, a significant relationship was found between physical activity and nutrition in adolescents(Reference Keskin, Alpkaya and Cubuk40).
In the current study, the FH of adolescents skipping meals were observed to be poor. Adolescents’ ability to access, understand and interpret nutritional information can be said to affect healthy eating behaviours, and as a result of this, they skip meals during the day. Three main meals should be consumed regularly for adequate and balanced nutrition. Skipping main meals, especially breakfast, will cause problems in the process of growth and development, as well as adversely affecting academic success. However, skipping meals is a common behaviour in adolescents(Reference Aksoydan and Cakır4).
A study reported that approximately 97 % of adolescents skipped breakfast twice a week and 82 % consumed junk food twice a week(Reference Joshi, Jethva and Patel42). In our study, adolescents were found to mostly skip breakfast. Similarly, in other studies, breakfast was shown to be the most often skipped meal(Reference Aksoydan and Cakır4,Reference Sonay Turkmen, Kalkan and Filiz17,Reference Akan43) . Students skipping breakfast in the morning may stem from reasons such as worrying about being late for school, not having an appetite for an early breakfast and having difficulty waking up in the morning. School settings can be an opportunity to improve food safety and dietary quality of adolescents. Schools can increase access to healthy foods and develop useful strategies to increase diet diversity and awareness of healthy diets(Reference Schreinemachers, Bhattarai and Subedi44).
Also, in our study, although the number of adolescents who skipped dinner was found to be less, they were found to have lower NL and FH. The reason for not skipping dinner may be due to cultural characteristics such as eating with the family. At the same time, adolescents may be said to have difficulty reaching, reading and understanding basic information about nutrition and changing their eating habits.
There is a significant relationship between the time spent watching TV and obesity in adolescents(Reference Akman, Tuzun and Unalan1,Reference Aksoydan and Cakır4,Reference Kabaran and Mercanligil25,Reference Prasanna Kamath, Bengalorkar and Deepthi45) . A 1 h increase in the time spent watching TV was reported to increase obesity prevalence by 2–6 %. With the time spent watching TV, the frequency of consuming snacks also increases. While watching TV, foods with low nutritional value are preferred and fruit, vegetable and milk consumption is reduced. Frequently consumed foods in front of the TV are pizza, hamburgers, chips, biscuits, cola drinks and juices(Reference Dennison and Edmunds46). Reasons related to watching TV, such as the increase in sedentary life and snacking behaviours in front of the screen instead of physical activities, unhealthy nutrition practices learned from advertisements and programmes that display unhealthy foods and the disruption of normal sleep patterns, can all lead to obesity(Reference Akcay47,Reference Zimmerman and Bell48) . In the current study, most of the students were found to not watch TV and those who watched TV for <1 h were found to have higher ANLS, FNL and INL scores. In the current study, most of the students were found to be not affected by TV commercials and nutrition programmes promoting unhealthy food on TV. Also, our study results showed that students did not watch TV much, they used the right sources of information about healthy nutrition, and that they had the skills to use this information for healthy nutrition behaviours. Also, adolescents in our study were thought to be able to critically evaluate nutritional information, and their capacity to be active in handling nutritional problems and barriers improved.
The energy requirement in adolescents manifests itself primarily as an increase in appetite and the tendency to eat additional food between meals and to eat out increases(Reference Aksoydan and Cakır4). In addition, eating lunch outside of the school cafeteria and the availability of fast food in school canteens increase unhealthy food consumption of students(Reference Kabaran and Mercanligil25). In the current study, the majority of students were found to consume fast food. This is thought to be the effect of media in directing the students to fast-food consumption or the lack of a snack alternative other than fast food at schools. On the other hand, ANLS and FNL scores of those who consumed fewer than three fast-food items a day were high, while those who did not consume any fast food at all showed healthy eating behaviours. According to the results of the study, adolescents who did not consume fast-food items or consumed fewer tended to gain and exhibit healthy eating habits. In the study of Ronto et al. (Reference Ronto, Lauren and Donna28), the consumption of fast food, packaged or processed snacks among adolescents with high food literacy was reported to decrease and the consumption of fruits and vegetables increased. This shows that food literacy is a suitable tool to facilitate healthy eating behaviour of adolescents. Similar to these results, Joulaei et al. (Reference Joulaei, Keshani and Kaveh27) stated that NL had an impact on food intake. They reported that the increase in the FNL score was associated with low sugar intake and improved energy balance in boys and increased milk intake in girls. Also, the increase in the INL score was reported to be likely to increase the energy score, and increases in CNL and NL score to increase vegetable intake(Reference Joulaei, Keshani and Kaveh27). In a systematic review, only one study reported that more frequent food preparation with interactive literacy was associated with increased intake of fruit in adolescent males and both fruit and vegetables in adolescent girls. Besides, the consumption of junk foods such as soft drinks in girls and fried foods in boys was reported to decrease as food preparation increased(Reference Vaitkeviciute, Ball and Harris30).
Sleep, which is one of the basic requirements of an individual, is important for health and quality of life at all ages. The intake of certain foods and beverages is known to affect sleep. Excessive and heavy eating, consumption of chocolate, cola, tea and coffee and insufficient protein intake can disrupt sleep patterns. Weight gain and loss also affect sleep patterns. Weight loss may shorten sleep time, while weight gain may cause prolongation of sleep time(Reference Senol, Soyuer and Akca49). In our study, the adolescents who slept from 7–12 h/d had more positive healthy eating behaviours than those who slept less. This finding suggested that adolescents who had adequate daily sleep exhibited healthy eating attitudes and behaviours.
Inadequate and unbalanced nutrition in adolescents may disrupt the rapidly developing brain and cognitive functions and, thus, affect academic achievement(Reference Meydanlıoglu50). In our study, it can be said that the intermediate level of nutritional habits of adolescents who studied 4–6 h outside school hours may have stemmed from their desire to be academically successful and thinking that incorrect eating behaviours would negatively affect their chances of success.
NL of adolescents was found to explain 12·8 % of the change in the level of FH. This finding is an important result showing the relationship between the two variables. Factors such as food knowledge and food preparation skills have been suggested to have positive effects on dietary intake in young adults. However, a comprehensive study on behavioural changes has shown that knowledge alone is generally not adequate to change the individual’s behaviour, including food choices. Therefore, it is necessary to turn to more inclusive concepts such as NL beyond knowledge to influence changes in behaviours, including dietary choices. Food literacy can play a role in shaping adolescents’ dietary intake(Reference Vaitkeviciute, Ball and Harris30,Reference Carbone and Zoellner37) .
NL is important for assessing changes in nutritional habits. In a study, FH have been reported to be affected by NL(Reference Kalkan51). In our study, adolescents’ ability to obtain, interpret and apply information about nutrition was found to affect healthy eating behaviours.
The limitation of the current study was that some of the informed consent form sent to parents via students was not delivered to parents or returned to the researchers. For this reason, the researchers frequently went to the schools and tried to send the forms to parents through the students again. This caused losses in the sample and cost extra time and expenses for the researchers in reaching the target number of subjects.
Conclusion
Adolescents’ NL and FH were at a good level. NL of the adolescents was determined to affect their FH. NL levels of adolescents were found to be affected by gender, the education level of father, grade, BMI value and daily lifestyle behaviours (engaging in sports, skipping meals, watching TV, fast-food consumption). In addition, lifestyle behaviours, such as playing sports, consuming fast food, skipping meals, daily sleep time, number of meals and time spent studying outside of school, were observed to affect FH. In line with these results, NL levels of individuals and societies should be determined and increased to ensure healthy nutrition. Continuous interventional studies planned by national education programmes are highly important for community health in terms of informing students and families about NL. Also, healthy food should be sold in school canteens. From an early age, adolescents should be helped to gain autonomy in healthy food selection in cooperation with health professionals, teachers, school administration and family. Physical activity/sports awareness and a positive health culture should be promoted, and these should be transformed into a lifestyle. To develop healthy lifestyle behaviours in adolescents, including adequate balanced nutrition and physical activity, awareness of adolescents should be raised, and appropriate health policies should be developed in respect to this issue by creating educational content through social and mass media, which are frequently used by adolescents.
Acknowledgements
Acknowledgements: The current study was undertaken without external funding. The authors would like to express our gratitude to the teachers who greatly supported us in conducting the research and to the students and parents who volunteered to participate in the research. Financial support: The current research received no specific grant from any funding agency, commercial or not-for-profit sectors. Conflict of interest: There are no conflicts of interest. Authorship: B.K. and G.A. designed and conducted the research, wrote the manuscript and had primary responsibility for the final content. B.K and G.A. performed the statistical analyses. All authors read and approved the final manuscript. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Non-invasive Ethics Committee of the Medical Faculty of Dokuz Eylul University (Issue: 2018/29-09). Written or verbal informed consent was obtained from all subjects and their parents. Verbal consents were obtained, witnessed by the researchers and formally recorded. Written approval of the Directorate of National Education was obtained. Also, permissions of the authors of the scales to be used in the study were obtained via email.




