



Plant-based diets, including vegan diets (which do not contain any animal products), are being recommended globally to alleviate the impacts of climate change on the environment and for health benefits(Reference Willett, Rockström and Loken1). In 2017–2018, the percentage of people identified as vegan in the USA and the United Kingdom was around 7 % of the population, representing a sixfold increase in a 3- to 4-year period(Reference Forgrieve2). While the rise of vegan diets may be potentially beneficial for health and the environment, care needs to be taken to ensure their nutritional adequacy. Vitamin B12 is of particular relevance to people on vegan and other plant-based diets, as food sources naturally containing the vitamin are almost exclusively animal-derived(3). Some foods which in early studies were reported to contain vitamin B12, including mushrooms, spirulina, tempeh and other fermented foods, have been found to be rich in inactive analogues of vitamin B12 rather than biologically active forms and are therefore not reliable sources(Reference Koyyalamudi, Jeong and Cho4–Reference Dagnelie, van Staveren and van den Berg6). Studies on vitamin B12 status have found a higher prevalence of vitamin B12 deficiency in not only vegans but also in vegetarians than in omnivores, with vegans and those not taking supplements most at risk(Reference Pawlak, Parrott and Raj7–Reference Pawlak, Lester and Babatunde9). Research on the vitamin B12 status of vegans in Australia is scant. A 1999 Australian study that explored the vitamin B12 status of Seventh-Day Adventist ministers who were not taking supplements (n 298) found that overall, 53 % of the vegetarian (n 234) and vegan subjects (n 11) had serum vitamin B12 below the reference range, compared with 21 % of non-vegetarian subjects (n 53)(Reference Hokin and Butler10). This suggests that vitamin B12 deficiency is potentially an issue amongst Australian vegetarians and vegans.
Vitamin B12 is an essential nutrient that acts as a cofactor in two important intracellular reactions, making it vital for proper red blood cell formation, DNA synthesis and nervous system function. Deficiency can result in serious haematological and neurological dysfunction and in infants can result in failure to thrive, developmental delay and long-term physical and intellectual impairment(Reference Graham, Arvela and Wise11,Reference Honzik, Adamovicova and Smolka12) . Even in the absence of overt deficiency, sub-optimal levels of vitamin B12 can increase levels of homocysteine, which has been independently linked to increased risk of CVD(Reference Humphrey, Fu and Rogers13) and dementia(Reference Werder14). Vitamin B12 status is especially important for infants as inadequacy is associated with increased risk of neural tube defects(Reference Peker, Demir and Tuncer15,Reference Molloy, Kirke and Troendle16) and preterm birth(Reference Rogne, Tielemans and Chong17) as well as with failure to thrive and physical and intellectual impairment(Reference Honzik, Adamovicova and Smolka12). Prevention of vitamin B12 deficiency in infants has been found to be more than a simple matter of preventing deficiency in pregnant and lactating women, due to the evidence that deficiency in infants can occur in the absence of maternal deficiency(Reference Demir, Koc and Ustyol18,Reference Finkelstein, Layden and Stover19) .
Ensuring an adequate intake of vitamin B12 is prudent, especially for those pregnant and lactating, as by the time a deficiency has been detected, irreversible neurological damage can have occurred(Reference Devalia, Hamilton and Molloy20). Furthermore, diagnosis of deficiency is complicated by the wide range of general symptoms and the limitations of commonly used diagnostic methods, such as serum vitamin B12 and holo-transcobalamin II(Reference Harrington21). With the number of people adopting plant-based diets increasing due to both a shift in societal attitudes and in government policy or dietary guidelines(22), the issue of vitamin B12 intake will have broader population implications.
People on a vegan diet are reliant on vitamin B12-fortified foods or supplements to meet their vitamin B12 needs, or risk deficiency, which can have severe and permanent health consequences. Gaining an understanding of the characteristics of women of reproductive age on a vegan diet and their vitamin B12 intake could help inform interventions aimed at ensuring an adequate intake in this vulnerable group. The aims of this present study were to (i) examine the demographic and health characteristics of women of reproductive age (age 18–44 years) on a vegan diet in Australia and compare these to the general population; (ii) identify their sources and intake of vitamin B12 and compare total intake to current reference values and (iii) examine associations between participant characteristics and adequacy of vitamin B12 intake.
Materials and methods
Data collection
A cross-sectional survey was designed to collect information from women of reproductive age on a vegan diet, including information on demographics, diet, health indices and behaviour and intake of vitamin B12 from food and supplements. Questions were primarily sourced from previously validated surveys, the details of which are outlined below. The survey had 150 questions (including the FFQ) and took approximately 20 min to complete. All questions were multiple choice, other than those with simple numeric answers (age, height and weight). The Checklist for Reporting Results of Internet E-Surveys(Reference Eysenbach23) was used as a guideline for the implementation and reporting of the survey details.
Questions relating to age, country of origin, language spoken at home, education, household food security, self-assessed overall health, height, weight, smoking, health conditions, intake of fruit, vegetables, salt and alcohol were worded identically to those in recent Australian National Health Surveys(24–26) to facilitate comparison with the general population. Additionally, the postcode of participants was collected and used to calculate their socio-economic index for area decile; a measure of socio-economic conditions used by the Australian Bureau of Statistics(27). Illustrations used to assist data collection in the surveys (such as to illustrate serve sizes of fruit, vegetables and alcohol) were included (with permission from the Australian Bureau of Statistics) for further consistency.
In order to estimate participants’ intake of vitamin B12 from food and drinks, a vitamin B12-specific FFQ based on a tool previously validated in New Zealand was used(Reference Mearns and Rush28). In adopting and adapting this tool, best practice guidelines for dietary assessment in health research were considered(Reference Cade, Warthon-Medina and Albar29). The FFQ was semi-quantitative and asked participants’ frequency of consumption of individual vitamin B12-containing foods in the past 3 months, providing eight answer options for frequency and four to five answer options for usual serve size, which were based on volume (e.g. ‘< ¼ cup’) or portion size (e.g. ‘one sausage’).
Under the Australian and New Zealand regulations, only plant-based milks and other dairy alternatives, meat analogues, yeast extracts and flakes, energy drinks and meal replacement products can be fortified with vitamin B12 up to specified levels, and fortification is at the manufacturer’s discretion(30). Products in these categories in supermarkets, health food stores and vegan grocery shops were examined to identify those which were fortified. To ensure that all available vitamin B12-fortified foods were included, five Australian Accredited Practising Dietitians who specialise in plant-based nutrition were asked to check to ensure that no currently available fortified foods had been omitted. A total of 105 vegan products fortified with vitamin B12 available for sale in Australia were identified. Colour photographs of all products were included in the online survey to enable easier identification. The vitamin B12 content of each product was checked (from labelling and/or contact with manufacturers). As part of the survey development process, content validation was undertaken by the aforementioned five dietitians. After this step, face validation was conducted with fifteen women of reproductive age who were on a vegan diet.
Participants and recruitment
Participants for the study were recruited via Australian-based Facebook groups that had a focus on veganism. Groups based in each state and in both metropolitan and regional areas were targeted to recruit participants from different areas of Australia. Potential participants were invited via a Facebook post to complete an anonymous online survey and a link was posted to the survey information page. All respondents were placed in a draw to win one of two vouchers valued at $250 each. Adaptive questioning was used, and cookies were used for the duration of the survey period to prevent participants from submitting the survey more than once. Recruitment and survey completion took place over a 2-month period in 2018. In 2016–2017, 97 % of Australians aged 18–44 years were Internet users(31), and over 90 % of Australians women in that age group were users of Facebook in 2018(Reference Hughes32).
Inclusion criteria for participation in the current study were must be female, aged between 18 and 44 years, have been on a vegan diet (defined as a diet free of animal products) continuously for at least the past 6 months, intended to stay on a vegan diet indefinitely, currently reside in Australia and had done so for at least 21 months out of the past 2 years.
Data preparation
The responses were checked for completion after submission, and the amount of missing data was determined for each variable and for each case. The pattern of missing data was analysed using both Little’s Missing Completely at Random test(Reference Little33) and separate variance t-tests. The resulting P-values were all above 0·05, indicating that the missing values were missing completely at random (Missing Completely at Random). As the amount of missing data was very small (0·39 % overall and below 1·6 % for all questions), simple pairwise deletion of data was used where data were missing.
Participants’ intake of vitamin B12 from food was calculated from the FFQ from the number of serves of each of the vitamin B12-fortified foods and their frequency of consumption. Participants’ intake of vitamin B12 from supplements was calculated by multiplying the dose and frequency of the supplement they took containing the most vitamin B12 and that of the supplement containing the second highest amount of vitamin B12 (if more than one B12-containing supplement taken), adding these together and calculating daily dose equivalent. The intake of vitamin B12 of participants was compared with the Australian Recommended Dietary Intake (RDI)(34) and to the available data on intake of the vitamin of women of comparable age in the general Australian population(35).
Data relating to intake of fruit, vegetables and alcohol were categorised according to whether intake met current Australian Dietary Guidelines(36) for minimum intake of 300 g of fruit/d and 375 g of vegetables (563 g for lactating women) and whether the guidelines for short-term high-risk consumption of alcohol (no more than 40 g of alcohol on any single occasion)(37) were exceeded or not.
Statistical analyses
The online calculator provided by the Australian Bureau of Statistics was used to first determine the number of participants required to obtain a representative sample of women aged 18–44 years on a vegan diet in Australia(38). There are currently no published estimates on the size of the vegan population in Australia, so an estimate was made using two sources: (i) the percentage of women aged 18–44 years people self-reporting as ‘vegetarian’ and as ‘avoiding dairy products’ in a 2016 consumer poll(Reference Morgan39) and (ii) an estimate made by the administrator of several of the largest Facebook groups for vegans in Australia (personal communication, S. DeSilva, 23/2/17). These methods estimated the number of females aged 18–44 years on a vegan diet in Australia in late 2017 as between 70 000 and 150 000. Using the top-end of the range as the population size and specifying a confidence level of 95 % and a CI of 0·05, the online calculator determined that the minimum sample size required for the current study was 384(38).
Data were analysed using SPSS Version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. IBM Corp). A P-value of <0·05 was considered statistically significant, although due to the large number of variables analysed, a Bonferroni correction was applied when considered appropriate, such as when reporting associations based on a large number of independent analyses without pre-planned hypotheses(Reference Armstrong40).
Descriptive statistics were used to summarise information on the demographics, dietary and health behaviours of the group. Continuous variables were assessed for normality and the range, and as appropriate, median, mean and sd were determined and reported. Categorical variables were presented as frequencies (percentages). Where available, data were compared with that of women from the general Australian population of comparable age using data from the Australian Bureau of Statistics. T-tests were used to determine the significance of differences observed.
Initially, χ 2 tests were used to explore the association between the characteristics (demographic, health-related variables) of the sample and the following dependent variables: (i) whether the RDI for vitamin B12 was met or not and (ii) whether a supplement containing vitamin B12 was taken or not.
Binomial logistic regression was conducted step wise to identify the influence that the independent variables most strongly associated (P < 0·1) with the dependent variables had on whether the RDI was met or not, and whether a supplement containing vitamin B12 was taken or not.
Results
A total of 1530 completed online surveys were submitted over a 6-week period. Nineteen people were exited at commencement due to confirming that they did not meet the inclusion criteria. An additional 990 people commenced the survey but did not complete or submit it, resulting in a completion rate of 61 %. As submission of the survey was taken as consent to participate, partially completed surveys were not used. Analysis of the questions answered in these surveys revealed that non-completers did not differ significantly from those who had submitted the survey.
Characteristics of the participants
Demographic, health and other data on the characteristics of participants are summarised in Tables 1 and 2.
Table 1 Demographic and health characteristics of Australian vegan women aged 18–44 years (n 1530) compared with women of comparable age in the general population of Australia(45,49,75–84)
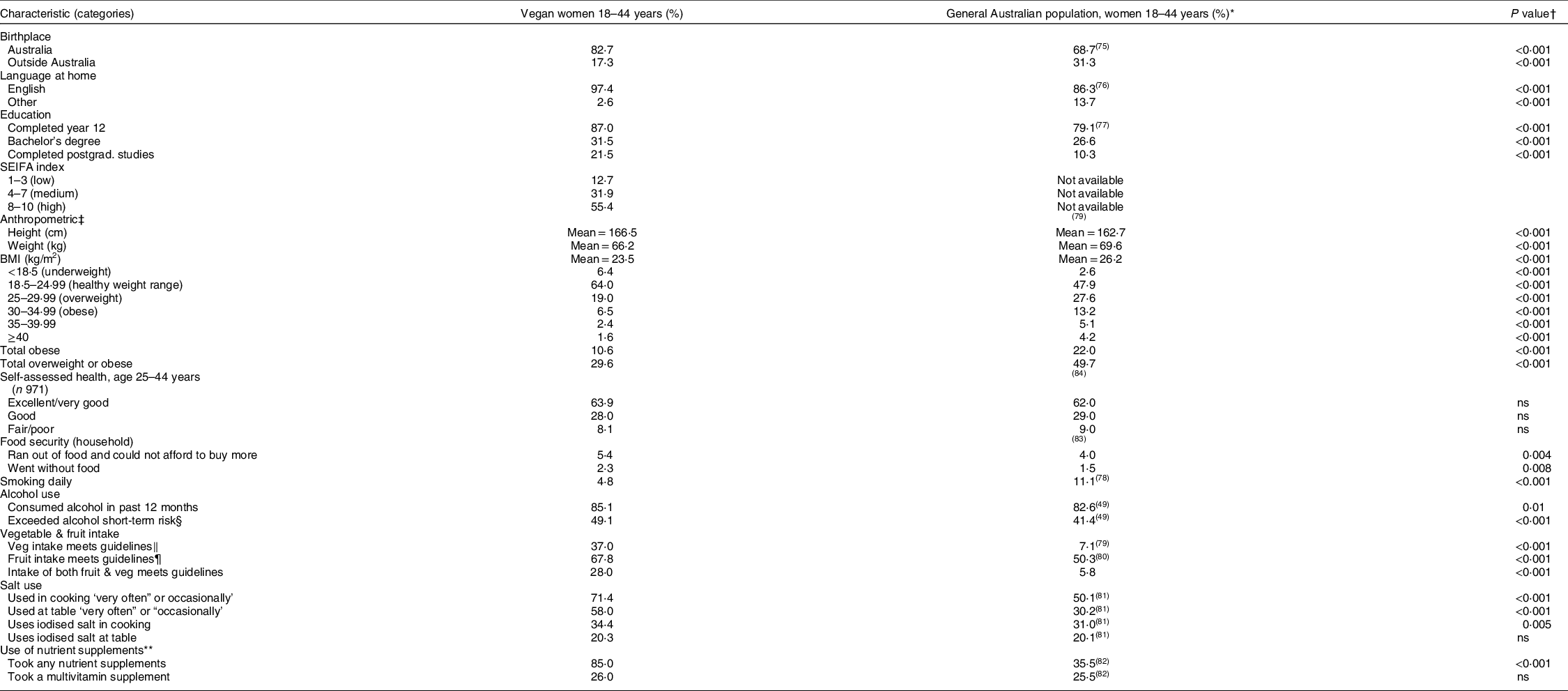
ABS, Australian Bureau of Statistics; SEIFA, Socio-Economic Index for Areas, an index of socioeconomic status measured on a scale of 1 to 10, with the higher values indicating greater relative advantage.
* ABS data.
† P value determined by t-test.
‡ ABS data based on measured heights and weights, not self-reported.
§ Defined as no more than four standard drinks on any single occasion(37).
‖ At least 375 g/d, not including legumes.
¶ At least 300 g/d.
** ABS figures based on past week, not past 3 months.
Table 2 Additional participant data on vegan women aged 18–44 years (n 1530)

Almost three-quarters (73·9 %) of participants reported taking a supplement containing vitamin B12 in the preceding 3 months and almost two-thirds (64·9 %) reported taking other supplements besides those containing vitamin B12. Of these participants, 10·7 % were not taking vitamin B12 in any form. The most frequently reported non-B12 supplement taken was Fe, with 33·2 % of participants reporting taking Fe in the past 3 months, followed by Mg (18·6 %), vitamin D (18·0 %), vitamin C (14·8 %), n-3 supplements (13·5 %) and Zn (11·3 %). Other single-nutrient supplements taken (by <6 % of participants for each supplement) included Ca, B1, B2, B3, B6, folic acid, iodine, Se, vitamin A, vitamin K and vitamin E.
Vitamin B12 intake and sources
Details on the mean amount of vitamin B12 obtained from the fortified foods consumed by study participants and their contribution to the total are provided in Table 3. The frequency of consumption of vitamin B12-fortified foods varied considerably between participants, ranging from never to more than 3 times/d over the past 3 months.
Table 3 Vitamin B12 supplied by fortified foods (µg/d) and percentage of total intake (mean intake of all participants) (n 1530)

Frequency of vitamin B12 supplementation varied from never (25·3 %) to daily (19·4 % of participants), with 57 % of participants taking a single-nutrient vitamin B12 supplement. Various forms of vitamin B12 were taken, with oral cyanocobalamin being the most frequently taken (33·7 % of participants), but 20·8 % reported not knowing what form they were taking.
The mean intake of vitamin B12 from fortified foods was 1·16 +/− 1·2 µg/d (range 0–14·4 µg). From supplements, the median intake was 71·7 µg (range 0–10 000 µg), and the median total intake was 74·4 µg (range 0–10 001·4 µg)/d. Over 99·5 % of vitamin B12 intake was from supplements. To enable comparison with other studies that reported average daily intake of participants, the average total intake was computed and was 262·2 (+/− 531·0) µg/d.
Adequacy of vitamin B12 intake
The RDI for vitamin B12 is 2·8 µg daily for lactating women, 2·6 µg during pregnancy and 2·4 µg for other adults, and the estimated average requirements are 2·4, 2·2 and 2·0 µg, respectively(34). The percent of participants meeting the estimated average requirement and RDI from food, supplements and from total intake is shown in Table 4.
Table 4 Adequacy of vitamin B12 intake from food and supplements and in total (n 1530)

EAR, estimated average requirement; RDI, recommended dietary intake.
Of the 74 % of participants meeting the recommended intake of vitamin B12, 75·4 % did so by taking a single-nutrient vitamin B12 supplement, 19·2 % did so by taking a multivitamin or other supplement containing vitamin B12 and 5·4 % met the recommended intake of vitamin B12 from fortified foods alone (without supplementing).
Relationship between adequacy of vitamin B12 intake and participants’ characteristics
A binomial logistic regression was performed to ascertain the influence of participant characteristics on meeting the RDI for vitamin B12. Of the predictor variables, only three were statistically significant: taking a B12 supplement (OR 110·5, 95 % CI 71·8, 170·2), being on a vegan diet for greater than 2 years (OR 1·74, 95 % CI 1·12, 2·69) and using iodised salt (OR 1·69, 95 % CI 1·06, 2·70), as shown in Table 5.
Table 5 Participant characteristics predicting likelihood of meeting recommended dietary intake for vitamin B12 (as predicted by logistic regression model) (n 1426)*

* Variables entered at Step 1: age, language at home, Socio-Economic Index for Area low or other), state of residence (Western Australia/South Australia or other), period on vegan diet, smoking status, food security, whether consumes alcohol, vegetable intake, fruit intake (i.e. whether meets guidelines or not), use of iodised salt, children since vegan, currently pregnant or lactating, prefers organic food, whether a B12 supplement was taken or not and whether any other supplements were taken.
Relationship between supplementation with vitamin B12 and participants’ characteristics
Binomial logistic regression identified that whether a participant took any other (non-B12 containing) supplement or not had the strongest association with whether a supplement containing vitamin B12 was taken or not (OR 3·31, 95 % CI 2·54, 4·31). Other predictor variables identified as significant were using iodised salt (OR 1·79, 95 % CI 1·34, 2·40), meeting recommended fruit intake (OR 1·59, 95 % CI 1·20, 2·10), meeting the recommended vegetable intake (OR 1·49, 95 % CI 1·13, 1·98), having a BMI <30 (OR 1·67, 95 % CI 1·12, 2·51), being over 35 years of age (OR 1·40, 95 % CI 1·05, 1·83) and having food security (OR 1·92, 95 % CI 1·15, 3·22), as shown in Table 6.
Table 6 Factors predicting likelihood of supplementing with vitamin B12 (as predicted by logistic regression model) (n 1530)*

* Variables entered at Step 1: age (≥35), takes non-B12 supps, iodised salt used, time period on vegan diet, fruit intake meets guidelines, food security, Socio Economic Index For Area, residing in South Australia/Western Australia or elsewhere, children since vegan, vegetable intake meets guidelines, currently pregnant or lactating, birth place, education, smoking status, prefers organic, whether consumes alcohol, blood tests for vitamin B12 in past 3 or next 3 months, BMI < 30, self-assessed health.
† Defined as did not ever run out of food without being able to afford to buy more.
Discussion
The key findings of the current study are: (i) the demographic and health characteristics of women on a vegan diet in Australia differ substantially from women in the general population; (ii) only 10·7 % met the recommended intake of vitamin B12 from food and 26·1 % did not meet the recommended intake from food and supplements combined; and (iii) taking a vitamin B12 supplement was the strongest predictor of meeting the RDI, and the significant predictors of doing this were greater age, taking other types of supplements, positive health behaviours and having food security. This is the first known study to explore the demographic and health characteristics of vegan women in Australia and adds to existing literature from overseas studies. It is also the first study to examine the intake of vitamin B12 of women of reproductive age in Australia, providing insight into a potential problem in this vulnerable group. To our knowledge, the number of vegan participants (n 1530) is exceeded only by the United Kingdom’s EPIC-Oxford Study (n 2596 vegans)(Reference Davey, Spencer and Appleby41) and the North American Adventist 2 Study (n 5548 vegans)(Reference Orlich and Fraser42) and demonstrates the ability of targeted use of social media to generate a large number of participants in a relatively short time period with minimal cost.
In comparison with women aged 18 to 44 years in the general Australian population, participants in the current study were more likely to be born in Australia and speak English at home and had a higher index of socio-economic advantage. They also had higher educational attainment than the general population, a finding common to some other studies on vegans(Reference Davey, Spencer and Appleby41–Reference Vollmer, Keller and Kroke43), apart from the French Nutrinet-Sante study which reported that vegans had lower educational attainment and income than meat-eaters(Reference Allès, Baudry and Méjean44).
The prevalence of overweight and obesity in this group was substantially lower at 29·6 % compared with 49·7 % in women of comparable age in the Australian population(45). However, the Australian Bureau of Statistics data are based on measured heights and weights so the lower BMI (−2·6 kg/m2) in vegans reported here needs to be interpreted with caution because of the inherent limitations in self-reported height and weight data, which tend to underestimate BMI(Reference Burton, Brown and Dobson46). However, several other studies have found vegans to have significantly lower BMI than non-vegans(Reference Davey, Spencer and Appleby41–Reference Allès, Baudry and Méjean44,Reference Kristensen, Madsen and Hansen47) .
The lower smoking rate amongst participants could indicate a greater health consciousness in this group, or it could be because tobacco use may be rejected by vegans as a result of tobacco companies testing on animals(Reference Harris, Tally and Schmidt48). Lower smoking rates amongst vegans have been found in several studies(Reference Orlich and Fraser42), while in others the rates did not differ significantly between dietary groups(Reference Davey, Spencer and Appleby41).
The finding that the prevalence of alcohol consumption and drinking in excess of the single occasion risk guidelines was higher amongst vegan women than women in the general population(49) is not in line with reports from other studies comparing vegans to the general population(Reference Davey, Spencer and Appleby41–Reference Vollmer, Keller and Kroke43,Reference Sobiecki, Appleby and Bradbury50–Reference Gili, Leeson and Montes-Chañi53) . Part of the reason for the differing result regarding alcohol consumption in the present study could be because in some other studies there was a higher proportion of subjects who were vegan for health reasons and/or were members of religions which encourages the avoidance of alcohol consumption. In the present study, only 12·1 % of participants maintained a vegan diet for health reasons and only 0·03 % participants cited religious or spiritual reasons for adopting a vegan diet. It has been reported that women living in the highest socio-economic areas in Australia are 1·3 times as likely to exceed this guideline as women in the lowest socio-conomic areas(54), so the higher socio-economic status of vegans may in part explain the higher alcohol intake. In any case, the high reported incidence amongst vegan women (50·8 %) of exceeding the guideline for single occasion alcohol consumption in the past 12 months indicates that it cannot be assumed that vegans have consistently favourable health practices.
While participants in the current study reported much higher intakes of fruit and vegetables than women of comparable age in the general population, only 37 % met the recommended intake of vegetables and only 28 % met the recommended intake of both fruit and vegetables (compared with 7·1 % and 5·8 %, respectively, amongst women of comparable age in the general population). Studies have consistently reported a higher intake of fruit and vegetables by vegans than other dietary groups(Reference Allès, Baudry and Méjean44,Reference Gili, Leeson and Montes-Chañi53,Reference Waldmann, Koschizke and Leitzmann55–Reference Beezhold, Radnitz and Rinne57) .
The finding that the majority of participants in the current study reported adopting and maintaining a vegan diet because of animal welfare or animal rights concerns is a similar result to that reported in several other studies(Reference Vollmer, Keller and Kroke43,Reference Janssen, Busch and Rodiger58,Reference Radnitz, Beezhold and DiMatteo59) , although in two studies from the United States, health reasons were more commonly cited(Reference Dyett, Sabaté and Haddad60,Reference Miki, Karlsen and Livingston61) . Three-quarters of participants in the current study had been on a vegetarian diet before adopting a vegan diet, which could impact their vitamin B12 status, given that lacto-ovo vegetarians are at higher risk of deficiency than omnivores(Reference Gilsing, Crowe and Lloyd-Wright8).
The mean intake of vitamin B12 from food was 1·16 µg/d in the current study which is less than half of the RDI(34) and less than one-third of that consumed by the women in the general population of Australia(35), although the latter was determined by 24-h recall. The different methodologies used (FFQ compared with 24-h recall) affect the accuracy of the estimate of the difference in vitamin B12 intake between the two different dietary groups, so should be interpreted with caution. The finding that the main food sources of vitamin B12 in this group were fortified meat analogues and unflavoured plant milks but that these only provided a total average intake of 0·9 mcg of vitamin B12/d indicates that at current fortification levels, alternatives to meat and milk are not consumed in adequate amounts by this group to meet vitamin B12 needs.
The intake of vitamin B12 from food in the current study was a little less than that reported in vegans in Spain(Reference Menal-Puey, del Ruste and Marques-Lopes56) and higher than the intake reported in several other European countries(Reference Allès, Baudry and Méjean44,Reference Kristensen, Madsen and Hansen47,Reference Schüpbach, Wegmüller and Berguerand51,Reference Elorinne, Alfthan and Erlund62–Reference Majchrzak, Singer and Manner64) and amongst vegans in the United Kingdom(Reference Davey, Spencer and Appleby41,Reference Sobiecki, Appleby and Bradbury50,Reference Draper, Lewis and Malhotra65) . In contrast, the intake of vitamin B12 from food in the current study was much lower than that reported amongst those on a vegan diet in the USA and Canada, where the mean intake of vitamin B12 was 4·78 µg/d(Reference Damayanti, Haddad and Jaceldo-Siegl66), which reflects the far greater range of foods which are fortified with vitamin B12 in the United States. This is an important consideration when using or adapting information materials on vitamin B12 or vegan diets developed in the USA for use in Australia or other countries with more restrictive fortification legislation. Using materials generated in other countries could result in errors such as attributing fortification to foods that are not actually fortified in Australia((67), p12), or down-playing the importance for vegans to supplement with vitamin B12 (68), which could put people on a vegan diet at risk of deficiency.
Based on the reported intake patterns of the participants in the present study, consumption of fortified foods is inadequate to meet the recommended intake of vitamin B12 for almost 90 % of women of reproductive age on a vegan diet in Australia, which is a similar finding to the French Nutrinet-Sante Study(Reference Allès, Baudry and Méjean44), and highlights the importance of supplementation for vegan women. The average daily intake of 261 µg/d from supplements by participants in the current study was higher than the 96·0 µg/d reported amongst North American vegan Seventh Day Adventists (n 67)(Reference Damayanti, Jaceldo-Siegl and Beeson69), the 25 µg/d reported in the Danish study (n 70)(Reference Kristensen, Madsen and Hansen47) or the 0·25 µg/d estimated in Draper’s UK study (n 30)(Reference Draper, Lewis and Malhotra65).
While it was encouraging that most participants did supplement with vitamin B12, the wide range of methods of vitamin B12 supplementation practices used by this group suggest that there may be a lack of clear guidelines (and/or awareness of these) on how to most effectively supplement. Further research on the clarity and accessibility of current guidelines on vitamin B12 supplementation for vegans would be useful, as well as on the different forms of cobalamin and their efficacy at preventing deficiency in this group.
It is of concern that a substantial proportion of women in the current study were not meeting the Australian recommended intake (26·1 %) or the Estimated Average Requirement (23·3 %) of vitamin B12 which puts them at risk of deficiency. It is not only the women themselves that are at risk, as even short-term restriction in intake of vitamin B12 during pregnancy or lactation has the potential to cause adverse effects on infants, not only during development but also later in life(Reference Finkelstein, Layden and Stover19,Reference Rosenblatt and Whitehead70,Reference Knight, Shields and Brook71) . Furthermore, as over half of the women on a vegan diet reported that children in their care consume an exclusively vegan diet, this raises concerns about the adequacy of vitamin B12 intake in these children when caregivers’ intakes are inadequate. Studies on the feeding practices of vegan parents and the nutritional status of children on a vegan diet in Australia would be useful.
Given the relative scarcity of vitamin B12 in vegan foods in Australia, it was not unexpected that taking a B12 supplement was the most significant predictor of meeting the RDI. Several of the predictor variables associated with taking a vitamin B12 supplement, i.e. taking other supplements, using iodised salt, meeting recommended intakes of fruit and vegetables and having a BMI under 30 kg/m2 suggest a greater awareness of nutrition and health-promoting behaviour in those supplementing. The finding that having food security was also a predictor of supplementation suggests that the cost of supplements may be a deterrent to those with limited financial resources. The finding that being over 35 years of age was also a predictor of supplementing suggests that in interventions aimed at increasing supplementation rates in this demographic, targeting those under 35 years of age could be a priority.
Limitations of the current study include that participants were self-defined as being on a vegan diet, and no additional measures were undertaken to confirm this. The use of a self-selected convenience sample of Facebook users could have resulted in a selection bias and may not be representative of all vegan women of reproductive age in Australia. Comparison with women in the general Australian population needs to be treated with caution for the same reason. Participants were members of Facebook groups specifically for vegans, where vitamin B12 is frequently discussed. As a result, awareness of vitamin B12 may be relatively high and possibly result in a higher intake of vitamin B12 than in those who are not members of vegan Facebook groups.
Although the wording of questions relating to health behaviours was identical to that in National Health Surveys, the latter were conducted via face-to-face interviews rather than the online survey method employed for the current study, and the difference in results due to this methodological difference is unknown. The BMI were based on self-reported height and weight and are not directly comparable with the measured BMI in the Australian National Health Survey.
Another important limitation of the current study is the way that the intake of vitamin B12 intake from supplements was estimated and then compared with the RDI. Assumptions were made relating to equivalency between mean daily doses, formulation of supplements used (i.e. whether stand-alone or compounded with other nutrients), mode of ingestion, form of vitamin B12 used and the validity of comparing mean intake from food to mean intake from supplements. The latter assumption is the most significant because the RDI is based on intake from food, with the assumption that vitamin B12-containing foods will be consumed at each meal, and that absorption rate is 50 %(72), whereas supplements were consumed much less frequently than this and absorption rates are considerably lower(Reference Adams, Ross and Mervyn73,Reference Chanarin74) . Therefore, an individual who is ostensibly meeting the recommended intake of vitamin B12 via supplements may in fact be at risk of deficiency. Further detailed analysis of the data would be required to reveal the magnitude of the ramifications of this limitation.
Strengths of the current study were the large sample size compared with most other studies on vegans, the broad range of information obtained and the design enabling demographic and health characteristics to be compared with women of comparable age in the general Australian population. The results relating to vitamin B12 intake from food were based on a validated FFQ, and the survey underwent content validity by experts in the field and face validity by women in the target audience.
Conclusion
The current study has identified that that the mean daily intake of over one-quarter of the women of reproductive age on a vegan diet did not meet the recommended intake of vitamin B12 and almost a quarter did not meet the estimated average requirement. This is of concern given the potential deleterious effects not only on adults but also on their infants. Supplementing with vitamin B12 is the most effective way for those on a vegan diet to meet their vitamin B12 needs, but a substantial proportion of participants in the current study were failing to do so. An increase in the uptake of plant-based diets and avoidance of animal products are likely to result in an increase in prevalence of diet-related vitamin B12 deficiency unless the issue of inadequate intake is addressed. Further research on how to identify and implement strategies for ensuring vitamin B12 adequacy amongst people on a vegan diet is required.
Acknowledgements
Acknowledgements: The authors would like to acknowledge the Accredited Practising Dietitians Lucy Taylor, Jane Whitbread, Angela Saunders, Dr Kate Marsh, Shirley Chan and Linda Smillie for assistance with the survey development and validation and also to the Queensland University of Technology students who generously helped road test the surveys. Additionally, we would like to acknowledge the 1,530 anonymous vegan women who completed the initial survey for their generosity in giving up their time to participate in the current study. Financial support: Amanda Benham received funding to complete this project in the form of an Australian Government Research Training Program Scholarship. The Australian Government had no role in the design, analysis or writing of this article. Conflict of interest: Danielle Gallegos is currently supported by the Queensland Children’s Hospital Foundation via a philanthropic grant from Woolworths. Authorship: All authors conceptualised the project. A.B. designed the research, survey and did all the primary analyses. A.B. undertook preliminary interpretation of the results with assistance from K.H., M.H.J. and D.G. A.B. wrote the draft of the paper and all authors have been involved in editing the article and have approved the final version. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Queensland University of Technology’s Office of Research Ethics and Integrity (approval #1700000950). Informed consent was obtained from all subjects by making it clear that proceeding to the online survey after reading the information sheet and submitting their results was indicative of informed consent.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021001695








