



Non-communicable diseases (NCD) are a growing threat in low- and middle-income countries. An estimated 85 % of worldwide deaths associated with NCD occur in low- and middle-income countries (Reference Mathers and Loncar1–Reference Gakidou, Afshin and Abajobir3). It is projected that NCD cases will overtake infectious diseases by 2030 in sub Saharan Africa (SSA)(Reference Mathers and Loncar1,Reference Haddad, Hawkes and Udomkesmalee2,Reference Yach, Hawkes and Gould4,5) . NCD account for approximately 27 % of total deaths annually in Uganda(6). Key risk factor for NCD is overweight. Overweight and obesity prevalence are increasing in urban Uganda. Prevalence of overweight is higher among women than in men at 28·8 % and 15·8 %, respectively(7). Similarly, obesity is at 15·6 % in women and 3·1 % in men(7). Despite the rising cases of overweight and obesity in urban Uganda, it is not yet recognised as a public health problem(8). The increasing burden of NCD in urban Uganda reflects an urgent need to develop efficient preventative strategies(8,Reference Holdsworth, Kruger and Nago9) .
Key modifiable risk factors for overweight and obesity are dietary behaviour and physical activity(Reference Alwan10,Reference Cecchini, Sassi and Lauer11) . Dietary patterns observed among urban Ugandans showed poor alignment with WHO recommendations(7,12) . It is estimated that 90 % of urban Ugandans do not consume 400 g of fruits and vegetable daily as recommended. Studies depict an increase in physical inactivity in urban Uganda, especially among women(7,Reference Guthold, Stevens and Riley13) . At the base of these dietary and physical inactivity behaviours are socio-cultural and environmental determinants which are conceptually complex. Understanding determinants of dietary and physical activity behaviours is a prerequisite for health interventions(Reference Beagan and Chapman14–Reference Eldredge, Markham and Ruiter16). Interventions tailored to existing beliefs are effective in improving behaviour(Reference Eldredge, Markham and Ruiter16). In SSA, dietary decisions are made by mostly women and they directly influence the family’s dietary behaviours(Reference Phillips, Comeau and Pisa17–Reference Van, Riet, Den Hartog and Mwangi20). Hence, understanding determinants of dietary and physical activity decisions in women is vital. Our topical systematic review on determinants of dietary and physical activity behaviours among women of reproductive age (WRA) in urban SSA found food knowledge gaps, time and financial barriers, culture (prestige linked to weight gain and consumption of animal protein) and family network to be important determinants of dietary behaviours(Reference Yiga, Seghers and Ogwok21). Cultural beliefs instigating several misconceptions (mainly gender stereotypes) and fast changing transport environment chiefly mediated physical activity behaviours. However, evidence was from mainly West and South Africa. Accordingly, the determinants of dietary and physical inactivity behaviours are not well understood in urban Uganda and East African region. The study qualitatively explored the determinants of dietary and physical activity behaviours among WRA in urban Uganda to guide interventions.
Methodology
A consolidated criteria for reporting qualitative research was followed as a guideline to report the qualitative study(Reference Tong, Sainsbury and Craig22).
Study design and participants
Generic qualitative interpretative research design was used. The qualitative study involved women aged 18–45 years living in Kampala, Uganda. Participants were recruited through institutional religious women groups. A collaboration was established with Our Lady of Africa Parish, Mbuya and Beauty for Ashes International Rescuing Ministries. The two institutions were selected owing to their established social networks and community outreach across Kampala. The inclusion criteria were gender (women) and age (18–45 years). No exclusion was done on the basis of health conditions or anthropometric indices. This was to ascertain determinants in the general population not those with specific medical conditions.
Theoretical framework
A modified theoretical framework (Fig. 1) was used to guide the development of FGD. The basis of the framework was the theory of planned behaviour(Reference Godin and Kok23) complemented with specific constructs from social cognitive theory(Reference Bandura24), health belief model(Reference Abraham and Sheeran25), precaution adoption process model(Reference Weinstein, Sandman, Blalock, Glanz, Rimer and Viswanath26) and social support theory(Reference Catherine, Barbara, Glanz, Rimer and Viswanath27). Complementarity was important since no theory explains behaviour independently(Reference Eldredge, Markham and Ruiter16). The above theories have been shown to include constructs which explain dietary and physical activity behaviours(Reference Godin and Kok23,Reference Hagger, Chatzisarantis and Biddle28–Reference Marcus, Williams and Dubbert32) . The adapted model can be described as follows; according to theory of planned behaviour, intention (motivational force to perform an action) is the proximal determinant of behaviour. Intention in turn is determined by attitude, subjective norms and self-efficacy. At the same time, barriers and awareness (a construct from precaution adoption process model)(Reference McEachan, Lawton and Jackson30,Reference Springvloet, Lechner and Oenema31) might impede intention from being translated into behaviour. Attitudes are further determined by behavioural beliefs and evaluation of behavioural outcomes(Reference Godin and Kok23). However, attitude may as well be influenced by perceived severity to lifestyle related to NCD (a construct from health belief model). Hence, the model was complemented with perceived severity. According to social cognitive theory(Reference Bandura24), knowledge and skills could have an influence on self-efficacy, consequently adding the two constructs to the model. Dietary and physical activity behaviours are strongly influenced by environment as shown in social cognitive theory(Reference Bandura24,Reference Kelder, Hoelscher, Perry, Glanz, Rimer and Viswanath33,Reference Kremers, De Bruijn and Visscher34) .Therefore, environment construct was added. Finally, social support has been shown to have a large influence on behaviour(Reference Seghers, Van Hoecke and Schotte29,Reference Rhodes and Pfaeffli35) .
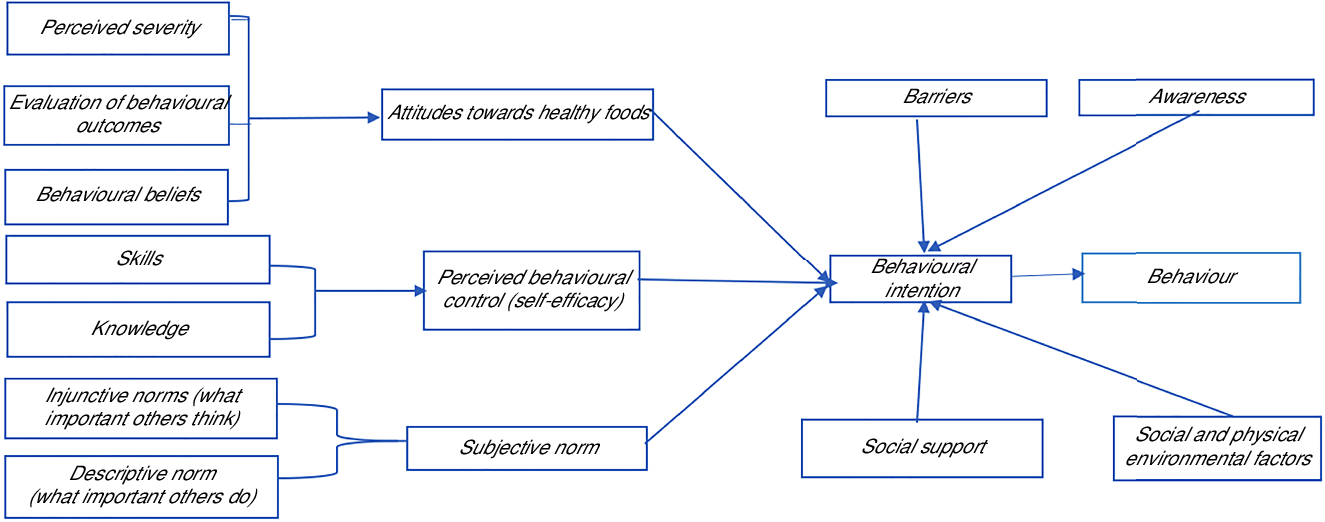
Fig. 1 Modified theoretical framework for designing focus group discussions, source – the theory of planned behaviour (TPB)(Reference Godin and Kok23) complemented with specific constructs from social cognitive theory (SCT)(Reference Bandura24), health belief model (HBM)(Reference Abraham and Sheeran25), precaution adoption process model (PAPM)(Reference Weinstein, Sandman, Blalock, Glanz, Rimer and Viswanath26) and social support theory(Reference Catherine, Barbara, Glanz, Rimer and Viswanath27)
Data collection
Semi-structured questioning routes for both behaviours were developed (see online supplementary material, Supplemental Tables 1 and 2), pre-tested on undergraduate female students of Kyambogo University, Uganda, and then refined. FGD were conducted in January/February 2019. Separate FGD for dietary and physical activity behaviours were conducted. Different sets of participants were recruited to study each behaviour. Women were recruited using opportunistic sampling, a purposive non-probability approach in which participants are recruited from existing groups. Two contact personnel coordinated the recruitment from the existing women groups across the sub parishes of Mbuya parish and Beauty for Ashes. Furthermore, for homogeneity purposes and confidence of expression during the discussions, WRA were further categorised into young adults (18–34 years) and adults (35–45 years). A researcher with experience in qualitative research moderated FGD with a trained silent observer who took notes on non-verbal behaviour and group interactions(Reference Krueger and Casey36). The FGD were conducted in English or Luganda depending on language preference by participants. Open-ended questions were followed up by more specific probes to clarify and extend responses. Visual listings (see online supplementary material, Supplemental Tables 3 and 4) of healthy and unhealthy foods and physical/sedentary activities were used during the FGD. The FGD were audio-recorded and lasted between 60 and 90 min. Before the start of each FGD, a debriefing on the goal of study was held and the participants consent to participate was requested. Each participant signed an informed consent. Participants received healthy refreshments (bottled water and banana) and transport refund.
Data analysis
Records were transcribed verbatim, translated into English for the FGD conducted in Luganda and cross-checked by two researchers. Data were analysed following inductive thematic content analysis approach(Reference Elo and Kyngäs37,Reference Burnard, Gill and Stewart38) . Open coding was conducted independently by two researchers to generate an initial coding framework. The two researchers discussed the generated frameworks for contrasts and similarities. Generated codes from all transcripts were then organised together into a second coding framework. Codes with overlapping content were grouped into categories. Correspondingly, overlapping categories were grouped into themes using theoretical ideas from the modified theoretical framework to generate final coding frameworks. Two researchers synchronised the final coding frameworks (see online supplementary material, Supplemental Tables 5 and 6), which was then shared with the third researcher. Each theme was then allocated a colour. Each transcript was then worked through and data fitting under a theme marked with the corresponding colour theme. Inclusion of factors was based on the frequency, specificity, emotion and extensiveness of the quotes related to the factor(Reference Krueger and Casey36). The non-verbal behaviour and group interactions were well considered.
Results
After twelve FGD, six groups per behaviour and three per age category, no new themes were coming up. Overall, twelve FGD were conducted with group sizes ranging between five and eight members.
Socio-demographic characteristics of participants
Details of socio-demographic characteristics of participants are presented in Table 1. In total, 81 participants took part in the study. Majority (65·4 %) were single and were either unemployed (19·8 %) or worked in the informal sector (29·6 %). About half (53·1 %) of the participants had university/tertiary qualification.
Table 1 Socio-demographic characteristics of participants
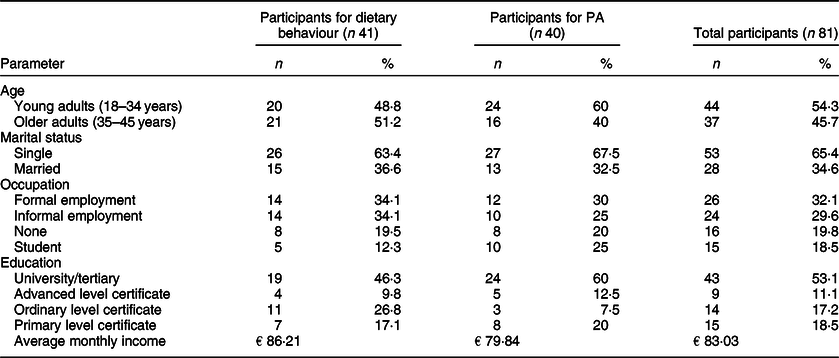
PA, physical activity.
Determinants of dietary and physical activity behaviours
The emergent themes from the data analysis are schematically arranged following the modified theoretical framework described in Fig. 1. The identified themes covered the three broad levels of intra-individual, socio-cultural and environmental levels. Results are presented according to these three levels.
Determinants of dietary behaviour
Twenty-one factors organised under twelve themes were identified to have an influence on dietary behaviour, Fig. 2.
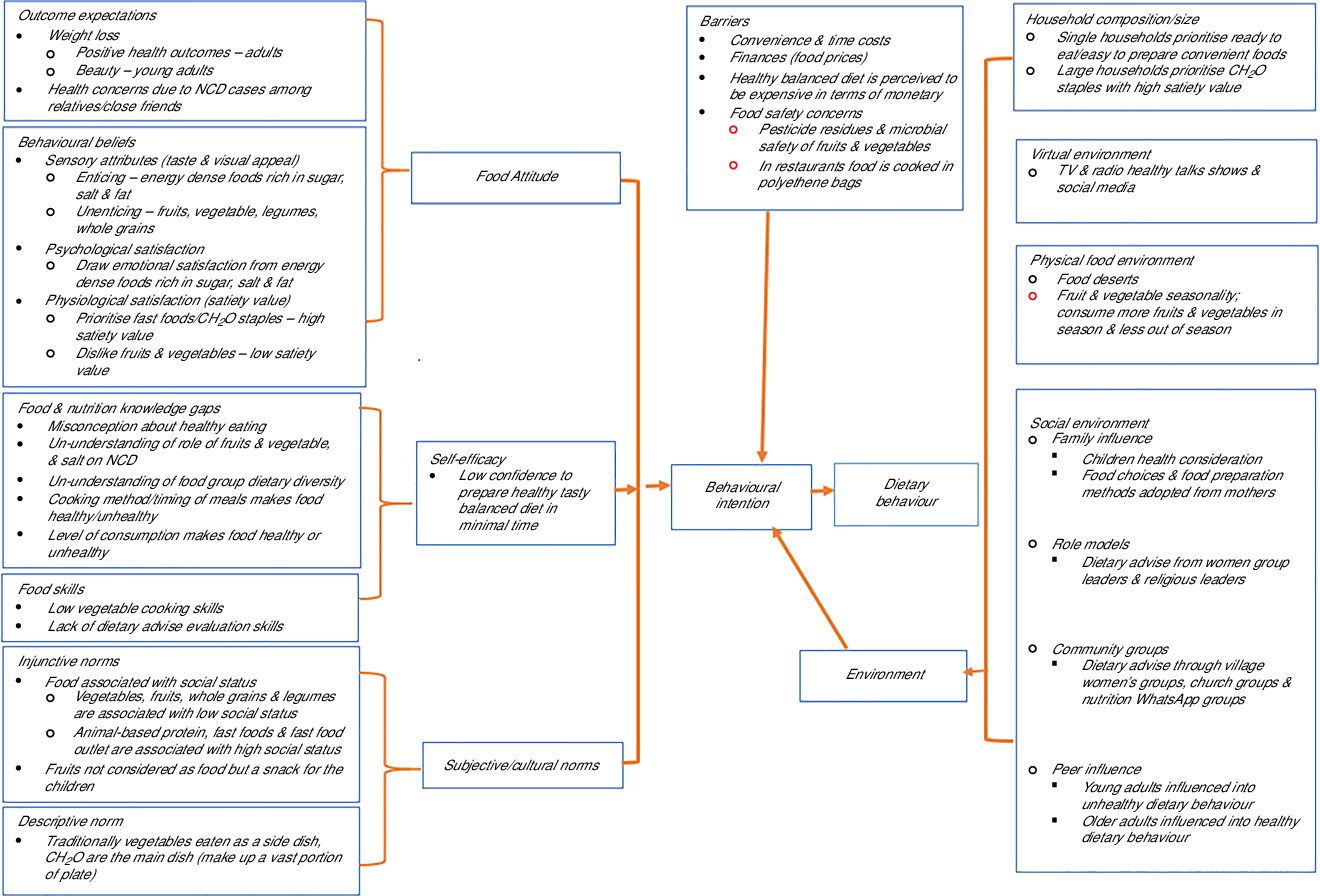
Fig. 2 Determinants of dietary behaviour
Intra-individual factors
Barriers
Convenience and time costs
Participants mentioned that during weekdays, they had no time to prepare breakfast and ultimately convenience influenced their food choices. Ease of storage, preparation and accessibility were discussed as attention points. Easily accessible ready-to-eat unhealthy street foods and easy to prepare/store foods like eggs were preferred by especially young adults. Vegetables were regarded as cumbersome to prepare. There are limited quality prepacked vegetable options in markets.
“I have no time, I come back from work and I need to rest, and those vegetables take some time to wash them to make sure that they are clean and cut cutting them, I feel that it is time wasting, I have no time for that” participant in FGD 3.
Financial barriers (price and affordability)
Participants agreed that food choices were planned according to food prices. Amidst a limited budget, considerations are given to affordable foods perceived to have a high satiety value. Such foods include carbohydrate staples mentioned by mostly adults and energy-dense and ready-to-eat street foods cited by young adults.
‘you see you can’t use the money you would have used to buy food that you are buying pineapples’ participant in FGD 6.
However, during discussions, it was evident that a good financial situation does not automatically translate into healthy eating.
Food safety concerns
Participants had concerns about antibiotic residues in milk and chicken and aflatoxins and metal fillings in groundnut powder. Likewise, concerns were raised about hygiene of prepacked and street-vended fresh vegetables and fruits. Furthermore, vegetables were associated with high levels of pesticide residues.
‘the tomatoes, the cabbages, they grow up on pesticides, everything is sprayed with pesticides. yes, even though we would like to eat them but when we think about the pesticides, we leave them’ participants in FGD 6.
Behavioural beliefs
Psychological and physiological satisfaction
Young adults affirmed that food choices are informed by cravings, emotional and physiological satisfaction. Participants considered carbohydrate staples to have high satiety value while vegetables and fruits low satiety value.
‘Others greens they don’t see them as food, for them they like something which will make them full’, participant in FGD 1.
Emotional satisfaction is drawn from foods rich in mostly sugar, salt and fat.
Sensory attributes
Participants discussed that foods considered unhealthy are tasty and visually enticing. On the other hand, foods like whole wheat bread and some vegetables are not tasty and lack visual appeal. Some vegetables like ‘bitter tomatoes’ and Solanum Macrocarpon were cited to be bitter.
‘the unhealthy ones are more tastier ones, that is the thing, and are attractive to look at, if you tell me to look at greens ooh my God’, FGD 3 participant,
Outcome expectations
Adult women discussed limiting sugar and oil consumption to protect themselves against diabetes, heart attack and unhealthy weight gain.
‘I discovered that I had heart problems, so they stopped me taking too much oil,’FGD 4 participant
Young adults discussed moderating oily foods (linked to pimples) and foods perceived to cause weight gain because of negative perception towards weight gain among peers.
‘I used to take soda from Monday to Monday, from morning to evening, I take sodas, so I had started putting on a lot of weight, that everyone is like that is not your size, so I was like, no more sodas’FGD 1 participant
Adverse health effects suffered by a relative or close friend was discussed as a key motivation to change dietary behaviours.
Self-efficacy and food skills
Participants mentioned the understanding of food benefits to be an important booster of their confidence to eat healthy foods previously perceived to be for the poor.
‘But as people continue to learn the benefits of these foods previously associated with poverty, the perception is changing. Because even if you cook your meat and me, I cook my silver fish, I be feeling very comfortable, participant in FGD 6’
It was noted that vegetable cooking skills and meal planning were important determinants of dietary behaviour. Participants observed that people from Northern Uganda paste a range of vegetables in groundnut and sesame sauce and thus have higher vegetable consumption than those from central Uganda, with limited vegetable cooking skills and engage mostly in frying. Preparation of a balanced meal was perceived to be expensive due to the time involved and food and fuel costs. During the discussions, it was observed that the skills to evaluate dietary advice from social networks and other platforms were limited.
Food and Nutrition Knowledge
Participants had limited knowledge on healthy eating and balanced diet. Some participants defined healthy diet as a diet rich in fruits and vegetables and low in oily foods. To others, a healthy diet was interpreted as not using cooking oil and sugar.
‘healthy diet, I think vegetables like Sukuma-wiki, they are good for our health, it is better if you take more vegetables than taking oily foods like meat, chicken’ participant in FGD 3
On the other hand, balanced diet was defined as having a diversity of carbohydrate staples on a plate. Food group dietary diversity knowledge was scanty.
‘you mean, you eat matooke, cassava, posho, Irish and rice. M: no, food groups. R: that is what I have listed’, participant in FGD 5, discussing balanced diet.
Cakes, soda, pizza, sausage, red meat, French fries and deep-fried foods were categorised as unhealthy. These foods were considered to contain too much oil, sugar and artificial colourants. Sugar was linked to type 2 diabetes and cooking oil to heart diseases. However, participants could not make a distinction between healthy cooking oils and unhealthy cooking fats.
‘if you eat foods that contain a lot of sugar, you will be at risk of diabetes, and also oil you be at risk of cardiac arrest’, participant in FGD 3
Fruits, vegetables, legumes, water, homemade juice and boiled foods were categorised as healthy. Though these foods are mentioned as healthy, none of the participants knew the daily recommendations of fruits and vegetables and lacked basic knowledge on prevention roles of fruits and vegetables towards NCD. Benefits of consuming fruits and vegetables were interpreted in terms of improving mainly blood levels and immunity.
Social-cultural norms
Injunctive norms
Vegetables, whole grains and legumes are foods for the poor, while animal-based protein, fast foods and eating at fast-food outlets are accorded a high social status. Fruits are not considered as food but a snack for children.
‘like what H said, like the vegetables people think it is for the poor and then the fruits we think they are for children’, participant in FGD 4
Descriptive norms
Participants concurred that carbohydrate staples are the main traditional dish and make up a vast portion of the plate. Vegetables are eaten as a side dish.
‘we believe that in our diet, like in a meal, that veg should be the least, even if it is affordable, available in large quantities, we believe that they should be eaten in little amounts, as a side dish’ participant in FGD 1.
Environment-related factors
Social environment
Four components of social environment were discussed to have an influence on dietary behaviours. First level was the family, where dietary choices are hinged on the desire to provide healthy foods to children.
‘I have to plan because I have a daughter, I say okay today we ate beans, may be even tomorrow we shall have beans, so the next day we have to change, so that she gets used to every type of food’FGD 1 participant.
Young adults living with parents mentioned that food choices were decisions of their mothers. Adults and young adults living independently mentioned that their food preparation methods and choices were adopted from the mothers. Second, religious and women group leaders were presented as role models with regard to providing healthy dietary advice. Third, it was observed that community groups that included village and church small groups played an important role in dietary counsel. Some participants were part of nutrition WhatsApp groups formed on the basis of promoting healthy lifestyles.
‘We also have a community health worker in our group, she usually brings for us education sessions on how to eat, she goes a lot for these education sessions and what she learns she brings them back to us’, FGD 6 participants.
The fourth level was the peer influence. Direction on dietary influence was dependent on age category. Young adults were influenced into unhealthy dietary behaviours while adults into healthy options.
Physical food environment
An abundance of cheap processed and street foods rich in salt, fat and sugar was noted. It was observed that local restaurants and street eat outs with healthy food offers (boiled foods and vegetables) are scarce in Kampala.
‘Chicken and chips are in plenty – all streets, everywhere, any time and, soda and juice are in plenty’.‘We would love to have vegetables but most of us eat outside homes. They normally serve a very small portion and you can’t go behind the kitchen to ask for more’, participants in FGD 1& 4.
Fruits and vegetables are accessed through mostly traditional markets. However, some of these markets are occasional, occurring once in a week, and those which are permanent are far away from residential areas.
‘I like greens but because of where I live, they are not easily available, unless I have to go to the market every day to get them, so because of that I rarely eat them’, participant in FGD 6.
Seasonality, compared with other food groups, fruits and vegetable intake is highly dependent on season; consumption is higher in season. Out of season fruits are expensive and scarce.
Virtual environment
Social media and mainstream media (health talks on TV and radio) were reported as important sources of dietary advice. Some participants belong to nutrition WhatsApp groups (platforms formed with an objective of sharing dietary advice), and they highly trust information shared in these groups.
Determinants of physical activity behaviour
Eighteen factors organised under eleven themes were identified to have an influence on physical activity behaviour, Fig. 3.
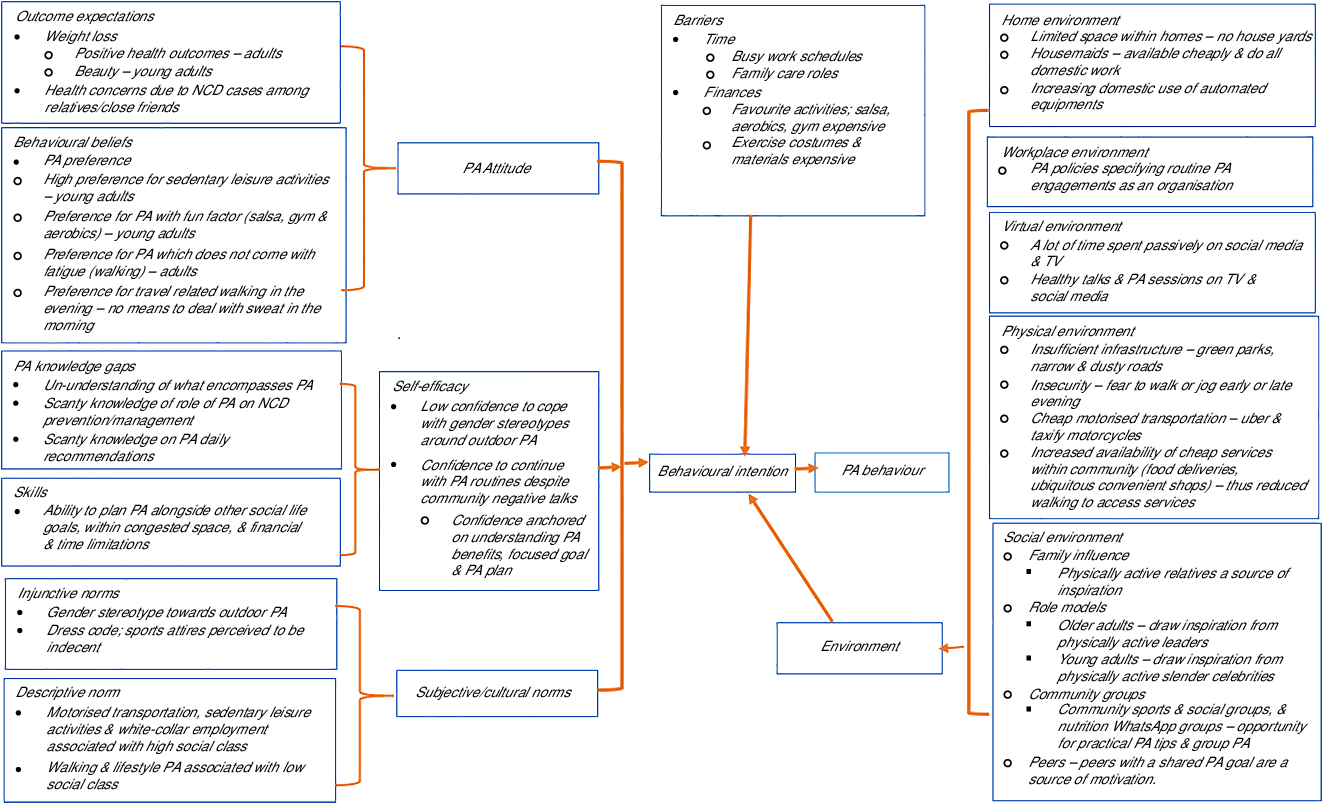
Fig. 3 Determinants of physical activity behaviour
Intra-individual determinants
Barriers
Time and financial barriers
All participants agreed that busy work schedules and mothers’ role in the family leave them with limited time to engage in physical activity. Young adults mentioned limited finances as a barrier. They discussed that engaging in salsa, gym and aerobics was expensive and yet these activities are favourite types of physical activity. In addition, they decried the high cost of exercise outfits and materials.
‘yes, there is some other hinderance, for example when you’re interested in aerobics, but those aerobics places are for paying, so you be not having money and you love aerobics, you will just end up not going’, participant in FGD 7
Behavioural beliefs
Preference
Has an influence on physical activity and varies with age. During leisure time, young adults prefer sedentary activities (watching movies) and physical activity that comes with a fun factor, dancing, salsa and aerobics. Adults declared to enjoy activities like walking which do not come with fatigue. However, preference was dependent on the time of the day. They did not support walk to work during the morning hours due to lack of means of dealing with sweat. Evening walks are generally preferred to morning walk.
Outcome expectations
Positive health outcomes and weight loss for beauty are important push factors to participate in physical activity. Adults discussed that they engage in physical activity not because they like it but because it is a treatment for their health conditions. Particularly, adverse health effects suffered by a relative or close friend is a catalyst for individuals to engage in physical activity.
‘I developed pressure like 3 years ago. when I went to a doctor, he advised me to do exercises, so I decided to do some exercises at home like in the morning I skip the rope, I jump, stretch the body’, participant in FGD 11.
For young adults, the main goal for engaging in physical activity was driven by the benefits of remaining slender, an attribute they associated with beauty.
‘For exercises, I do not like them, but also for my body, I don’t want to find I have a funny body, you know, so it forces me to do some exercises’, participant in FGD 8
Skills and Self-efficacy
Participants reported low confidence to engage in outdoor activities after being ridiculed by the community for involvement in physical activities perceived to be unfeminine. However, some women possess confidence to continue with their physical activity routines despite negative reproach. Confidence was anchored on understanding the benefits of physical activity, having a focused goal and a plan of how to achieve it.
‘I may even have money, but I will decide to walk to Bugolobi, because it is me. I know the benefits, Iam the one who benefits, not the person looking at me’, participant in FGD 8
Physical activity knowledge
Inconsistency was observed on understanding what encompasses physical activity. According to some participants, physical activity is different from exercise and encompass mainly domestic/routine daily activities. To others, physical activity meant exercise. Participants had a perception that structured physical activity has more health benefits compared with lifestyle physical activity. Generally, participants were unable to distinguish between lifestyle physical activity (activities usually part of one’s daily routine) and structured fitness physical activity (exercise). Knowledge on the role of physical activity towards NCD prevention and daily recommended levels of physical activity was limited. Participants consistently discussed physical activity benefits in terms of stress relief, body cleansing and weight management, with fewer mentions of NCD prevention/management.
‘it increases your immunity, burns fats, relaxes your mind, you sleep well, you reduce your weight’ Participant in FGD 8
Socio-cultural norms
Traditionally, outdoor physical activity (playing football, jogging and biking) is perceived to be unfeminine.
‘there are some types of exercises that the society would not be comfortable with, for us as women seeing us do. because like for us, those days if a girl got a bicycle to ride, that was next to an abomination. Yeah also like playing football however much you are a lady and would like to play football in Buganda people are not well with it, they can see it as if you are bi-sexual’, FGD 12, participant.
Walking and lifestyle physical activity like digging and cleaning are associated with low social class, while sedentary office work and motorised transportation are a sign of good socio-economic conditions.
‘Even walking, they be saying, that one just walks, she cannot even afford money for transport. she walks Banda to Nakawa, every day, she is so bad off, very poor’, participant in FGD 7.
Furthermore, there is a perception that exercise is for the rich, those who are fat or idle. Exercise dress code also has an influence on physical activity; costumes (tight and short) are observed as a sign of indecency.
‘now you see, I may put on my panties and would like to jog but whenever you pass, people be shouting at you. So, the following day you can’t do it again’, participant in FGD 11.
Environment-related factors
Social environment
Four levels of social environment were discussed to influence physical activity. The first level was the family network; physical activities are planned and undertaken with partners while physically active relatives are source of inspiration.
‘for example, her sister encourages them, mostly as G said if you have the pushing factor it encourages you, so even if you feel it, even if you do not, you have to. Because you have someone pushing and someone you can do it with’, participant in FGD 8.
Second, membership in a social/community sports group or WhatsApp group formed with an objective of living an active lifestyle was discussed as an opportunity to get practical physical activity tips. Participants agreed that beneficial groups have members with similar goals.
‘We have a netball team, at-times we even go for competitions. But even if I find those playing, even if they are young girls, I also join them and play. But my aim is to exercise my body’, participant in FGD 11.
Peers and role models were the third and fourth levels that influence physical activity. Peers were discussed as a source of demotivation. Only peers with shared goals are a source of motivation. Regarding role models, young adults discussed to follow physical activity lifestyles of good looking (nicely shaped slender bodies) women celebrities, while adults draw inspiration from physically active leaders.
‘I normally get this information from people, especially those ladies who aim to have good looking figures, they say when you exercise you be having small belly, you don’t easily get fat’ participant in FGD 7.
Physical environment
Congestion, insufficient infrastructure, insecurity, increased motorised transportation and improved services were described to be central determinants of physical activity. Recent improvements in motorcycle transportation (Uber and Safe-boda apps) have contributed to increased access to cheap and safe travels.
‘Right now, boda-boda, they have brought the app, a boda-boda picks you from home, drops you where exactly you want to go and from there you walk just two steps and you are inside where you are going and at a cheaper cost’. Participant in FGD 8
In terms of infrastructure, participants complained of narrow and dusty roads and lack of green parks for outdoor physical activity. On insecurity, members concurred that the high crime rate hindered walking or jogging in the early morning or late evening. In addition, participants raised concern on increased availability of services like food deliveries at home/workplaces and ubiquitous convenient shops. These services negatively impact on physical activity, as people no longer walk or walk for very short distance to access services.
‘services these days are really always available. Now you can imagine people working in arcades. when it is midday people are passing by, do you need food, do you need this, instead of someone getting out of their office’ Participant in FGD 8.
Home environment
Involvement of housemaids in chores, limited home space and increased use of domestic automated equipment negatively affects physical activity. It was noted that housewives no longer engage in domestic work because of hired housemaids. Additionally, most residences are in single rooms without yards to engage in physical activity.
‘And another thing is your home where you stay you may not have space, for example one may be sleeping in one room and outside there is no space, yet she sleeps in the room with other people. And she has no place where she can do some exercises from’, participant in FGD 11.
Virtual environment
The virtual environment had both negative and positive effects on physical activity. On a negative note, participants spent much of their time passive on social media and TV that limit involvement in physical activities.
‘people spend a lot of time on social media like J said, that you can’t tell a person about your jogging, when there is a trending video on you-tube’, participant in FGD 10.
On a positive note, some members mentioned that TV and social media was a source of physical activity information. They get physical activity tips from instructors on regular TV programmes. Some participants were part of physical activity WhatsApp groups where they share practical tips and planned group activities. However, in general, information on physical activity is still scanty and difficult to find.
‘that information is not so common that you’re going to find it somewhere. Sometimes maybe you get on TV, when they are some teachings about PA, on radios. I think like that, but it is very difficult to find’, FGD 10, participant.
Workplace environment
Participants within the formal sector reported workplace policies specifying routine physical activity engagements as an organisation. Some adopted these physical activity routines outside their workplace environment.
Discussion
Dietary and physical activity behaviours are determined by intra-individual, socio-cultural and environmental interrelated factors. The findings are peculiar to WRA as defined in the current study. The study identified twenty-one factors influencing dietary behaviour of which eighteen were in line with findings from other settings across urban SSA(Reference Yiga, Seghers and Ogwok21,Reference Gissing, Pradeilles and Osei-Kwasi39) . One of the factors (negative perception towards overweight) was divergent from previous findings across urban SSA, while two determinants food safety concerns and social media are new additions in urban SSA. For physical activity, fourteen of the eighteen determinants were comparable with previous findings across urban SSA(Reference Yiga, Seghers and Ogwok21). Five determinants like social media, limited space within homes, physical activity planning skills, physical activity preferences and increased availability of cheap services are new additions to evidence base within urban SSA. Weight loss was an important motivation for physical activity which contravenes previous findings across urban SSA that reported a positive perception towards overweight.
Participants acknowledged high consumption of carbohydrate staples and low consumption of fruits and vegetables. This is consistent with findings from West and South African communities(Reference Everett-Murphy, De Villiers and Ketterer18,Reference Boatemaa, Badasu and De-Graft Aikins40–Reference Hiamey, Amuquandoh and Boison42) . The observed dietary behaviours in urban Uganda could be linked to food and nutrition knowledge gaps, cultural misconceptions and negative behaviour beliefs (sensory and satiety value perceptions)(Reference Vidgen and Gallegos43–Reference Scripa45). On a positive note, during discussions, it was noted that as people learn about the benefits of fruits, vegetables and legumes then cultural misconceptions and negative behavioural beliefs on these foods start to change.
Food safety concerns, particularly pesticide residues, deter participants from eating adequate fruits and vegetables. This perception has been confirmed by data that fresh produce in Uganda contain high levels of pesticide residues(Reference Kaye, Nyombi and Mutambuze46,Reference Atuhaire, Kaye and Mutambuze47) . Participants noted that over the last decade, Kampala has increasingly become a food desert. Fruits and vegetables are accessible in mainly traditional markets that are generally far away from residences. Across urban SSA, similar findings have been reported(Reference Hiamey, Amuquandoh and Boison42,Reference Aryeetey, Oltmans and Owusu48–Reference Steyn and McHiza50) . The 2018 global nutrition report shows a 16 % increase in per capita consumption of packaged energy dense ready-to-eat foods in Africa between 2005 and 2015(51). However, in South Africa, a substantial proportion of consumed energy dense ready-to-eat foods in urban areas comes in the form of undocumented unpackaged street vended foods(Reference Micklesfield, Lambert and Hume52).Convenience and time costs are important determinants of food choices due to the increasing number of working women in urban Uganda. Accordingly, participants discussed their dietary choices to be skewed towards the easily accessible ready-to-eat foods. Vegetable consumption is further hampered by lack of quality prepacked vegetables. Besides the convenience, energy dense foods are perceived to offer emotional satisfaction owing to their perceived superior sensory attributes. These findings reinforce the latest recommendations by Perry(Reference Perry, Samra and Edmonstone53) and Vidgen(Reference Vidgen and Gallegos43) that healthy food decisions need not only consider nutrition but also gastronomic needs and available resources especially time and money.
Social and virtual environment emerged as important dietary behaviour determinants. In line with findings from urban settings in West and South Africa, cooking methods and dietary patterns are adopted from mainly mothers(Reference Phillips, Comeau and Pisa17–Reference Van, Riet, Den Hartog and Mwangi20). In addition, community groups (village- and religious-based women groups) are vital sources of dietary information. Notable finding was the existence of social media groups (WhatsApp and Facebook) solely formed with a goal of sharing dietary advice to achieve healthy dietary lifestyles. Evidence from high-income countries depicts social media platforms to be important platforms for nutrition information sharing and social support particularly among young adults(Reference Klassen, Douglass and Brennan54).
Divergent from previous studies in urban SSA(Reference Phillips, Comeau and Pisa17,Reference Kiawi, Edwards and Shu41,Reference Stern, Puoane and Tsolekile55) , we found a negative perception towards overweight. Young adults related slender body to beauty while older adults related overweight to health risks. Hence, weight management was an important consideration in dietary choices. Evidence shows that as societies modernise, cultures change and adapt slender body ideals(Reference Swami56).
Gender stereotypes influenced structural physical activity which is consistent with findings from other parts of Africa(Reference Phillips, Comeau and Pisa17,Reference Walter and Du Rosa57) . Traditionally, women are ridiculed when involved in activities like football, jogging and biking. Accordingly, many women lack the self-efficacy to engage in sports. This could be linked to knowledge gaps of what encompasses physical activity and its health benefits(Reference Phillips, Comeau and Pisa17,Reference Kiawi, Edwards and Shu41,Reference Stern, Puoane and Tsolekile55,Reference Walter and Du Rosa57) . In the current study, understanding of physical activity benefits was discussed to increase self-efficacy to overcome physical activity cultural misconceptions. Women who receive social support from community, family, friends and role models are the most successful at incorporating a regular routine of physical activity into their life(Reference Seghers, Van Hoecke and Schotte29,Reference Stern, Puoane and Tsolekile55,Reference Adeniyi, Ogwumike and Bamikefa58–Reference Coakley62) .Social support may be in form of verbal encouragement or companionship during exercise. In South Africa, amateur community sports teams have been suggested as important initiatives to engage women in physical activity(Reference Phillips, Comeau and Pisa17). In Belgium(Reference Seghers, Van Hoecke and Schotte29) and Barbados(Reference Alvarado, Murphy and Guell60), social physical activity groups have been observed to enact sustained physical activity routines. In this study, participants emphasised that peers with a shared physical activity plan are a source of support and motivation.
Limited space, automation of domestic activities and sedentary indoor entertainment in home environment emerged as a constraining factor to physical activity among WRA. Sedentary home environment has been reported in developed countries(Reference Owen, Healy and Matthews63), signifying physical activity transition from active to sedentary home environments in urban Uganda. Physical activity transition has also been reported in urban Kenya(Reference Katzmarzyk and Mason64,Reference Larouche, Oyeyemi and Prista65) .
Implication for health promotion policies and programming
Topical systematic reviews have highlighted a need for rigorous qualitative studies to understand the determinants of dietary and physical activity behaviours in urban Uganda(Reference Yiga, Seghers and Ogwok21,Reference Gissing, Pradeilles and Osei-Kwasi39) . This study highlights potential determinants amenable to change through policy and programming. A set of determinants, namely, limited time due to increasing employment opportunities for women, low self-efficacy, cultural misconceptions, preference for slender body sizes, social media and community social support cut across physical activity and dietary behaviours. Interventions combining dietary and physical activity behaviours have been demonstrated to be effective at alleviating overweight and obesity(Reference Andrade, Lachat and Cardon66).The commonality in determinants presents an opportunity to design health promotion strategies combining dietary and physical activity behaviours in urban Uganda. For example, preference for slender body sizes could be an opportunity to encourage adoption of healthy lifestyles by emphasising the importance of the compounded effect of dietary and physical activity towards weight management, but attention has to be paid to avoidance of eating disorders. Time limitations call for strategies that can enhance women’s skill and self-efficacy to develop convenient physical activity and healthy dietary plans(Reference Chatzisarantis, Frederick and Biddle67). However, planning necessitates knowledge, skills and a good understanding of health recommendations and available opportunities(Reference Chatzisarantis, Frederick and Biddle67).Contextualised food-based dietary and physical activity guidelines in urban areas in Uganda could potentially address the existing gaps in knowledge and skills, cultural misconceptions and behavioural beliefs while looking for social support as a leverage(Reference Vidgen and Gallegos43,Reference Perry, Samra and Edmonstone53) . Physical activity guidelines need to detail the different types of physical activity, health benefits and practical tips regarding intensity and duration of physical activity options. Furthermore, socialisation through community groups and role models could be a potential strategy to address the cultural misconceptions. A potential mode of delivery is the use of social media, however, taking into account the nonfactual nutrition information shared on these platforms. Therefore, as recommended by Vidgen(Reference Vidgen and Gallegos43), there is a need to equip the general population with skills to evaluate and distinguish evidence based from nonfactual information. Home gardens could be an explored to address fruit and vegetable accessibility gaps in urban Uganda.
Study strengths and limitations
The FGD questioning route design was based on modified theoretical framework encompassing five theories previously used to study dietary and physical activity behaviours in other settings. Theoretical frameworks need cultural and local setting adaptations to capture the relevant details(Reference Eldredge, Markham and Ruiter16,Reference Glanz, Rimer and Viswanath68) . Our aim was to capture relevant details to aid designing of tailored interventions to counter nutrition transition in urban Uganda. Based on our systematic review across urban SSA(Reference Yiga, Seghers and Ogwok21), we needed an adapted theoretical framework to capture relevant details. However, questions may arise on the validity of adapted framework. In our view, adapting a theoretical framework presents no methodological flaws as theoretical frameworks are not golden standards but rather guiding tools to obtain relevant information. Combining health behaviour theories to understand behaviour is emphasised by health promotion protocols as no single theory can describe behaviour in its entirety(Reference Eldredge, Markham and Ruiter16,Reference Glanz, Rimer and Viswanath68) . Overall, using an adapted theoretical framework enabled us to get an understanding of dietary and physical activity behaviours in urban Uganda’s setting. Using a questioning route rather than a topic guide could have obstructed all major themes to emerge from the FGD. However, this was minimised as our questioning route included probes to allow interviewer flexibility to explore emerging themes. This approach is described in the guidelines for designing FGD guides(Reference Hennink69). Our recruitment and study approach enabled us to capture age-related differences, giving an insight into the need for age-specific intervention strategy. However, recruitment centres were Christian-based organisations; thus, it is possible that we could have obtained results with a Christian religious bias.
Conclusion
Dietary and physical activity behaviours among WRA in urban Uganda are shaped by an intertwined array of vast contextual beliefs at intra-individual, socio-cultural and environmental levels. A set of determinants cut across physical activity and dietary behaviours. The commonality in determinants presents an opportunity to design health promotion policy and intervention strategies combining dietary and physical activity behaviours in urban Uganda. Combined healthy dietary and physical activity behaviours are shown to confer positive synergistic effect towards metabolic health. Generally, available insights suggest a need for comprehensive interventions that could address socio-cultural misconceptions, financial and time limitations through bridging gaps in knowledge, skills and self-efficacy.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
Acknowledgements: The authors acknowledge John Mungereza, Paulino Twesigye Mondo and Francesca Ihongoyi Kimwama of Our Lady of Africa, Mbuya (Uganda), Stella Azamadia of Beauty for Ashes (BFA) and Nakawesa Stella of Kiyaga Village Savings Loan Association (Uganda) for their assistance in the community. The authors are also grateful to the participants for volunteering to take part in the study. Financial support: The research was funded by the Belgian Directorate General for Development Cooperation and Humanitarian Aid (DGD), an initiative implemented by VLIR-UOS.The funder had no role in designing of the study, data collection, analysis, interpretation and writing of the manuscript. Conflict of interest: None. Authorship: P.Y., C.M., P.O. and J.S. designed the study. P.Y., J.A. and M.D.A. conducted the FGD. P.Y., J.A., M.D.A. and C.M. analysed the data. P.Y. wrote the first draft of the manuscript, while C.M., P.O. and J.S. critically reviewed and improved the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by Human Research Ethics committee of Clarke International University (reference number IHSU-REC/0117) and Uganda National Council for Science and Technology (reference number HS290ES). Participants signed a written informed consent for their participation in the study.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020003432






