
331 results
Peer review of clinical and translational research manuscripts: Perspectives from statistical collaborators
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 04 January 2024, e20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Apples to advocacy: Evaluating consumer preferences for hard cider policies
-
- Journal:
- Journal of Wine Economics / Volume 18 / Issue 4 / November 2023
- Published online by Cambridge University Press:
- 28 November 2023, pp. 286-301
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Creating an electronic antibiogram using visualization software: Easily updatable and removes the need for yearly manual review
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s34
-
- Article
-
- You have access
- Open access
- Export citation
-
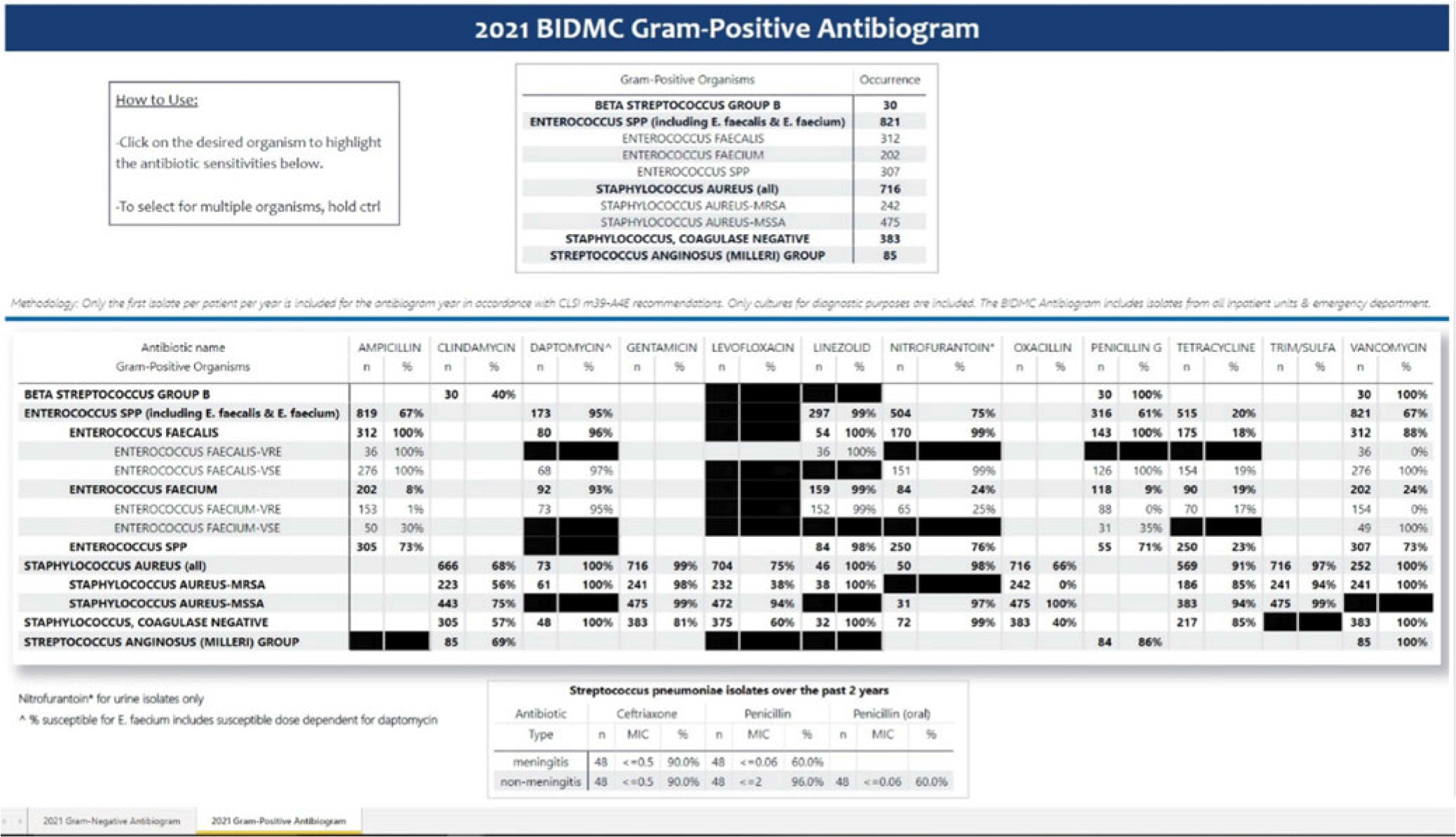
Background: Previously, our hospital manually built a static antibiogram from a surveillance system (VigiLanz) culture report. In 2019, a collaboration between the antimicrobial stewardship team (AST) and the infection control (IC) team set out to leverage data automation to create a dynamic antibiogram. The goal for the antibiogram was the ability to easily distribute and update for hospital staff, with the added ability to perform advanced tracking and surveillance of organism and drug susceptibilities for AST and IC. By having a readily available, accurate, and Clinical and Laboratory Standards Institute (CLSI)–compliant antibiogram, clinicians have the best available data on which to base their empiric antibiotic decisions. Methods: First, assessment of required access to hospital databases and selection of a visualization software (MS Power BI) was performed. Connecting SQL database feeds to Power BI enabled creation of a data model using DAX and M code to comply with the CLSI, generating the first isolate per patient per year. Once a visual antibiogram was created, it was validated against compiled antibiograms using data from the microbiology laboratory middleware (bioMerieux, Observa Integrated Data Management Software). This validation process uncovered some discrepancies between the 2 reference reports due to cascade reporting of susceptibilities. The Observa-derived data were used as the source of truth. The antibiogram prototype was presented to AST/IC members, microbiology laboratory leadership, and other stakeholders to assess functionality. Results: Following feedback and revisions by stakeholders, the new antibiogram was published on a hospital-wide digital platform (Fig. 1). Clinicians may view the antibiogram at any time on desktops from a firewall (or password)–protected intranet. The antibiogram view defaults to the current calendar year and users may interact with the antibiogram rows and columns without disrupting the integrity of the background databases or codes. Each year, simple refreshing of the Power BI antibiogram and changing of the calendar year allows us to easily and accurately update the antibiogram on the hospital-wide digital platform. Conclusions: This interdisciplinary collaboration resulted in a new dynamic, CLSI-compliant antibiogram with improved usability, increased visibility, and straightforward updating. In the future, a mobile version of the antibiogram may further enhance accessibility, bring more useful information to providers, and optimize AST/IC guidelines and education.
Disclosures: None

Description of Patients with Out-of-Hospital Cardiac Arrest within 24 Hours of EMS Transport Refusal.
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, p. s106
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
The Virtues of Interpretable Medical AI
-
- Journal:
- Cambridge Quarterly of Healthcare Ethics , First View
- Published online by Cambridge University Press:
- 10 January 2023, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antidepressant medications in dementia: evidence and potential mechanisms of treatment-resistance
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 3 / February 2023
- Published online by Cambridge University Press:
- 09 January 2023, pp. 654-667
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Virtues of Interpretable Medical Artificial Intelligence
-
- Journal:
- Cambridge Quarterly of Healthcare Ethics , First View
- Published online by Cambridge University Press:
- 16 December 2022, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Occurrence of baleen whales in the New York Bight, 1998–2017: insights from opportunistic data
-
- Journal:
- Journal of the Marine Biological Association of the United Kingdom / Volume 102 / Issue 6 / September 2022
- Published online by Cambridge University Press:
- 02 November 2022, pp. 438-444
-
- Article
- Export citation
Radar attenuation demonstrates advective cooling in the Siple Coast ice streams
-
- Journal:
- Journal of Glaciology / Volume 69 / Issue 275 / June 2023
- Published online by Cambridge University Press:
- 11 October 2022, pp. 566-576
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cost-effectiveness of mirtazapine for agitated behaviors in dementia: findings from a randomized controlled trial
-
- Journal:
- International Psychogeriatrics / Volume 34 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 19 July 2022, pp. 905-917
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of a model to predict antidepressant treatment response for depression among Veterans
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 11 / August 2023
- Published online by Cambridge University Press:
- 15 July 2022, pp. 5001-5011
-
- Article
- Export citation
Suicidal ideation in dementia: associations with neuropsychiatric symptoms and subtype diagnosis
-
- Journal:
- International Psychogeriatrics / Volume 34 / Issue 4 / April 2022
- Published online by Cambridge University Press:
- 25 March 2022, pp. 399-406
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Birth without intervention in women with severe mental illness: cohort study
-
- Journal:
- BJPsych Open / Volume 8 / Issue 2 / March 2022
- Published online by Cambridge University Press:
- 24 February 2022, e50
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of a model to predict psychotherapy response for depression among Veterans
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 8 / June 2023
- Published online by Cambridge University Press:
- 11 February 2022, pp. 3591-3600
-
- Article
- Export citation
Poor outcomes in both infection and colonization with carbapenem-resistant Enterobacterales
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 02 February 2022, pp. 1840-1846
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The baby and the bathwater: On the need for substantive–methodological synergy in organizational research
-
- Journal:
- Industrial and Organizational Psychology / Volume 14 / Issue 4 / December 2021
- Published online by Cambridge University Press:
- 14 December 2021, pp. 497-504
-
- Article
- Export citation
Characterisation of age and polarity at onset in bipolar disorder
-
- Journal:
- The British Journal of Psychiatry / Volume 219 / Issue 6 / December 2021
- Published online by Cambridge University Press:
- 25 August 2021, pp. 659-669
- Print publication:
- December 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trajectories of psychological distress among individuals exposed to the 9/11 World Trade Center disaster
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 14 / October 2022
- Published online by Cambridge University Press:
- 07 April 2021, pp. 2950-2961
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
60941 Vaginal pH predicts cervical intraepithelial neoplasia-2 regression in women living with human immunodeficiency virus
-
- Journal:
- Journal of Clinical and Translational Science / Volume 5 / Issue s1 / March 2021
- Published online by Cambridge University Press:
- 30 March 2021, pp. 23-24
-
- Article
-
- You have access
- Open access
- Export citation
Klaus Bergmann, MD, FRCPsych
-
- Journal:
- BJPsych Bulletin / Volume 45 / Issue 4 / August 2021
- Published online by Cambridge University Press:
- 26 February 2021, pp. 251-252
- Print publication:
- August 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
