
52 results
Large-scale circulation reversals explained by pendulum correspondence
-
- Journal:
- Journal of Fluid Mechanics / Volume 993 / 25 August 2024
- Published online by Cambridge University Press:
- 13 September 2024, A3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We introduce a low-order dynamical system to describe thermal convection in an annular domain. The model derives systematically from a Fourier–Laurent truncation of the governing Navier–Stokes Boussinesq equations and accounts for spatial dependence of the flow and temperature fields. Comparison with fully resolved direct numerical simulations (DNS) shows that the model captures parameter bifurcations and reversals of the large-scale circulation (LSC), including states of (i) steady circulating flow, (ii) chaotic LSC reversals and (iii) periodic LSC reversals. Casting the system in terms of the fluid's angular momentum and centre of mass (CoM) reveals equivalence to a damped pendulum with forcing that raises the CoM above the fulcrum. This formulation offers a transparent mechanism for LSC reversals, namely the inertial overshoot of a forced pendulum, and it yields an explicit formula for the frequency
 $f^*$ of regular LSC reversals in the high-Rayleigh-number (Ra) limit. This formula is shown to be in excellent agreement with DNS and produces the scaling law
$f^*$ of regular LSC reversals in the high-Rayleigh-number (Ra) limit. This formula is shown to be in excellent agreement with DNS and produces the scaling law  $f^* \sim {Ra}^{0.5}$.
$f^* \sim {Ra}^{0.5}$.


Predicting convection configurations in coupled fluid–porous systems
-
- Journal:
- Journal of Fluid Mechanics / Volume 953 / 25 December 2022
- Published online by Cambridge University Press:
- 09 December 2022, A23
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization – ERRATUM
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 07 October 2022, e166
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s78-s79
-
- Article
-
- You have access
- Open access
- Export citation
-
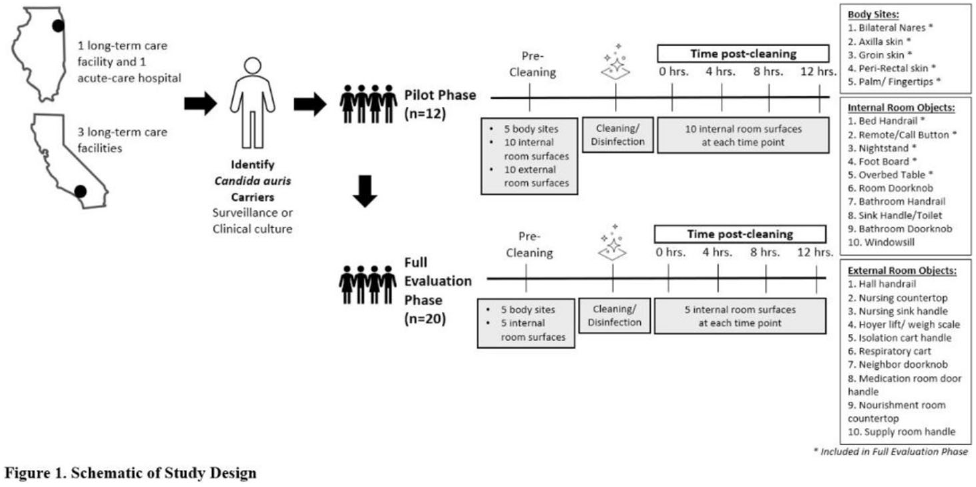
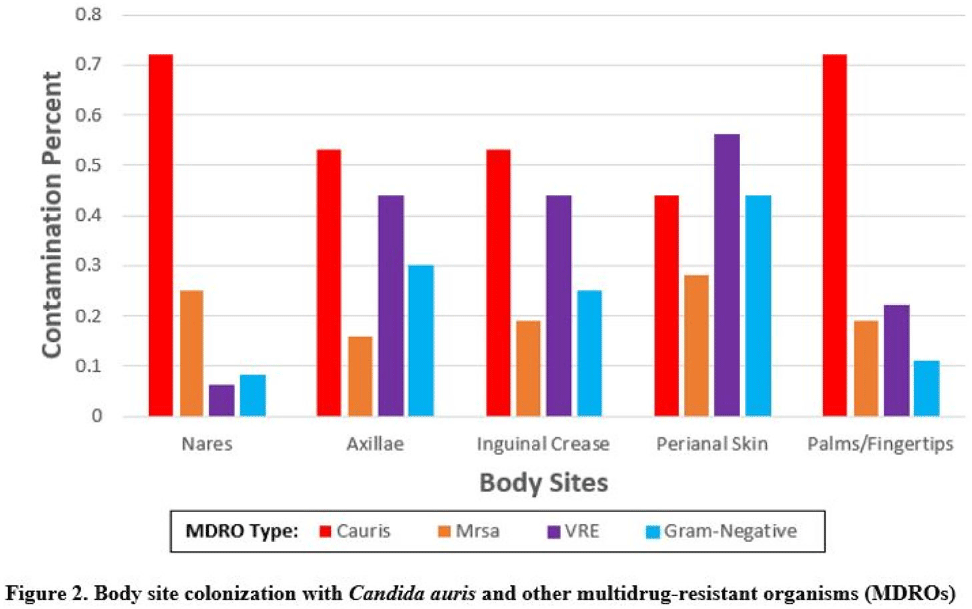
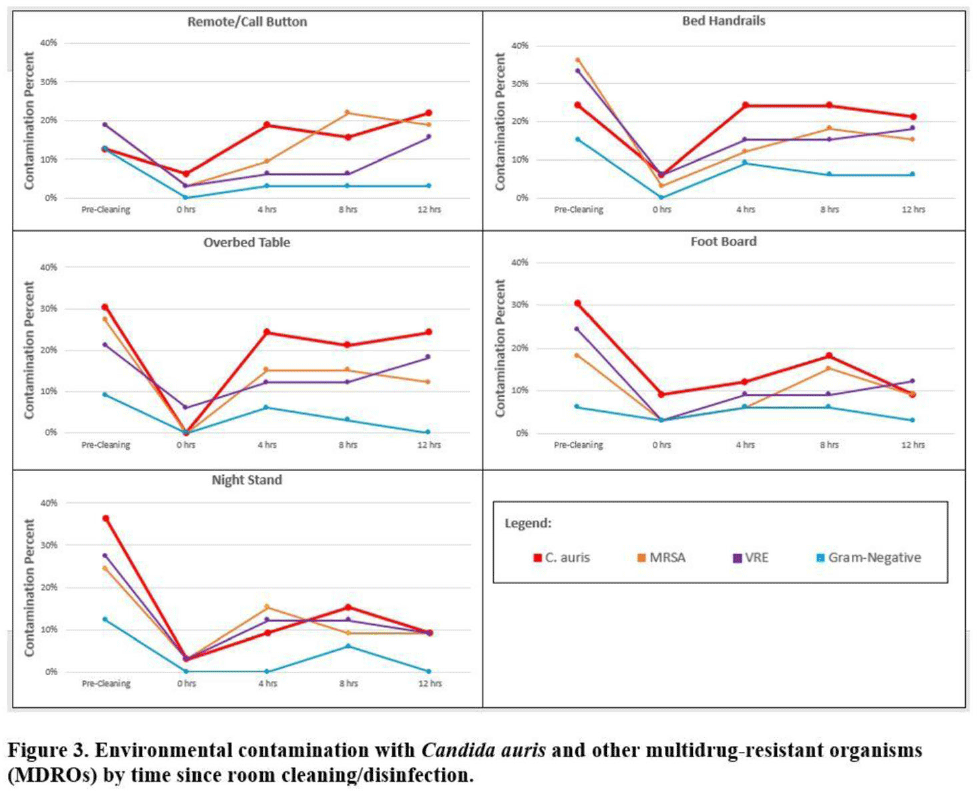
Background:Candida auris is an emerging multidrug-resistant yeast that is transmitted in healthcare facilities and is associated with substantial morbidity and mortality. Environmental contamination is suspected to play an important role in transmission but additional information is needed to inform environmental cleaning recommendations to prevent spread. Methods: We conducted a multiregional (Chicago, IL; Irvine, CA) prospective study of environmental contamination associated with C. auris colonization of patients and residents of 4 long-term care facilities and 1 acute-care hospital. Participants were identified by screening or clinical cultures. Samples were collected from participants’ body sites (eg, nares, axillae, inguinal creases, palms and fingertips, and perianal skin) and their environment before room cleaning. Daily room cleaning and disinfection by facility environmental service workers was followed by targeted cleaning of high-touch surfaces by research staff using hydrogen peroxide wipes (see EPA-approved product for C. auris, List P). Samples were collected immediately after cleaning from high-touch surfaces and repeated at 4-hour intervals up to 12 hours. A pilot phase (n = 12 patients) was conducted to identify the value of testing specific high-touch surfaces to assess environmental contamination. High-yield surfaces were included in the full evaluation phase (n = 20 patients) (Fig. 1). Samples were submitted for semiquantitative culture of C. auris and other multidrug-resistant organisms (MDROs) including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), extended-spectrum β-lactamase–producing Enterobacterales (ESBLs), and carbapenem-resistant Enterobacterales (CRE). Times to room surface contamination with C. auris and other MDROs after effective cleaning were analyzed. Results:Candida auris colonization was most frequently detected in the nares (72%) and palms and fingertips (72%). Cocolonization of body sites with other MDROs was common (Fig. 2). Surfaces located close to the patient were commonly recontaminated with C. auris by 4 hours after cleaning, including the overbed table (24%), bed handrail (24%), and TV remote or call button (19%). Environmental cocontamination was more common with resistant gram-positive organisms (MRSA and, VRE) than resistant gram-negative organisms (Fig. 3). C. auris was rarely detected on surfaces located outside a patient’s room (1 of 120 swabs; <1%). Conclusions: Environmental surfaces near C. auris–colonized patients were rapidly recontaminated after cleaning and disinfection. Cocolonization of skin and environment with other MDROs was common, with resistant gram-positive organisms predominating over gram-negative organisms on environmental surfaces. Limitations include lack of organism sequencing or typing to confirm environmental contamination was from the room resident. Rapid recontamination of environmental surfaces after manual cleaning and disinfection suggests that alternate mitigation strategies should be evaluated.
Funding: None
Disclosures: None



Genomic investigation to identify the source of SARS-CoV-2 infection among healthcare personnel
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s74-s75
-
- Article
-
- You have access
- Open access
- Export citation
-
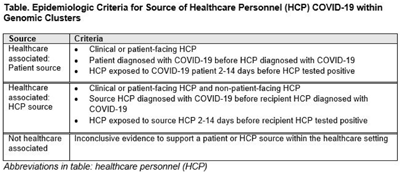
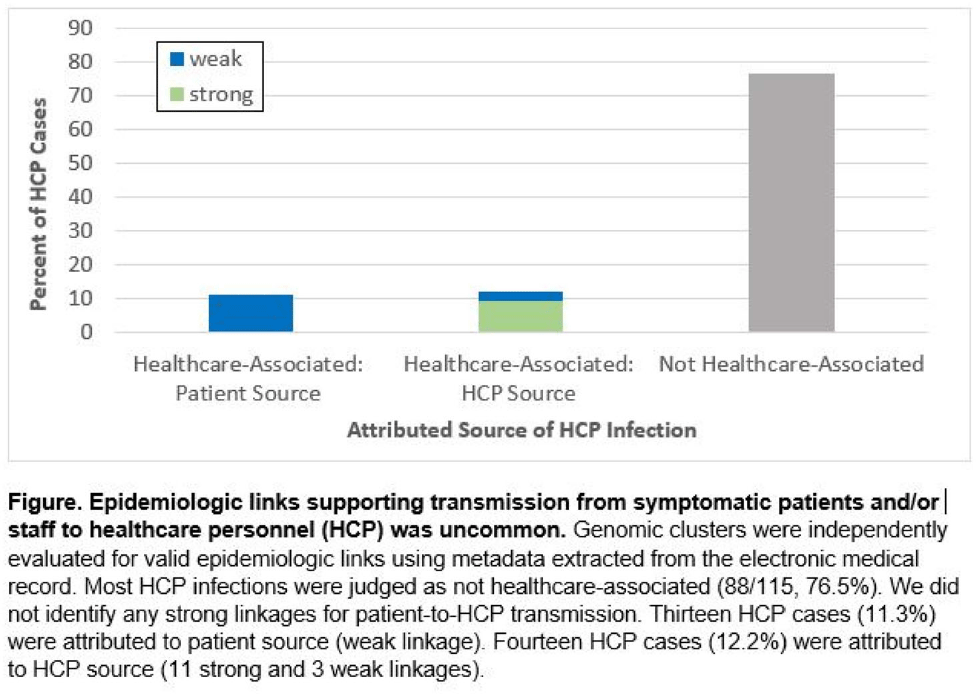
Background: Contact tracing alone is often inadequate to determine the source of healthcare personnel (HCP) COVID-19 when SARS-CoV-2 is widespread in the community. We combined whole-genome sequencing (WGS) with traditional epidemiologic analysis to investigate the frequency with which patients or other HCP with symptomatic COVID-19 acted as the source of HCP infection at a large tertiary-care center early in the pandemic. Methods: Cohort samples were selected from patients and HCP with PCR-positive SARS-CoV-2 infection from a period with complete retention of samples (March 14, 2021–April 10, 2020) at Rush University Medical Center, a 664-bed hospital in Chicago, Illinois. During this period, testing was limited to symptomatic patients and HCP. Recommended respiratory equipment for HCP evolved under guidance, including a 19-day period when medical face masks were recommended for COVID-19 care except for aerosol-generating procedures. Viral RNA was extracted and sequenced (NovaSeq, Illumina) from remnant nasopharyngeal swab samples in M4RT viral transport medium. Genomes with >90% coverage underwent cluster detection using a 2 single-nucleotide variant genetic distance cutoff. Genomic clusters were independently evaluated for valid epidemiologic links by 2 infectious diseases physicians (with a third adjudicator) using metadata extracted from the electronic medical record and according to predetermined criteria (Table 1). Results: In total, 1,031 SARS-CoV-2 sequences were analyzed, identifying 49 genomic clusters with HCP (median, 8; range, 2–43 members per cluster; total, 268 patients and 115 HCP) (Fig. 1). Also, 20,190 flowsheet activities were documented for cohort HCP and patient interactions, including 686 instances in which a cohort HCP contributed to a cohort patient’s chart. Most HCP infections were considered not healthcare associated (88 of 115, 76.5%). We did not identify any strong linkages for patient-to-HCP transmission. Moreover, 13 HCP cases (11.3%) were attributed to patient source (weak linkage). Also, 14 HCP cases (12.2%) were attributed to HCP source (11 strong and 3 weak linkages). Weak linkages were due to lack of epidemiologic data for HCP location, particularly nonclinical staff (eg, an environmental service worker who lacked location documentation to rule out patient-specific contact). Agreement for epidemiologic linkage between the 2 evaluators was high (κ, 0.91). Conclusions: Using genomic and epidemiologic data, we found that most HCP COVID-19 infections were not healthcare associated. We found weak evidence to support symptomatic patient-to-HCP transmission of SARS-CoV-2 and stronger evidence for HCP-to-HCP transmission. Large genomic clusters without plausible epidemiologic links were identified, reflecting the limited utility of genomic surveillance alone to characterize chains of transmission of SARS-CoV-2 during extensive community spread.
Funding: None
Disclosures: None


‘He Saw Heaven Opened’: Heavenly Temple and Universal Mission in Luke-Acts
-
- Journal:
- New Testament Studies / Volume 68 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 09 December 2021, pp. 38-51
- Print publication:
- January 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Whole-genome sequencing for neonatal intensive care unit outbreak investigations: Insights and lessons learned – ADDENDUM
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 03 August 2021, e18
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Next Generation File Formats and Platforms
-
- Journal:
- Microscopy and Microanalysis / Volume 27 / Issue S1 / August 2021
- Published online by Cambridge University Press:
- 30 July 2021, p. 2842
- Print publication:
- August 2021
-
- Article
-
- You have access
- Export citation
Admission and Discharge Sampling Underestimates Multidrug-Resistant Organism (MDRO) Acquisition in an Intensive Care Unit
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
-
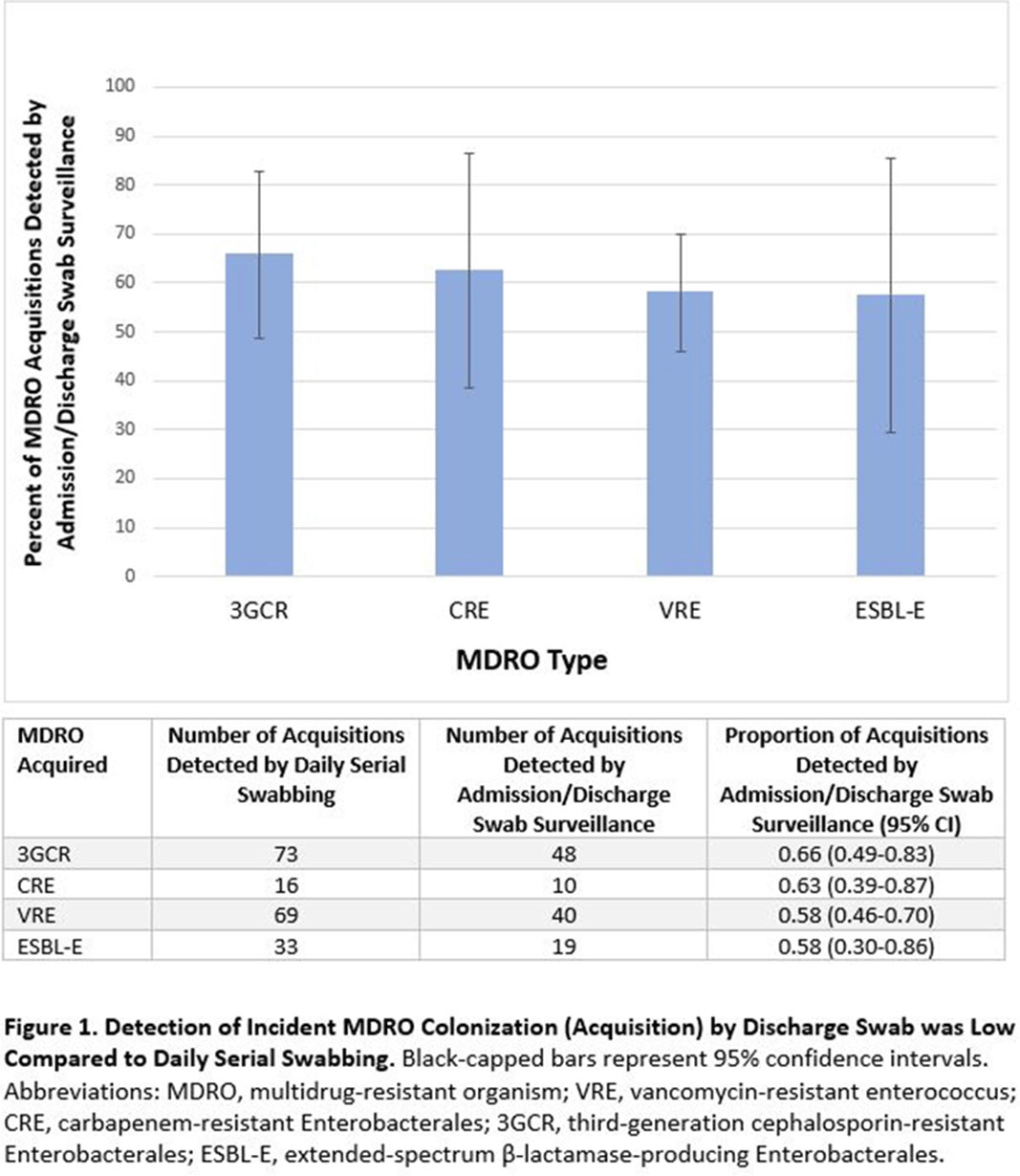
Background: Identification of hospitalized patients with enteric multidrug-resistant organism (MDRO) carriage, combined with implementation of targeted infection control interventions, may help reduce MDRO transmission. However, the optimal surveillance approach has not been defined. We sought to determine whether daily serial rectal surveillance for MDROs detects more incident cases (acquisition) of MDRO colonization in medical intensive care unit (MICU) patients than admission and discharge surveillance alone. Methods: Prospective longitudinal observational single-center study from January 11, 2017, to January 11, 2018. Inclusion criteria were ≥3 consecutive MICU days and ≥2 rectal or stool swabs per MICU admission. Daily rectal or stool swabs were collected from patients and cultured for MDROs, including vancomycin-resistant Enterococcus (VRE), carbapenem-resistant Enterobacterales (CRE), third-generation cephalosporin-resistant Enterobacterales (3GCR), and extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E) (as a subset of 3GCR). MDRO detection at any time during the MICU stay was used to calculate prevalent colonization. Incident colonization (acquisition) was defined as new detection of an MDRO after at least 1 prior negative swab. We then determined the proportion of prevalent and incident cases detected by daily testing that were also detected when only first swabs (admission) and last swabs (discharge) were tested. Data were analyzed using SAS version 9.4 software. Results: In total, 939 MICU stays of 842 patients were analyzed. Patient characteristics were median age 64 years (interquartile range [IQR], 51–74), median MICU length of stay 5 days (IQR, 3–8), median number of samples per admission 3 (IQR, 2–5), and median Charlson index 4 (IQR, 2–7). Prevalent colonization with any MDRO was detected by daily swabbing in 401 stays (42.7%). Compared to daily serial swabbing, an admission- and discharge-only approach detected ≥86% of MDRO cases (ie, overall prevalent MDRO colonization). Detection of incident MDRO colonization by an admission- or discharge-only approach would have detected fewer cases than daily swabbing (Figure 1); ≥34% of total MDRO acquisitions would have been missed. Conclusions: Testing patients upon admission and discharge to an MICU may fail to detect MDRO acquisition in more than one-third of patients, thereby reducing the effectiveness of MDRO control programs that are targeted against known MDRO carriers. The poor performance of a single discharge swab may be due to intermittent or low-level MDRO shedding, inadequate sampling, or transient MDRO colonization. Additional research is needed to determine the optimal surveillance approach of enteric MDRO carriage.
Funding: No
Disclosures: None
Figure 1.

Whole-genome sequencing for neonatal intensive care unit outbreak investigations: Insights and lessons learned
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 24 June 2021, e2
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A history of high-power laser research and development in the United Kingdom
- Part of
-
- Journal:
- High Power Laser Science and Engineering / Volume 9 / 2021
- Published online by Cambridge University Press:
- 27 April 2021, e18
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
KPC-Producing Enterobacter cloacae Transfer Through Pipework Between Hospital Sink Waste Traps in a Laboratory Model System
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s308-s309
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Baseline results from the European non-interventional Antipsychotic Long acTing injection in schizOphrenia (ALTO) study
-
- Journal:
- European Psychiatry / Volume 52 / August 2018
- Published online by Cambridge University Press:
- 01 January 2020, pp. 85-94
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An analysis of the impacts of Cretaceous oceanic anoxic events on global molluscan diversity dynamics
-
- Journal:
- Paleobiology / Volume 45 / Issue 2 / May 2019
- Published online by Cambridge University Press:
- 10 April 2019, pp. 280-295
-
- Article
- Export citation
The Hennepin Ketamine Study Investigators’ Reply
-
- Journal:
- Prehospital and Disaster Medicine / Volume 34 / Issue 2 / April 2019
- Published online by Cambridge University Press:
- 03 May 2019, pp. 111-113
- Print publication:
- April 2019
-
- Article
-
- You have access
- HTML
- Export citation
2507 A novel multi-photon microscopy method for neuronavigation in deep brain stimulation surgery
-
- Journal:
- Journal of Clinical and Translational Science / Volume 2 / Issue S1 / June 2018
- Published online by Cambridge University Press:
- 21 November 2018, pp. 2-3
-
- Article
-
- You have access
- Open access
- Export citation
9 - Balancing Privacy and Public Safety in the Post-Snowden Era
- from Part II - Surveillance Applications
-
-
- Book:
- The Cambridge Handbook of Surveillance Law
- Published online:
- 20 October 2017
- Print publication:
- 12 October 2017, pp 227-247
-
- Chapter
- Export citation
Modifiable Risk Factors for the Spread of Klebsiella pneumoniae Carbapenemase-Producing Enterobacteriaceae Among Long-Term Acute-Care Hospital Patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 6 / June 2017
- Published online by Cambridge University Press:
- 11 April 2017, pp. 670-677
- Print publication:
- June 2017
-
- Article
- Export citation
The Last Interglacial Ocean
-
- Journal:
- Quaternary Research / Volume 21 / Issue 2 / February 1984
- Published online by Cambridge University Press:
- 20 January 2017, pp. 123-224
-
- Article
- Export citation
Age Dating and the Orbital Theory of the Ice Ages: Development of a High-Resolution 0 to 300,000-Year Chronostratigraphy1
-
- Journal:
- Quaternary Research / Volume 27 / Issue 1 / January 1987
- Published online by Cambridge University Press:
- 20 January 2017, pp. 1-29
-
- Article
- Export citation
