
421 results
Presenteeism Among Healthcare Professionals (HCP) During the COVID-19 Pandemic: Survey of Perceived Barriers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s104
-
- Article
-
- You have access
- Open access
- Export citation
-
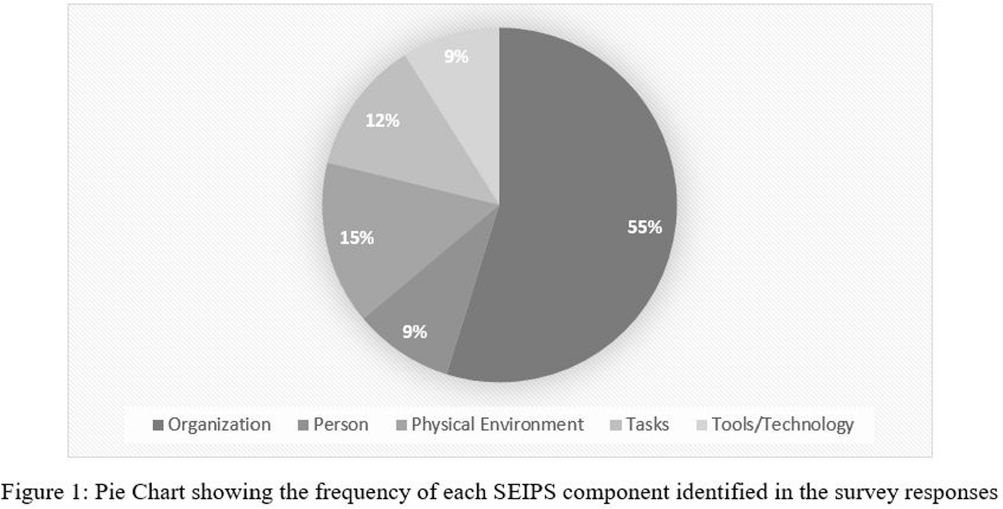
Background: Presenteeism when ill in healthcare personnel (HCP) can contribute to the spread of respiratory illness among HCP and patients. However, during the COVID-19 pandemic and now, there are substantial challenges preventing HCP from staying home when ill. We examined these challenges using the Systems Engineering Initiative for Patient Safety (SEIPS) framework. Method: As part of a larger anonymous electronic survey between 3/11/2022 and 4/12/2022 at an academic tertiary referral center, in inpatient and ambulatory settings where respondents were asked to describe factors impacting presenteeism when ill, we analyzed free-text responses using the SEIPS categories of tasks, tools/technology, person, organization, and physical environment. Result: 522 comments were received in response to the open-ended survey question asking individuals to describe any factors that would assist them in remaining home and/or help them get tested for COVID-19 when they have symptoms of a respiratory illness; 21 were excluded due to absent or incomplete response. Of the remaining responses (N = 501, Figure 1), 82% were associated with a single SEIPS component such as organization (N = 409), while other responses discussed factors that involved two SEIPS components, in no particular order (N = 92). A majority of the responses (N = 324, 55%) reported organizational barriers, frequently citing a strict sick call-in policy as well as a lack of protected time-off for COVID-19 testing or related absences. The next two most commonly identified components were physical environment (N= 88, 15%) and tasks (N = 72, 12%), mentioning barriers such as far distances to testing centers and prolonged waiting periods for testing Results: The person and tools/technology components were less commonly identified, with a frequency of 9% each. Conclusion: A number of systems level factors were identified that may impact the ability of HCP to stay home when ill. Interventions to help overcome HCP perceived barriers to staying home when experiencing respiratory symptoms should focus on the policies and practices within an organization. Communication from leadership should support staying home with respiratory symptoms by creating plans for coverage and back up consistently across all employee types in direct care.

A Comparison of Variable Input Strategies used for Risk-adjustment Models of Antimicrobial Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
-
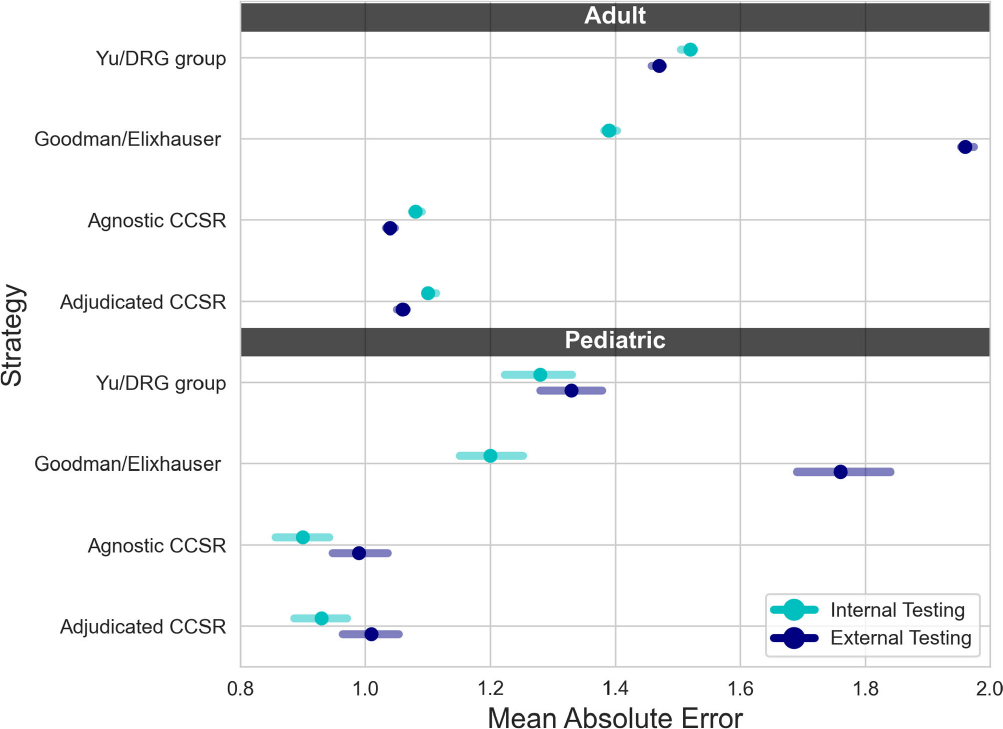
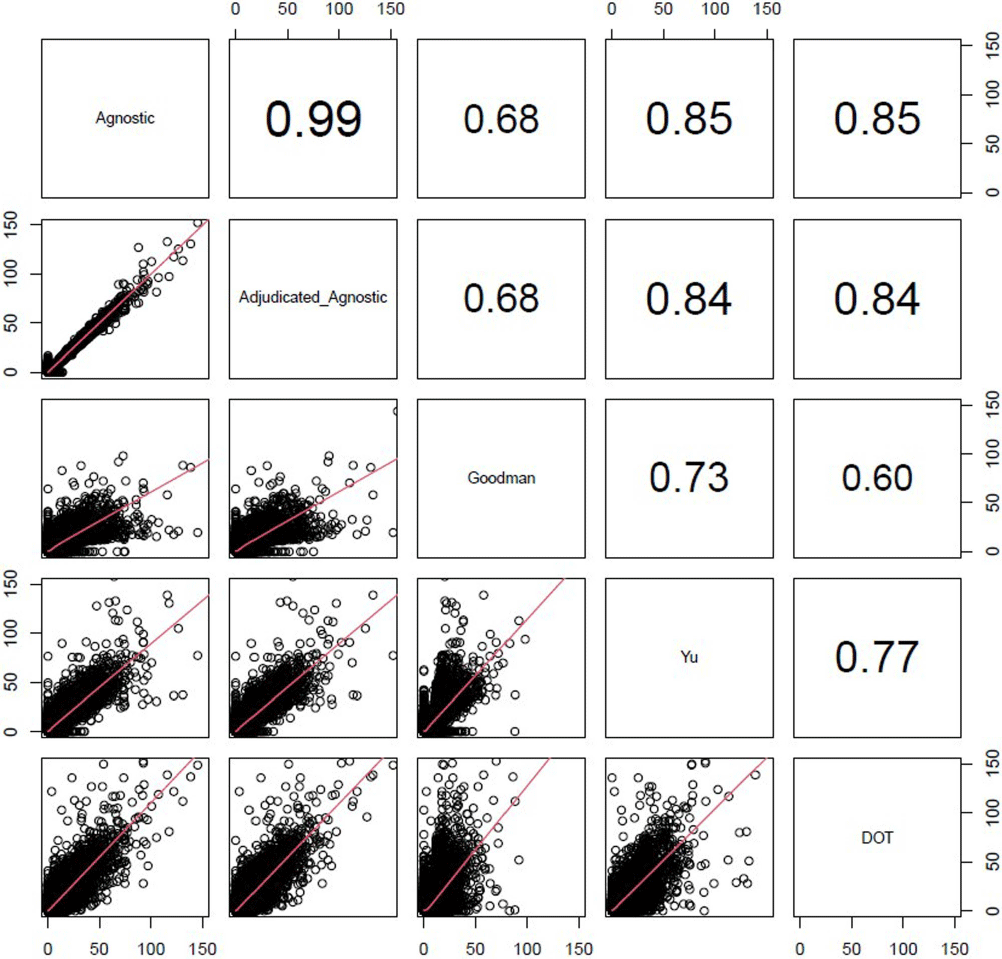
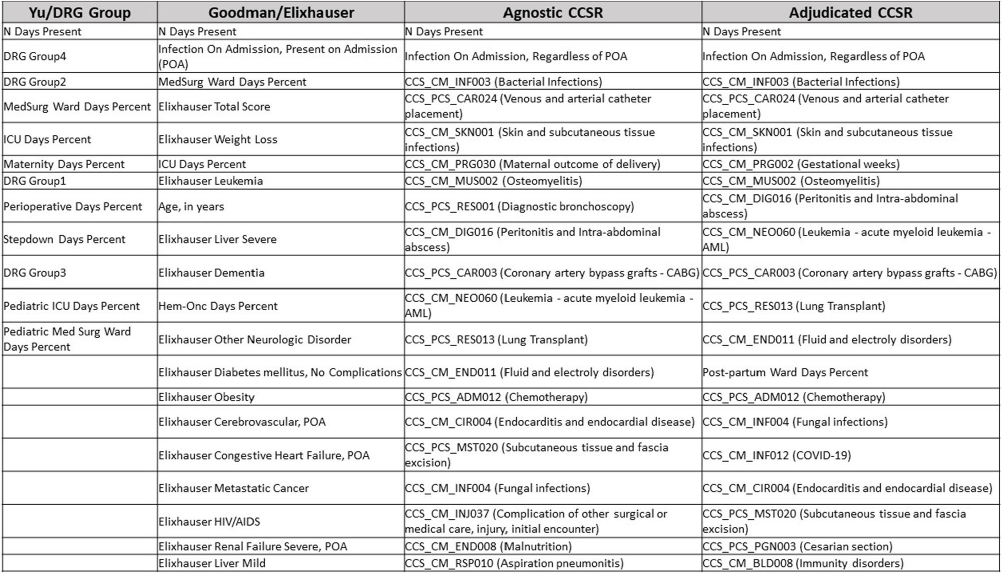
Background: External comparisons of antimicrobial use (AU) may be more informative if adjusted for encounter characteristics. Optimal methods to define input variables for encounter-level risk-adjustment models of AU are not established. Methods: This retrospective analysis of electronic health record data included 50 US hospitals in 2020-2021. We used NHSN definitions for all antibacterials days of therapy (DOT), including adult and pediatric encounters with at least 1 day present in inpatient locations. We assessed 4 methods to define input variables: 1) diagnosis-related group (DRG) categories by Yu et al., 2) adjudicated Elixhauser comorbidity categories by Goodman et al., 3) all Clinical Classification Software Refined (CCSR) diagnosis and procedure categories, and 4) adjudicated CCSR categories where codes not appropriate for AU risk-adjustment were excluded by expert consensus, requiring review of 867 codes over 4 months to attain consensus. Data were split randomly, stratified by bed size as follows: 1) training dataset including two-thirds of encounters among two-thirds of hospitals; 2) internal testing set including one-third of encounters within training hospitals, and 3) external testing set including the remaining one-third of hospitals. We used a gradient-boosted machine (GBM) tree-based model and two-staged approach to first identify encounters with zero DOT, then estimate DOT among those with >0.5 probability of receiving antibiotics. Accuracy was assessed using mean absolute error (MAE) in testing datasets. Correlation plots compared model estimates and observed DOT among testing datasets. The top 20 most influential variables were defined using modeled variable importance. Results: Our datasets included 629,445 training, 314,971 internal testing, and 419,109 external testing encounters. Demographic data included 41% male, 59% non-Hispanic White, 25% non-Hispanic Black, 9% Hispanic, and 5% pediatric encounters. DRG was missing in 29% of encounters. MAE was lower in pediatrics as compared to adults, and lowest for models incorporating CCSR inputs (Figure 1). Performance in internal and external testing was similar, though Goodman/Elixhauser variable strategies were less accurate in external testing and underestimated long DOT outliers (Figure 2). Agnostic and adjudicated CCSR model estimates were highly correlated; their influential variables lists were similar (Figure 3). Conclusion: Larger numbers of CCSR diagnosis and procedure inputs improved risk-adjustment model accuracy compared with prior strategies. Variable importance and accuracy were similar for agnostic and adjudicated approaches. However, maintaining adjudications by experts would require significant time and potentially introduce personal bias. If findings are confirmed, the need for expert adjudication of input variables should be reconsidered.
Disclosure: Elizabeth Dodds Ashley: Advisor- HealthTrackRx. David J Weber: Consultant on vaccines: Pfizer; DSMB chair: GSK; Consultant on disinfection: BD, GAMA, PDI, Germitec



Are paediatric cardiology textbooks obsolete in the current digital era?
-
- Journal:
- Cardiology in the Young , First View
- Published online by Cambridge University Press:
- 13 September 2024, pp. 1-4
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Striatal brain volume linked to severity of substance use in high-risk incarcerated youth
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 13 May 2024, pp. 1-10
-
- Article
- Export citation
25 Evaluating serum copper and kidney function in a cohort of bariatric surgery patients
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 7
-
- Article
-
- You have access
- Open access
- Export citation
Properties of Water in Calcium- and Hexadecyltrimethylammonium-Exchanged Bentonite
-
- Journal:
- Clays and Clay Minerals / Volume 47 / Issue 1 / February 1999
- Published online by Cambridge University Press:
- 28 February 2024, pp. 28-35
-
- Article
- Export citation
The devil’s in the defaults: An interrupted time-series analysis of the impact of default duration elimination on exposure to fluoroquinolone therapy
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 13 February 2024, pp. 733-739
- Print publication:
- June 2024
-
- Article
- Export citation
Variation of subclinical psychosis across 16 sites in Europe and Brazil: findings from the multi-national EU-GEI study
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 8 / June 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1810-1823
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Weathering of Almandine Garnet: Influence of Secondary Minerals on the Rate-Determining Step, and Implications for Regolith-Scale Al Mobilization
-
- Journal:
- Clays and Clay Minerals / Volume 61 / Issue 1 / February 2013
- Published online by Cambridge University Press:
- 01 January 2024, pp. 34-56
-
- Article
- Export citation
Properties of surface-modified colloidal particles
-
- Journal:
- Clays and Clay Minerals / Volume 54 / Issue 1 / February 2006
- Published online by Cambridge University Press:
- 01 January 2024, pp. 12-24
-
- Article
- Export citation
41 Predictors of Cognitive Symptoms Following Adult Civilian Mild Traumatic Brain Injury
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 148
-
- Article
-
- You have access
- Export citation
APPROACHES TO ANCIENT HOUSING - (J.A.) Baird, (A.) Pudsey (edd.) Housing in the Ancient Mediterranean World. Material and Textual Approaches. Pp. xviii + 499, b/w & colour ills, b/w & colour maps. Cambridge: Cambridge University Press, 2022. Cased, £105, US$135. ISBN: 978-1-108-84526-7.
-
- Journal:
- The Classical Review / Volume 74 / Issue 1 / April 2024
- Published online by Cambridge University Press:
- 20 December 2023, pp. 221-224
- Print publication:
- April 2024
-
- Article
- Export citation
Promoting equity, inclusion, and efficiency: A team science approach to the development of authorship guidelines for a multi-disciplinary research team
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 30 November 2023, e265
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
EMS Responses for Pediatric Behavioral Health Emergencies in the United States: A 4-Year Descriptive Evaluation
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 30 November 2023, pp. 784-791
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies used for the COVID-OUT decentralized trial of outpatient treatment of SARS-CoV-2
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 07 November 2023, e242
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Introduction to A Compendium of Strategies to Prevent Healthcare-Associated Infections In Acute-Care Hospitals: 2022 Updates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 19 October 2023, pp. 1533-1539
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Modeling the development of cognitive reserve in children: A residual index approach
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 3 / March 2024
- Published online by Cambridge University Press:
- 05 September 2023, pp. 264-272
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Executive Summary: A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute-Care Hospitals: 2022 Updates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 22 August 2023, pp. 1540-1554
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Assessing enrollment of eligible infants in the national pediatric cardiology quality improvement collaborative (NPC-QIC) through linkage to the pediatric cardiac critical care consortium (PC4) registry
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 12 July 2023, pp. 373-379
-
- Article
- Export citation
