
237 results
Neurophysiological evidence of motor preparation dysfunction to inner speech in schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S243
-
- Article
-
- You have access
- Open access
- Export citation
Impact of COVID-19 restriction on weight, physical activity, diet and psychological distress on people with polycystic ovary syndrome
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE1 / April 2024
- Published online by Cambridge University Press:
- 07 May 2024, E82
-
- Article
-
- You have access
- Export citation
The role of interoception in the mechanism of pain and fatigue in fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, p. S139
-
- Article
-
- You have access
- Open access
- Export citation
Dementia patients have greater anti-cholinergic drug burden on discharge from hospital: A multicentre cross-sectional study
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S422-S423
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Anticholinergic medications block cholinergic transmission. The central effects of anticholinergic drugs can be particularly marked in patients with dementia. Furthermore, anticholinergics antagonise the effects of cholinesterase inhibitors, the main dementia treatment.
ObjectivesThis study aimed to assess anticholinergic drug prescribing among dementia patients before and after admission to UK acute hospitals.
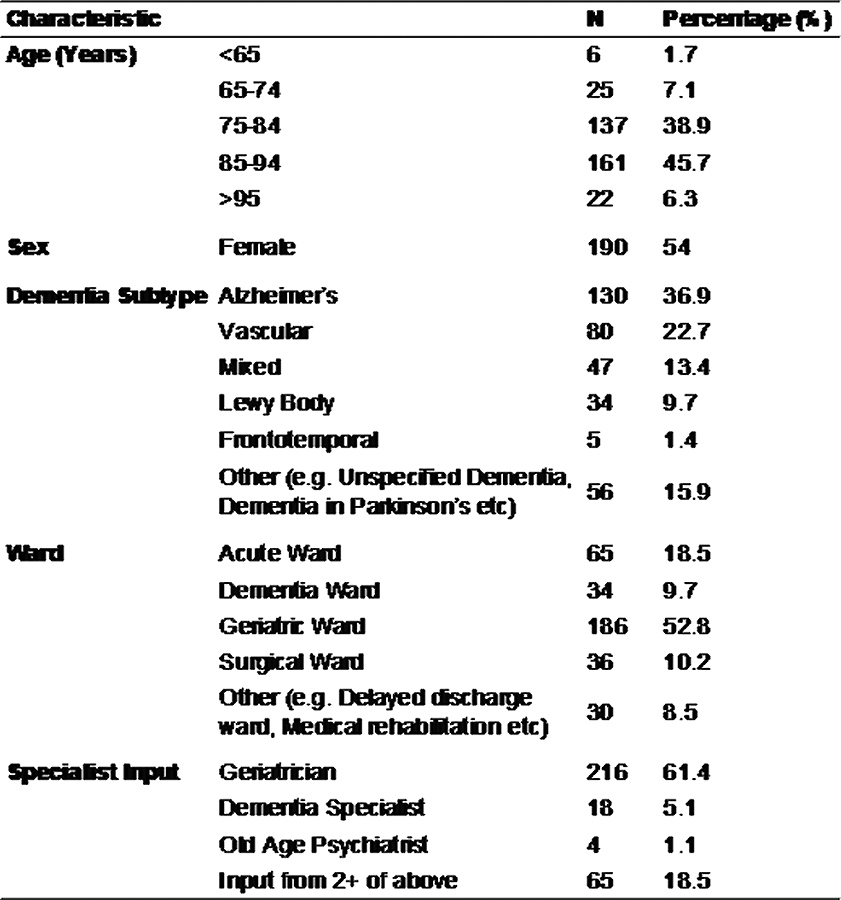
Methods352 patients with dementia were included from 17 hospitals in the UK. All were admitted to surgical, medical or Care of the Elderly wards in 2019. Information about patients’ prescriptions were recorded on a standardised form. An evidence-based online calculator was used to calculate the anticholinergic drug burden of each patient. The correlation between two subgroups upon admission and discharge was tested with Spearman’s Rank Correlation.
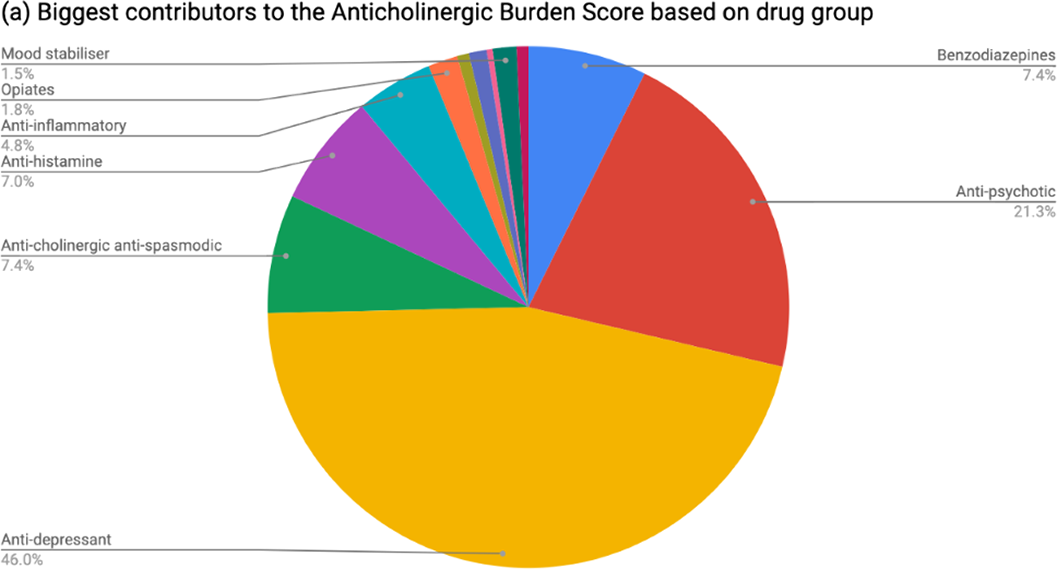
ResultsTable 1 shows patient demographics. On admission, 37.8% of patients had an anticholinergic burden score ≥1 and 5.68% ≥3. At discharge, 43.2% of patients had an anticholinergic burden score ≥1 and 9.1% ≥3. The increase was statistically significant (rho 0.688; p=2.2x10-16). The most common group of anticholinergic medications prescribed at discharge were psychotropics (see Figure 1). Among patients prescribed cholinesterase inhibitors, 44.9% were also taking anticholinergic medications.
 Conclusions
ConclusionsThis multicentre cross-sectional study found that people with dementia are frequently prescribed anticholinergic drugs, even if also taking cholinesterase inhibitors, and are significantly more likely to be discharged with a higher anticholinergic drug burden than on admission to hospital.
Conflict of interestThis project was planned and executed by the authors on behalf of SPARC (Student Psychiatry Audit and Research Collaborative). We thank the National Student Association of Medical Research for allowing us use of the Enketo platform. Judith Harrison was su


Management of ENT emergencies during the coronavirus disease 2019 pandemic
- Part of
-
- Journal:
- The Journal of Laryngology & Otology / Volume 135 / Issue 2 / February 2021
- Published online by Cambridge University Press:
- 22 February 2021, pp. 117-124
- Print publication:
- February 2021
-
- Article
- Export citation
P091: Essential elements to implementing the paramedics providing palliative care at home program: an application of the Consolidated Framework for Implementation Research (CFIR)
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 22 / Issue S1 / May 2020
- Published online by Cambridge University Press:
- 13 May 2020, p. S97
- Print publication:
- May 2020
-
- Article
-
- You have access
- Export citation
P0305 - Frequency of psychosis-like symptoms in a non-clinical population of 12 year olds: Results from the Alspac birth cohort
-
- Journal:
- European Psychiatry / Volume 23 / Issue S2 / April 2008
- Published online by Cambridge University Press:
- 16 April 2020, p. S282
-
- Article
-
- You have access
- Export citation
Assessing the risk of venous thromboembolism in psychiatric in-patients
-
- Journal:
- European Psychiatry / Volume 41 / Issue S1 / April 2017
- Published online by Cambridge University Press:
- 23 March 2020, p. S686
-
- Article
-
- You have access
- Export citation
Consensus Statements On Cognitive Dysfunction In Depression In The Uk: Rationale And Process For Gaining Consensus
-
- Journal:
- European Psychiatry / Volume 33 / Issue S1 / March 2016
- Published online by Cambridge University Press:
- 23 March 2020, p. S424
-
- Article
-
- You have access
- Export citation
The use of Polygenic Risk Scores to Inform Aetiology of Mood and Psychotic Disorders
-
- Journal:
- European Psychiatry / Volume 41 / Issue S1 / April 2017
- Published online by Cambridge University Press:
- 23 March 2020, p. S166
-
- Article
-
- You have access
- Export citation
Chapter Two - Analytical approaches for microbiome research
-
-
- Book:
- Microbiomes of Soils, Plants and Animals
- Published online:
- 07 March 2020
- Print publication:
- 12 March 2020, pp 8-28
-
- Chapter
- Export citation
Fundamental physics with the Square Kilometre Array
- Part of
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 37 / 2020
- Published online by Cambridge University Press:
- 27 January 2020, e002
-
- Article
-
- You have access
- HTML
- Export citation
Post-jökulhlaup geomorphic evolution of the Gígjökull Basin, Iceland
-
- Journal:
- Annals of Glaciology / Volume 60 / Issue 80 / December 2019
- Published online by Cambridge University Press:
- 10 October 2019, pp. 127-137
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Equivalency of the diagnostic accuracy of the PHQ-8 and PHQ-9: a systematic review and individual participant data meta-analysis – ERRATUM
-
- Journal:
- Psychological Medicine / Volume 50 / Issue 16 / December 2020
- Published online by Cambridge University Press:
- 19 August 2019, p. 2816
-
- Article
-
- You have access
- HTML
- Export citation
Equivalency of the diagnostic accuracy of the PHQ-8 and PHQ-9: a systematic review and individual participant data meta-analysis
-
- Journal:
- Psychological Medicine / Volume 50 / Issue 8 / June 2020
- Published online by Cambridge University Press:
- 12 July 2019, pp. 1368-1380
-
- Article
- Export citation
To investigate the effect of grass-based feeding practices on insulin sensitivity, adipose tissue inflammation and hepatic lipid composition in a transgenic mouse model
-
- Journal:
- Proceedings of the Nutrition Society / Volume 78 / Issue OCE1 / 2019
- Published online by Cambridge University Press:
- 07 March 2019, E15
-
- Article
-
- You have access
- HTML
- Export citation
Establishing the impact of powerful AGN on their host galaxies
-
- Journal:
- Proceedings of the International Astronomical Union / Volume 15 / Issue S359 / March 2019
- Published online by Cambridge University Press:
- 29 March 2021, pp. 203-211
- Print publication:
- March 2019
-
- Article
-
- You have access
- Export citation
Simulation of Legionnaires’ disease prospective spatiotemporal cluster detection, Allegheny County, Pennsylvania, USA
-
- Journal:
- Epidemiology & Infection / Volume 147 / 2019
- Published online by Cambridge University Press:
- 18 October 2018, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Smectite-polymer interactions in aqueous systems
-
- Journal:
- Clay Minerals / Volume 18 / Issue 4 / December 1983
- Published online by Cambridge University Press:
- 09 July 2018, pp. 373-397
-
- Article
- Export citation
Electro-fluorescence studies of the binding of fluorescent dyes to sepiolite
-
- Journal:
- Clay Minerals / Volume 31 / Issue 1 / March 1996
- Published online by Cambridge University Press:
- 09 July 2018, pp. 81-94
-
- Article
- Export citation
