
526 results
P.057 Achievement of minimal symptom expression in acetylcholine receptor antibody-positive participants treated with efgartigimod in ADAPT/ADAPT+
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 51 / Issue s1 / June 2024
- Published online by Cambridge University Press:
- 24 May 2024, p. S31
-
- Article
-
- You have access
- Export citation
A crinoid fauna and a new species of Pycnocrinus from the Martinsburg Formation (Upper Ordovician), lower Hudson Valley, New York
-
- Journal:
- Journal of Paleontology , First View
- Published online by Cambridge University Press:
- 13 May 2024, pp. 1-18
-
- Article
- Export citation
Alcohol milestones and internalizing, externalizing, and executive function: longitudinal and polygenic score associations
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 09 May 2024, pp. 1-14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Separating the rash from the chaff: novel clinical decision support deployed during the mpox outbreak
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 02 April 2024, pp. 1-3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Crystal Structure of Bannisterite
-
- Journal:
- Clays and Clay Minerals / Volume 40 / Issue 2 / April 1992
- Published online by Cambridge University Press:
- 28 February 2024, pp. 129-144
-
- Article
- Export citation
Implementation of contact precautions for multidrug-resistant organisms in the post–COVID-19 pandemic era: An updated national Emerging Infections Network (EIN) survey
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 14 February 2024, pp. 703-708
- Print publication:
- June 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Peer review of clinical and translational research manuscripts: Perspectives from statistical collaborators
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 04 January 2024, e20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
28 Traumatic Brain Injury and Genetic Risk for Alzheimer's Disease Influence ß-Amyloid Levels
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 238-239
-
- Article
-
- You have access
- Export citation
4 Urinary Fluoride Levels and Metal Co-Exposures Among Pregnant Women in Los Angeles, California
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 867-868
-
- Article
-
- You have access
- Export citation
Age and beliefs about vaccines associated with COVID-19 vaccination among US Veterans
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 23 October 2023, e184
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Use of contact precautions for multidrug-resistant organisms and the impact of the COVID-19 pandemic: An Emerging Infections Network (EIN) survey
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s102-s103
-
- Article
-
- You have access
- Open access
- Export citation
-
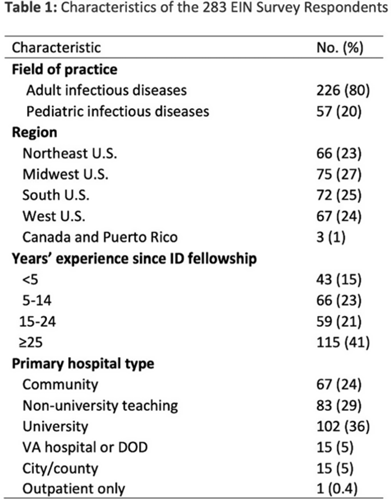
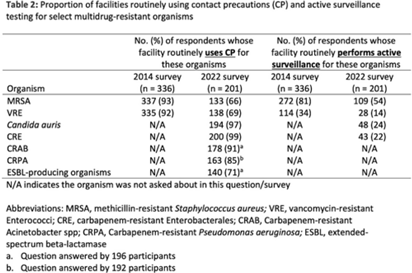
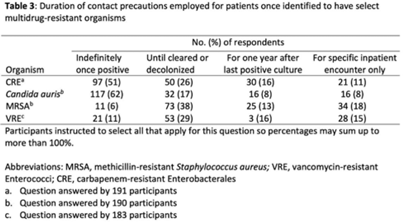
Background: The CDC recommends routine use of contact precautions for patients infected or colonized with multidrug-resistant organisms (MDROs). There is variability in implementation of and adherence to this recommendation, which we hypothesized may have been exacerbated by the COVID-19 pandemic. Methods: In September 2022, we emailed an 8-question survey to Emerging Infections Network (EIN) physician members with infection prevention and hospital epidemiology responsibilities. The survey asked about the respondent’s primary hospital’s recommendations on transmission-based precautions, adjunctive measures to reduce MDRO transmission, and changes that occurred during the COVID-19 pandemic. We sent 2 reminder emails over a 1-month period. We used descriptive statistics to summarize the data and to compare results to a similar EIN survey (n = 336) administered in 2014 (Russell D, et al. doi:10.1017/ice.2015.246). Results: Of 708 EIN members, 283 (40%) responded to the survey, and 201 were involved in infection prevention. Most respondents were adult infectious diseases physicians (n = 228, 80%) with at least 15 years of experience (n = 174, 63%). Respondents were well distributed among community, academic, and nonuniversity teaching facilities (Table 1). Most respondents reported that their facility routinely used CP for methicillin-resistant Staphylococcus aureus (MRSA, 66%) and vancomycin-resistant Enterococcus (VRE, 69%), compared to 93% and 92% respectively, in the 2014 survey. Nearly all (>90%) reported using contact precautions for Candida auris, carbapenem-resistant Enterobacterales (CRE), and carbapenem-resistant Acinetobacter spp, but there was variability in the use of contact precautions for carbapenem-resistant Pseudomonas aeruginosa and extended-spectrum β-lactamase–producing gram-negative organisms. In 2014, 81% reported that their hospital performed active surveillance testing for MRSA, and in 2022 this rate fell to 54% (Table 2). The duration of contact precautions varied by MDRO (Table 3). Compared to 2014, in 2022 facilities were less likely to use contact precautions indefinitely for MRSA (18% vs 6%) and VRE (31% vs 11%). Also, 180 facilities (90%) performed chlorhexidine bathing in at least some inpatients and 106 facilities (53%) used ultraviolet light or hydrogen peroxide vapor disinfection at discharge in some rooms. Furthermore, 89 facilities (44%) reported institutional changes to contact precautions policies after the start of the COVID-19 pandemic that remain in place. Conclusions: Use of contact precautions for patients with MDROs is heterogenous, and policies vary based on the organism. Although most hospitals still routinely use contact precautions for MRSA and VRE, this practice has declined substantially since 2014. Changes in contact-precaution policies may have been influenced by the COVID-19 pandemic, and more specifically, contemporary public health guidance is needed to define who requires contact precautions and for what duration.
Disclosures: None



Effect of an initial specimen diversion device on blood-culture contamination rates and vancomycin usage: A quasi-experimental study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 03 August 2023, pp. 100-102
- Print publication:
- January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
17 - Practical Calculations Involving Two-Component Fermions
- from Part IV - Sample Calculations in the Standard Model and Its Supersymmetric Extension
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 667-681
-
- Chapter
- Export citation
C - Appendix C Behavior of Fermion Bilinears under P, T, C
- from Part V - The Appendices
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 819-824
-
- Chapter
- Export citation
5 - Anomalies
- from Part I - Spin-1/2 Fermions in Quantum Field Theory, the Standard Model, and Beyond
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 229-258
-
- Chapter
- Export citation
-
Summary
Consider a collection of
two-component left-handed
Preface
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp xiii-xvi
-
- Chapter
- Export citation
J - Appendix J MSSM and RPV Fermion Interaction Vertices
- from Part V - The Appendices
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 952-967
-
- Chapter
- Export citation
4 - Gauge Theories and the Standard Model
- from Part I - Spin-1/2 Fermions in Quantum Field Theory, the Standard Model, and Beyond
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 191-228
-
- Chapter
- Export citation
E - Appendix E The Spin-1/2 and Spin-1 Wave Functions
- from Part V - The Appendices
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp 842-872
-
- Chapter
- Export citation
Acknowledgments
-
- Book:
- From Spinors to Supersymmetry
- Published online:
- 06 July 2023
- Print publication:
- 08 June 2023, pp xvii-xviii
-
- Chapter
- Export citation
