


Young children and their parents are important targets of obesity prevention because in the early years of life children gain knowledge about food, dietary preferences and eating habits that may underpin lifelong eating habits( Reference Campbell and Hesketh 1 ). Within the home environment, shaped by parents, young children have their earliest experiences with food and eating, and from these experiences they gain their knowledge of nutrition. The home food environment is determined by many factors including food availability, feeding rules, parent role modelling, discussion about food and parents’ food preparation skills( Reference Birch and Davison 2 – Reference Worsley 4 ). When forming the home food environment parents are likely to be influenced by their own attitudes and nutrition knowledge, and therefore these two factors can be important for children's nutrition knowledge, food preferences and eating habits( Reference Gibson, Wardle and Watts 5 ).
Knowledge is a complex system of beliefs determined by individuals’ experiences within their social, physical and biological environments( Reference Worsley 4 ). In the context of nutrition and eating, knowledge is commonly defined as the understanding of the health benefits of food and nutrients( Reference Wardle 6 ). However, nutrition knowledge may be defined in many ways, and it is important to consider the relevance of the definition for the target group. Domains of nutrition knowledge relevant for nutrition professionals may not be relevant for, or understood by, the general public( Reference Worsley 4 ). For this reason, governments develop dietary guidelines to provide consumers with relevant information to make informed choices about the foods they eat. In Australia, two key documents serve this purpose, the Dietary Guidelines for Children and Adolescents and the Australian Guide to Healthy Eating( 7 , 8 ).
Of the many factors that can influence eating behaviours, a lack of nutrition knowledge is one of the most amenable to change, and improving nutrition knowledge through nutrition education is a common component of obesity interventions( Reference Campbell and Hesketh 1 ). Studies in children and adults have shown positive associations between nutrition knowledge and likelihood of healthy food consumption, indicating that nutrition knowledge is necessary for making healthier food choices( Reference Worsley 4 , Reference Gibson, Wardle and Watts 5 , Reference Wardle, Parmenter and Waller 9 ). Despite this, there has been little investigation of factors that can shape young children's nutrition knowledge( Reference Gibson, Wardle and Watts 5 ). The aim of the present cross-sectional study was therefore to investigate the extent to which parents’ nutrition knowledge and attitudes about food predict young children's knowledge of healthy foods.
Methods
Participants
The study was conducted in Adelaide, South Australia in June to September of 2008. Children aged 5–6 years and their parents were recruited from primary schools in metropolitan Adelaide. There were no exclusion criteria, although parents and children needed to understand English to take part. The Socio-Economic Index for Areas (SEIFA) Index of Relative Advantage and Disadvantage was used to stratify schools according to socio-economic status (SES) according to postcodes based on Australian Bureau of Statistics census data from 2006 for income, education attainment and occupation( 10 ). Postcodes for the Adelaide metropolitan area were sorted from most to least disadvantaged and divided into five socio-economic strata ranging from very low to very high SES. Four postcodes were randomly selected from each group, and a school from each selected postcode area was sent information about the study. Twenty school principals were contacted, and following declines to participate in the study, a further two schools were contacted to achieve a stratified spread of SES. Study information sheets, parent consent forms and questionnaires were distributed by classroom teachers to all students of participating classes.
Ethics approval was obtained from the University of South Australia Human Research Ethics Committee and the Department of Education and Children's Services. A Police Clearance Certificate was obtained by the researchers. Written consent was obtained from the school and all parents and verbal consent was obtained from each child.
To detect a medium effect size with a significance level of P < 0·05 using eight independent variables in a multiple regression analysis, the minimum sample size required was 107 participants( Reference Cohen 11 ). Of the twenty-two schools invited to take part, ten schools (45 %) agreed to participate. Study information was distributed to 521 families, of whom 216 families consented to take part, resulting in a 41 % response rate.
Materials
A parent questionnaire measured lifestyle variables, parents’ nutrition knowledge and attitudes to food. Children's nutrition knowledge was measured using the Healthy Food Knowledge Activity (HFKA)( Reference Zarnowiecki, Dollman and Sinn 12 ). Parent questionnaires were distributed with information sheets and consent forms, and parents were asked to return completed questionnaires with consent forms to the classroom teacher, who stored them in a provided sealed envelope until they were collected by the researcher. The researchers attended each school to conduct the HFKA with children. All children for whom consent had been received by parents were included; 216 responses were received from parents, and 192 paired parent and child responses were included. Reasons for excluding responses included children not completing the HFKA due to school absence, largely incomplete questionnaires, parents returning a consent form without completing a questionnaire, or the child declining to do the HFKA.
Parent questionnaire
Section 1 of the questionnaire collected general demographic information about the child and parents (Table 1). Section 2 contained questions about lifestyle variables that may influence children's knowledge of foods, including children's television viewing, takeaway meal consumption and special dietary requirements. To measure parents’ attitudes to foods they were asked to rate seven factors (taste, cost, disease prevention, speed, convenience, health and weight control) on a scale from 1 to 7 according to importance placed on these factors in making food choices for their child( Reference Gibson, Wardle and Watts 5 ). In addition, they were asked to indicate on a scale of 1 to 5 (1 = most important and 5 = least important) how important they felt it was to teach their children about healthy foods.
Table 1 Summary of demographics, lifestyle characteristics and nutrition knowledge scoresFootnote * (192 children aged 5–6 years and their parents, Adelaide, Australia, 2008)

| Parents (n 192) | |||||||
| Parent 1 | Parent 2 | Children (n 192) | |||||
| Mean or Median | sd or IQR | Mean or Median | sd or IQR | Mean or Median | sd or IQR | ||
| Age (years) | 36·2 | 6·0 | 38·0 | 6·4 | Age (years) | 5·3 | 0·46 |
| Gender (%) | Gender (%) | ||||||
| Male | 14·7 | Male | 57 | ||||
| Female | 85·3 | Female | 43 | ||||
| Number of children | 2·4 | 1·0 | Attended child care (%) | 71·4 | |||
| Two-parent family status (%) | 83·2 | Breast-feeding (%) | 82·2 | ||||
| SES (%) | Special dietary needs (%) | 3·1 | |||||
| Very low or low | 36·1 | Television viewing (%) | |||||
| Middle | 15·7 | Less than 2 h/d | 69·2 | ||||
| Very high or high | 48·2 | More than 2 h/d | 30·7 | ||||
| Weekly hours of employment | 19·9 | 17·2 | 37·2 | 15·3 | Takeaway meals (%) | ||
| Type of employment (%) | ≤1 meal/week | 87·9 | |||||
| Full time | 26·7 | 75·2 | ≥2 meals/week | 12·0 | |||
| Part time or casual | 41·9 | 18·7 | Cultural background (%) | ||||
| Not employed | 31·4 | 6·2 | Australian | 59·9 | |||
| Education level (%) | Aboriginal/Torres Strait Islander | 1·9 | |||||
| High school | 27·3 | 27·0 | Other | 38·2 | |||
| Trade or apprenticeship | 35·8 | 39·6 | Children's HFKA score | 23·0 | 3·8 | ||
| University degree or higher | 36·8 | 33·3 | |||||
| Importance of teaching child about healthy foods† (scale 1–5) | 5 | 1 | |||||
| Rank factors on importance in choosing foods for child† (rank 1–7) | |||||||
| Taste | 6 | 2 | |||||
| Cost | 4 | 3 | |||||
| Disease prevention | 4 | 4 | |||||
| Speed | 2 | 2 | |||||
| Convenience | 3 | 3 | |||||
| Health | 7 | 1 | |||||
| Weight control | 3 | 3 | |||||
| Parents’ nutrition knowledge | 72·5 | 14·8 | |||||
IQR, interquartile range; SES, area-level socio-economic status derived from home postcode; HFKA, Health Food Knowledge Activity (children's nutrition knowledge).
Parent 1 denotes parent who completed the questionnaire, parent 2 is the other parent in the family.
* Data are presented as mean and standard deviation (age, two-parent family status, nutrition questions), or as percentage (categorical variables), or as median and interquartile range (attitude questions).
† Higher median indicates greater importance placed on that factor.
Section 3 comprised a questionnaire measuring four areas of nutrition knowledge: (i) knowledge of dietary recommendations (thirteen items); (ii) sources of nutrients (seventy items); (iii) everyday food choices (eight items); and (iv) diet–disease relationships (twenty-three items)( Reference Parmenter and Wardle 13 ). Responses to each question were scored as 1 point if they were correct or 0 if incorrect, giving a nutrition knowledge score out of 114 points, with a higher score reflecting greater nutrition knowledge. Construct validity of the questionnaire has been demonstrated by significantly (P < 0·01) higher scores on all sections by third year nutrition students v. a general community sample and test–retest reliability was high (r = 0·87, P < 0·001)( Reference Hendrie, Cox and Coveney 14 ).
Healthy Food Knowledge Activity
The HFKA is a photo-based activity, designed to assess the nutrition knowledge of 5–6-year-old children. To introduce the activity, children were asked to say what they understood to be the meaning of the terms ‘healthy food’ and ‘unhealthy food’, and were subsequently provided with a standardized definition for each term, regardless of their response, to confirm they understood what the activity was about and to ensure a consistent understanding of the terms across all participants. The terms were defined as follows: ‘Healthy food is food that is good for you that you should eat a lot of’ and ‘Unhealthy food is food that is not good for you that you should only eat sometimes’. Children were then shown photos of thirty foods, one at a time, and asked to indicate if the foods were healthy or unhealthy by placing the photo with a tick or a cross (method outlined in more detail in Zarnowiecki et al.( Reference Zarnowiecki, Dollman and Sinn 12 )). Responses were scored as 1 if correct or 0 if incorrect, providing a score out of 30 for each child. Test–retest reliability of the HFKA, measured using intra-class correlations in a pilot study, was high (r = 0·84; P < 0·03)( Reference Zarnowiecki, Dollman and Sinn 12 ).
Data analysis
Postcodes were coded using the SEIFA index as a measure of area-level SES. Bivariate correlations were performed to explore associations between variables. Correlation results and theoretical information were used to construct a path diagram to examine interrelationships among variables correlated with the HFKA score. Structural equation modelling (SEM) allows for a series of interrelated dependence relationships to be examined simultaneously and to characterize previously unobserved concepts in these relationships( Reference Byrne 15 ). Missing data were imputed using multiple imputation( Reference Little and Rubin 16 ). Statistical analyses were conducted using the SPSS for Windows statistical software package version 15·0 (SPSS Inc., Chicago, IL, USA). SPSS AMOS software version 17 was used for SEM.
Results
One hundred and ninety-two children aged 5–6 years completed the HFKA, of whom 110 were boys and 70 % were 5 years old. Descriptive demographic characteristics and a summary of lifestyle variables for the sample are presented in Table 1. Results for attitudes and nutrition knowledge are also presented in Table 1.
SEM was performed on matched data from 192 children and parents in the sample. Bivariate correlations showed no evidence of multicollinearity. Multiple indices were used to evaluate model fit. The overall model appeared to fit the observed data well. The χ 2 value was not significant (minimum discrepancy divided by degrees of freedom (cmin/df) = 1·26; P = 0·29); the ratio of χ 2 to degrees of freedom was less than 2 which is desirable; normed fit index (NFI = 0·97), comparative fit index (CFI = 1·00) and adjusted general fit index (AGFI = 0·96) were greater than 0·95; and the root-mean-square error of approximation (RMSEA = 0·04) was less than 0·05, indicating good fit( Reference Byrne 15 ).
The structural equation model is shown in Fig. 1; a summary of standardized and unstandardized coefficients for this model is provided in Table 2. Parents’ nutrition knowledge was influenced by both socio-economic indicators and was a direct, positive predictor of children's nutrition knowledge (r = 0·30, P < 0·001). Parents’ education level predicted children's nutrition knowledge directly, as well as a through an indirect pathway mediated by parents’ nutrition knowledge. Home postcode indirectly predicted children's food knowledge, in a path mediated by parents’ nutrition knowledge. The relationship between parents’ attitudes to health and children's food knowledge was mediated by parents’ nutrition knowledge. Overall, although parents’ SES, education level and attitudes to health were associated with children's food knowledge, parents’ nutrition knowledge was the strongest independent predictor.
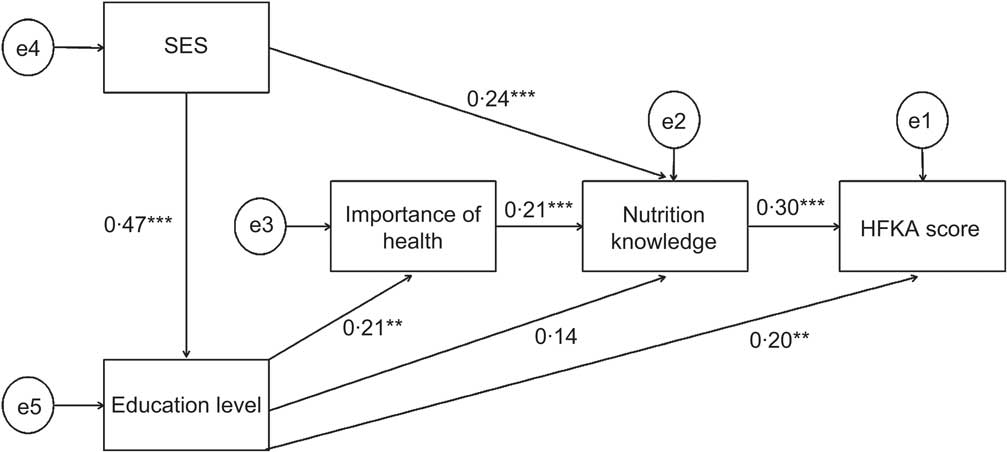
Fig. 1 Path analysis diagram for children's healthy food knowledge (192 children aged 5–6 years and their parents, Adelaide, Australia, 2008). Circles represent latent measurement errors (e1 to e5) and rectangles represent manifest variables: SES = area-level socio-economic status derived from home postcode; Education level = parents’ education level; Importance of health = importance placed by parents on teaching children about healthy eating; Nutrition knowledge = parents’ nutrition knowledge; HFKA (Healthy Food Knowledge Activity) score = children's nutrition knowledge. **P < 0·01, ***P < 0·001
Table 2 Standardized and unstandardized coefficients for the structural equation model (192 children aged 5–6 years and their parents, Adelaide, Australia, 2008)

| Observed variable | β | B | se | P |
| SES – Education level | 0·47 | 0·53 | 0·07 | 0·000 |
| Education level – Importance of health | 0·20 | 0·10 | 0·04 | 0·004 |
| Importance of health – Nutrition knowledge | 0·21 | 3·77 | 1·22 | 0·002 |
| Education level – Nutrition knowledge | 0·14 | 1·30 | 0·68 | 0·056 |
| SES – Nutrition knowledge | 0·24 | 2·49 | 0·76 | 0·001 |
| Nutrition knowledge – HFKA | 0·30 | 0·08 | 0·02 | 0·000 |
| Education level – HFKA | 0·20 | 0·46 | 0·16 | 0·004 |
SES, area-level socio-economic status derived from home postcode; Education level, parents’ education level; Importance of health, importance placed by parents on teaching children about healthy eating; Nutrition knowledge, parents’ nutrition knowledge; HFKA (Health Food Knowledge Activity) score, children's nutrition knowledge.
Discussion
In the present study, SEM determined that parents’ nutrition knowledge directly predicted children's nutrition knowledge, indicating that children of parents with greater nutrition knowledge were likely to have a better recognition of healthy v. unhealthy foods. Parents’ attitudes to healthy eating, represented by the importance that parents placed on teaching their children about healthy foods, influenced children's nutrition knowledge indirectly via parents’ nutrition knowledge. This effect was seen regardless of parents’ education and postal code (SEIFA), meaning that parents’ nutrition knowledge independently predicted children's nutrition knowledge. In a practical sense this indicates that improving parents’ nutrition knowledge may help to improve children's knowledge regardless of parents’ socio-economic position.
Relatively few studies have investigated nutrition knowledge of young children; however our results support some previous findings that parents have an important influence on older children's nutrition knowledge( Reference Gibson, Wardle and Watts 5 ). In a French study, children aged 9–11 years reported that parents were their main source of nutrition information, followed by school teachers, television and doctors( Reference Bellisle and Rollan-Cachera 17 ). Gibson et al.( Reference Gibson, Wardle and Watts 5 ) reported that 9–10-year-old children's knowledge of the fat and sugar content of food and total nutrition knowledge were positively associated with mothers’ knowledge. In the current study with younger children, parents with better nutrition knowledge and who placed greater importance on teaching their children about healthy foods were more likely to have children with better nutrition knowledge.
The manner in which children learn about nutrition knowledge is different from adult learning of nutrition. Children may learn about new foods through repeated exposure, for example exposure to a variety of fruits and vegetables in the home, which is also associated with greater acceptance, preference for and intake of these foods( Reference Birch 18 ). Young children may also develop an understanding of what are ‘normal’ eating behaviours by observing the actions of adults who are familiar to them, particularly parents( Reference Nicklas, Baranowski and Baranowski 19 ). For example, by observing that fruits and vegetables are readily available in the home and that these foods are regularly consumed by the family, children become familiar with these as a key component of the diet. This understanding can be manifested in a young child's nutrition knowledge. The converse scenario may be posited when snack foods and soft drinks are readily available and consumed in place of healthy foods. Children may also learn about food and nutrition from direct discussion of this topic with their parents. Verbal communication includes parents discussing topics with children such as which foods are liked, which foods are good for you, trying new foods and what foods to prepare for meals, with simple statements such as ‘eat it up, it's good for you’ or ‘don't eat any more of those, they're bad for you’ or more specific nutrition information such as ‘this food will make you big and strong’ or ‘this food has vitamin C’( Reference Wardle 6 , Reference Nicklas, Baranowski and Baranowski 19 , Reference Anliker, Laus and Samonds 20 ). It is noteworthy that positive messages emphasizing why food is important may have a greater influence on improving children's nutrition knowledge than negative messages such as why certain foods should not be eaten; and the quantity, quality and specificity of the information provided is significantly related to children's nutrition knowledge( Reference Anliker, Laus and Samonds 20 , Reference Contento 21 ).
In the present study, the relationship between parents’ attitudes to healthy eating and children's nutrition knowledge was mediated by parents’ nutrition knowledge, indicating the importance of attitudes in forming knowledge. Worsley( Reference Worsley 4 ) identifies knowledge as a dynamic framework of facts arising from the individual's own interests. Hence, parents’ nutrition knowledge in the present study is likely a reflection of the importance they place on this topic and their interest in health and nutrition. Parents’ attitudes are likely to impact how much information they provide to their children about food and nutrition, and how important they feel it is to discuss these topics with their children, thereby influencing children's nutrition knowledge. Gibson et al.( Reference Gibson, Wardle and Watts 5 ) showed that mother's concern for disease prevention and attitude to fruit and vegetable consumption were significant predictors of fruit and vegetable intake, indicating that parents’ attitudes can also influence children's food intake. This may be problematic for health professionals, as it may be easier to improve knowledge through education programmes than to modify attitudes. However, the act of providing information itself may alter the framework on which an individual bases beliefs, which could in turn influence attitudes( Reference Worsley 4 ).
The importance of nutrition knowledge in contributing to choices about food intake is increasingly being recognized, with studies showing associations between nutrition knowledge and eating behaviours. Mother's nutrition knowledge has been positively related to children's fruit consumption, although not with vegetable or confectionery consumption( Reference Gibson, Wardle and Watts 5 ). However, in Australian adults, nutrition knowledge was found to be a positive predictor of vegetable intake( Reference Ball, Crawford and Mishra 22 ). Likewise, Wardle et al.( Reference Wardle, Parmenter and Waller 9 ) found a significant positive relationship between nutrition knowledge and eating behaviours, with UK adults in the highest quintile for nutrition knowledge almost twenty-five times more likely to consume adequate fruit and vegetables. The pathway through which parents’ nutrition knowledge can influence children's dietary intake is through the home food environment they provide. There are many factors within the home food environment which may be determined by parents’ nutrition knowledge and attitudes to foods, particularly the types of foods available, parents’ own role modelling of eating behaviours, feeding practices and rules around eating. These factors have all been shown to predict children's dietary intake( Reference Pearson, Biddle and Gorely 23 ).
In line with previous findings for a social gradient with dietary intake( Reference Rasmussen, Krolner and Klepp 24 ), the present study found that parents from lower socio-economic areas had lower nutrition knowledge than parents from higher socio-economic areas, and children's nutrition knowledge was positively predicted by parents’ education level. Differences in nutrition knowledge across the socio-economic strata can also be found in the way parents relate children's dietary intake and health. Parents of children aged 12 years or less from areas of low SES were more likely to relate children's eating behaviours to children's physical ability to grow and play, whereas parents from areas of high SES were more likely to discuss food in terms of nutrients and risk of obesity and disease( Reference Coveney 25 ). In the current study, parents with a lower education level were less likely to feel that it was important to teach their children about healthy eating. The relationship between education level and parents nutrition knowledge in our study was not as strong as would be expected based on previous literature( Reference Parmenter, Waller and Wardle 26 , Reference Hendrie, Coveney and Cox 27 ). Given that we had a comparatively even spread of SES by SEIFA and education levels, nutrition knowledge scores may have been influenced by considerable publicity within the media about diet-related issues, including national health promotion campaigns to increase fruit and vegetable consumption (Go For 2&5™). In 2008, the South Australian Government also began to implement a campaign based on a traffic light system to improve the types of foods sold in school canteens and many schools involved in our study were implementing a morning Crunch&Sip™ snack break during which children were required to eat fruit or vegetables as a morning snack.
The present study is one of the few that have directly measured the relationship between parents’ and children's nutrition knowledge( Reference Wardle 6 ). The strengths are the sample size, which is stratified relatively evenly across all SES levels, and the validity and reliability of the survey instruments used. The study was cross-sectional and therefore it is not possible to determine whether the observed associations are causal. Generalizability of the results may be limited by a self-selection bias because participants who volunteered to take part may have a greater interest in food and nutrition; however, parents were offered remuneration in the form of a double movie pass to mitigate this. Although parent questionnaires were self-administered and unsupervised, a similar mean and distribution of scores was achieved with supervised completion of the same questionnaire in South Australia( Reference Hendrie, Cox and Coveney 14 ).
Conclusions
The present study indicates that parents can transfer knowledge about healthy foods to their young children independently of SES and educational background. These results have implications for obesity prevention programmes, suggesting that improving parents’ nutrition knowledge can result in improvements in children's nutrition knowledge regardless of SES. This finding is important because children of lower SES are at a higher risk of overweight and obesity( Reference Shrewsbury and Wardle 28 ) and are therefore particularly important targets of obesity interventions. This may help to contribute to healthier food choices throughout childhood and later in life and could be an important target for government policy development.
Acknowledgements
The study was funded by University of South Australia professional development funds. The authors declare no conflicts of interest. D.Z., N.S. and J.D. all contributed to study design and conception. D.Z. coordinated the study and collected the data. All authors were involved in various aspects of data analysis. D.Z. and J.P. conducted the SEM. D.Z. and N.S. prepared the manuscript and all authors read, edited and approved the final manuscript. The authors gratefully acknowledge the assistance of all teachers, schools, parents and children for their assistance in providing data for the study.



