


Various types of psychological therapy have been shown to be effective in the treatment of depression of which the most popular is cognitive–behavioural therapy (CBT). In a climate of limited resources and long waiting lists, it is not surprising that there is an emphasis on ensuring that psychological treatments are cost-effective. The most recent UK National Institute for Health and Clinical Excellence (NICE) guidance on depression recommends psychological therapies as one of two first-line treatment options (the other being an antidepressant) for people with persistent subthreshold depressive symptoms or mild to moderate severity depression who have not benefited from receiving a low-intensity psychosocial intervention. 1 The evidence also shows that there is broad equivalence of effect between psychological therapies (such as CBT) and antidepressants over a range of depression severities. 1 Much of the evidence about psychological therapies pertains to individual approaches. There is a paucity of evidence for group-based therapies. At present, NICE guidance acknowledges a lack of evidence for group-based therapies but recommends that group CBT should be considered for people with persistent subthreshold depressive symptoms or mild to moderate depression who have declined low-intensity psychosocial interventions. Our aim was to conduct a systematic review and meta-analysis of the efficacy of group-based psychological therapies for depression, with a particular focus on treatment in primary care and in the community.
Method
Types of studies
Randomised controlled trials (RCTs, individual or cluster randomised) based in primary care or in the community in any country were included. Quasi-randomised trials as defined by the Cochrane Collaboration Depression, Anxiety and Neurosis Review Group (CCDAN) were excluded. There were no language restrictions.
Types of participants
Adults (aged 18 or over) of either gender with a primary diagnosis of depression were included, whether or not this diagnosis had been established by criteria such as DSM–IV 2 or ICD–10 3 or confirmed by a standardised clinician assessment. Studies were included if ⩾50% of participants were classified as clinically depressed.
Studies were excluded if their inclusion criteria required any of the following: a specific comorbid physical illness, self-harm, post-traumatic stress disorder, seasonal affective disorder, eating disorder, obsessive–compulsive disorder, phobia, panic attacks, drug use, alcohol misuse, personality disorder, psychosis, schizophrenia, pregnancy, postnatal women or grief. Studies specifically of children and adolescents (under the age of 18) and hospital in-patients were excluded. Studies in which individuals were in remission from depression or when an intervention was conducted as a preventative measure for depression were excluded.
Types of interventions
We included any group intervention based on any form of psychological therapy. The definition of psychological therapy was based on that established by the CCDAN, and included CBT, behavioural therapy, cognitive therapy, interpersonal therapy, problem-solving therapy, non-directive counselling therapy, supportive therapy, psychodynamic therapy and variations thereof. We defined CBT as an intervention based on cognitive restructuring training and/or promoting behavioural change. In line with the CCDAN, we included problem-solving and self-control approaches within the CBT category.
We found no formal definition of group therapy in either the NICE guidance or related reviews, so for the purposes of this review we defined group therapy as consisting of three or more participants. Studies were included regardless of any concomitant psychotropic medication regimes.
Types of outcome measures
Outcomes were categorised as immediately post-treatment (within 1 week of end of treatment), short term (>1 week to 3 months inclusive) and medium to long term (>3 months) following completion of intervention. Any studies with a follow-up period of 1 month or less duration from randomisation were excluded.
Primary outcome
The primary outcome was clinical improvement in depression, measured using a validated self-report or interview-based measure expressed as a continuous outcome using validated depression questionnaires or rating scales. If multiple measures were used, we used clinician-rated scales such as the Hamilton Rating Scale for Depression (HRSD) Reference Hamilton4 as first choice for data extraction if available.
Secondary outcomes
We extracted data about cost-effectiveness as a secondary outcome.
Search methods
We searched MEDLINE, Embase, PsycINFO, the Cochrane Central Register of Controlled Trials and the CCDAN databases from inception until July 2010. In addition, we inspected the references of all selected studies for published reports, citations of unpublished reports and relevant review papers. To ensure all RCTs were identified, we contacted the authors of the trials included and other experts in the field.
Data management and analysis
Selection of studies
One reviewer (A.L.H.) screened the abstracts of all publications obtained by the search strategy, in order to exclude the obviously irrelevant studies. Two authors screened the remaining relevant abstracts to identify those that were potentially eligible. Using the full text of these papers, eligibility based on the inclusion and exclusion criteria was assessed independently by two authors. Disagreements were resolved by consensus and where necessary by involving a third author. Records were kept of reasons for exclusion. References were managed using Reference Manager version 12.0 on Windows.
Data extraction
We collected the items of data described above in addition to general study characteristics for each included study (online Table DS1). Data were managed using Revman software 5.01 on Windows. One author extracted data independently and a second checked these for accuracy. Disagreements were resolved by consensus and where necessary by involving a third reviewer.
Assessment of risk of bias
We assessed the quality of included studies using the Cochrane Collaboration's domain-based evaluation tool for assessing risk of bias. Reference Higgins and Green5 This consists of six questions: two assess the applicability of the randomisation process; one assesses the analysis of incomplete data; and the remaining questions cover incomplete data, selective reporting and other biases. These are answered no, yes or unclear.
Measures of treatment effect
We made the following comparisons: group-based psychological therapy intervention v. (a) usual care or (b) psychological therapy delivered individually. We made each comparison at baseline, immediately post-treatment, after short-term and after medium- to long-term follow-up.
Data synthesis
Meta-analysis was considered appropriate if there were at least three similar studies (similar in terms of patient type, setting and intervention). The purpose of the meta-analysis was to determine any differences in treatment effect of group-based psychological therapies in comparison with other standard treatments for depression in primary care or out-patient settings. Continuous data were meta-analysed using the standardised mean difference (SMD), as different psychometric scales were used in different primary studies. If heterogeneity was ⩽50%, a fixed-effects model was used. If heterogeneity was >50%, then we explored heterogeneity using subgroup analysis and then applied a random-effects model. For consistency in comparisons, a negative SMD indicates lower depression scores in the group therapy arm.
Results
The database searches resulted in 13 303 records being identified (online Fig. DS1). Following title screening for obvious irrelevance, 185 records remained. After abstract screening, 90 full text articles were read to assess their eligibility, of which 29 articles were included describing 23 original studies, with 1 follow-up paper. Reference Araya, Rojas, Fritsch, Gaete, Rojas and Simon6–Reference Rehm, Kornblith, O'Hara, Lamparsky, Romano and Volkin34 Of these, 12 studies investigated group CBT plus usual care v. usual care alone, Reference Araya, Rojas, Fritsch, Gaete, Rojas and Simon6,Reference Epstein8–Reference Yang, Hsiao, Wang, Ng, Ho and Chan18 5 studies compared group CBT v. individually delivered CBT therapy, Reference Banken19,Reference Shaffer, Shapiro, Sank and Coghlan20,Reference Teri and Lewinsohn22,Reference Wierzbicki and Bartlett24,Reference Zettle, Haflich and Reynolds25 2 studies had both of the latter comparisons in a three-arm design, Reference Brown and Lewinsohn26,Reference Schmidt and Miller27 and 4 studies published in 5 papers described comparisons for dialectical behaviour therapy (DBT) (n = 2), interpersonal therapy or self-control therapy v. usual care. Reference Lynch, Morse, Mendelson and Robins28–Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe30,Reference Bass, Neugebauer, Clougherty, Verdeli, Wickramaratne and Ndogoni32,Reference Rehm, Kornblith, O'Hara, Lamparsky, Romano and Volkin34 No quasi-randomised trials were identified.
Risk of bias in studies
The first three questions of the risk of bias tool were easy to apply to the studies in this review (Fig. 1). However, the remaining three questions posed difficulties. Due to the nature of the intervention, masking of the participants was not possible, thus all studies were scored as ‘no’. Selective reporting was difficult to assess since the majority of studies were conducted prior to the introduction of trial registration sites that contain protocols and predefined outcome measures. Thus, we assessed whether the outcome measures described in the method of the paper were reported in the results section of the paper. Unsurprisingly, all studies scored ‘yes’. The final question asked whether the studies were free of other biases. This was sometimes difficult to assess because of limitations in how studies were reported.

Fig. 1 Risk of bias. +, low risk of bias; –, high risk of bias;?, unclear risk of bias.
Because there were only two comparisons with more than two included studies, we have focused the presentation of results on these: (a) group CBT plus usual care v. usual care alone (n =14 studies) and (b) group CBT v. individual CBT (n = 7 studies). There were four further comparisons describing three other distinct psychological therapies.
Studies describing group CBT plus usual care v. usual care alone
In total, 5 out of the 14 studies described adequate sequence generation for randomisation and described details of allocation concealment. The remaining studies provided insufficient data to judge how randomisation was performed. Of the 14 studies, all but 3 included details of individuals who had dropped out. Seven studies performed intention-to-treat analysis; three were described as being analysed according to treatment arm and four gave no details.
Individual CBT v. group CBT
None of the seven studies provided sufficient information to judge whether there was adequate sequence generation or allocation concealment during randomisation. In addition, one study stated that anyone dropping out would lead to ‘replacement depending on format availability’. Reference Banken19 Three of the studies reported details of individuals who had dropped out, addressed incomplete data and how participants were analysed. For the remaining four studies there were no details on individuals who had dropped out, missing data or whether analysis was on an ‘intention-to-treat’ basis.
Remaining studies
Reporting of these studies suggested methodological weaknesses. All studies provided insufficient information to assess whether there was adequate sequence generation or allocation concealment during randomisation, with the exception of Feldman et al who described the randomisation method. Reference Feldman, Harley, Kerrigan, Jacobo and Fava29 Bolton et al stated that some participants were excluded post-randomisation ‘if their age would skew data’. Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe30 Lynch et al randomised participants using the ‘toss of a coin’. Reference Lynch, Morse, Mendelson and Robins28 All four studies described individuals who dropped out but only two described intention-to-treat analysis and the remaining two gave insufficient detail.
Study size
Another common methodological problem was the very small number of participants in some studies. Ten studies (43%) had less than 15 participants in the intervention study arm(s), eight studies (35%) had 16–50 participants per arm and only five studies (22%) had 51 or more participants per arm. It is of note that for the two main comparisons, the 14 studies of group CBT v. usual care had a total number of 1217 participants, whereas the 7 studies of group CBT v. individual CBT had a total of only 211 participants.
Effects of interventions
Depression was measured in the majority of studies using the Beck Depression Inventory (BDI) (n = 13) and eight studies used the HRSD. Some used both of these measures but as per the protocol, HRSD was used for the analysis. The remaining two studies used the Hopkins Symptom Checklist and the Geriatric Depression Scale. Data were continuous and so were subject to calculation of standardised mean differences.
Group CBT plus usual care v. usual care alone
For the 14 studies in the group CBT plus usual care v. usual care alone (total n = 1217), analysis data for depression scores showed no evidence of difference at baseline between participants for all studies combined. Reference Araya, Rojas, Fritsch, Gaete, Rojas and Simon6,Reference Epstein8–Reference Yang, Hsiao, Wang, Ng, Ho and Chan18,Reference Brown and Lewinsohn26,Reference Schmidt and Miller27 Immediately post-treatment, there was a significant treatment effect in favour of group CBT plus usual care v. usual care alone (n = 14 studies; SMD =–0.55 (95% CI –0.78 to –0.32)) (Fig. 2(a)). In a sensitivity analysis we excluded the Araya et al study, which was based on a CBT group intervention but included attention to other aspects of care as well. Reference Araya, Rojas, Fritsch, Gaete, Rojas and Simon6 This made no difference to the findings.
Few studies provided data beyond the immediate post-treatment phase. At short-term and medium- to long-term follow-up (n = 3 studies each), data suggests a positive effect of group CBT over usual care alone (SMD =–0.47 (95% CI –1.06 to 0.12) and SMD =–0.47 (95% CI –0.87 to –0.08) respectively), but confidence intervals are wide so a definitive statement is not possible (Fig. 2(b) and (c)).
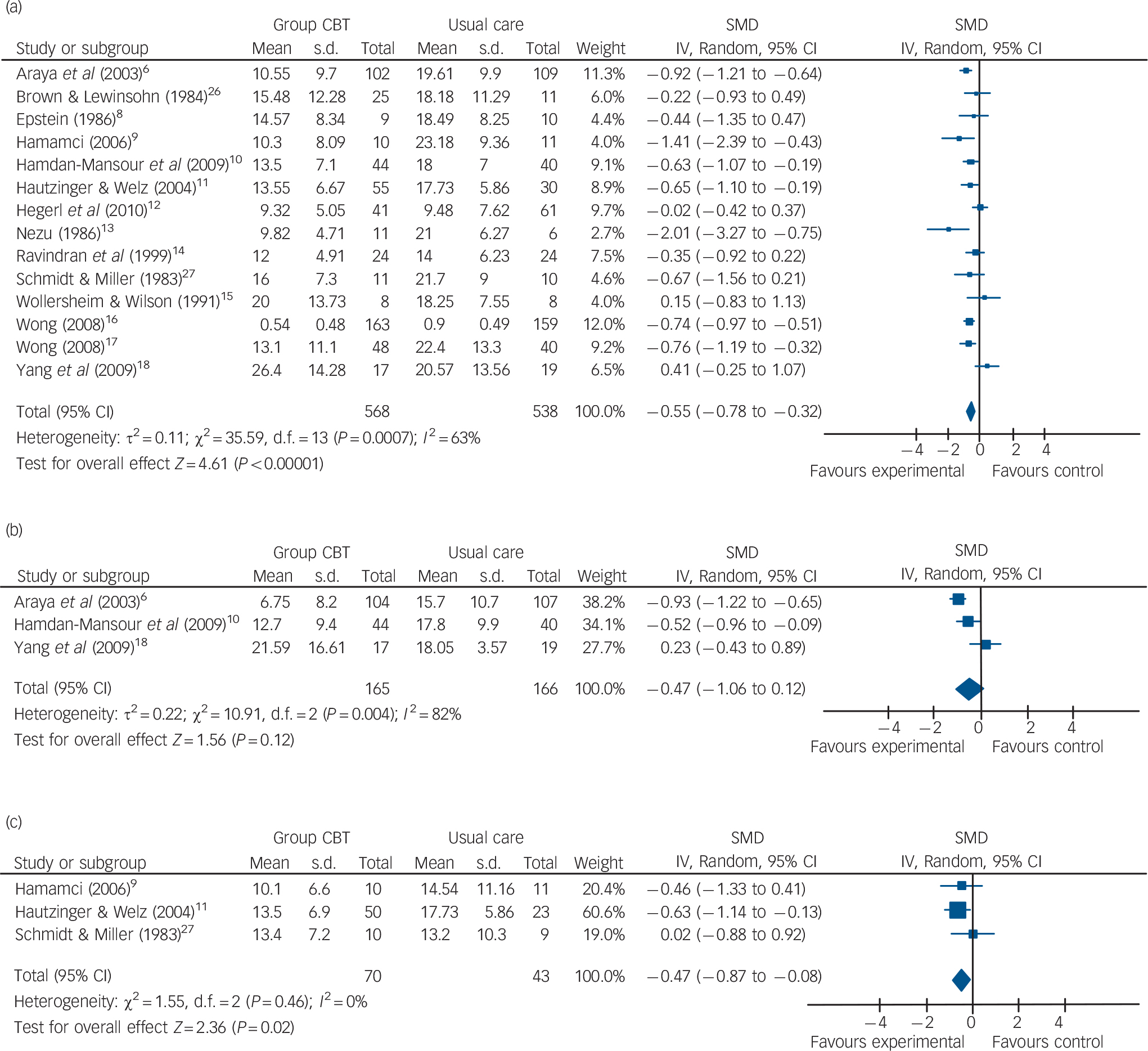
Fig. 2 Group cognitive–behavioural therapy (CBT) plus usual care v. usual care alone (a) immediate post-treatment, (b) short-term follow-up, (c) medium- to long-term follow-up. SMD, standardised mean difference.
Group CBT v. individual CBT therapy
For the seven studies in the group CBT v. individual CBT therapy analysis (total n = 211) there was no evidence of difference at baseline for all studies combined. Reference Banken19,Reference Shaffer, Shapiro, Sank and Coghlan20,Reference Teri and Lewinsohn22,Reference Wierzbicki and Bartlett24–Reference Schmidt and Miller27 Immediately post-treatment (n = 7 studies), there was a moderate treatment effect in favour of individual CBT v. group CBT (SMD = 0.38 (95% CI 0.09–0.66)) (Fig. 3(a)). Both short- and medium- to long-term follow-up data (n = 3 studies each) showed no evidence of difference in effect between group CBT and CBT delivered individually (SMD =–0.10 (95% CI –0.80 to 0.60) and SMD =–0.11 (95% CI –0.52 to 0.30) respectively (Fig. 3(b) and (c)).
Other studies
There were four studies in five papers describing comparisons for DBT (two studies), interpersonal therapy and self-control therapy with usual care (Table 1). Reference Lynch, Morse, Mendelson and Robins28–Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe30,Reference Bass, Neugebauer, Clougherty, Verdeli, Wickramaratne and Ndogoni32,Reference Rehm, Kornblith, O'Hara, Lamparsky, Romano and Volkin34 All showed a positive treatment effect for the psychological therapies over the usual care post-treatment but due to the small number of studies and their evident methodological weaknesses, no firm conclusions can be reached.
Cost-effectiveness data
Cost-effectiveness was reported by Araya et al based on their 2003 trial conducted in Chile. Reference Araya, Flynn, Rojas, Fritsch, Simon and Peters7 They reported that their group CBT intervention achieved 50 more depression-free days at 6 months than the usual care group after adjusting for age, presence of chronic disease and initial severity of depression. This improved clinical outcome was achieved at an additional cost of US$37.6 over that of usual care alone. The incremental cost-effectiveness ratio was US$0.75 that is one extra depression-free day was achieved with group CBT therapy relative to usual care at a cost of US$0.75. The authors concluded that the group CBT therapy was significantly more effective and marginally more expensive than usual care alone in the treatment of women with depression in primary care in Chile.
Siskin and colleagues Reference Siskin, Baingana and Kim33 used the data from the Ugandan study Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe30,Reference Bass, Neugebauer, Clougherty, Verdeli, Wickramaratne and Ndogoni32 cited in this review, in combination with other data from depression studies from low- and middle-income countries, to develop a Markov cohort model of depression and evaluate the health benefits and costs associated with group CBT with and without booster sessions. These calculations showed that group CBT in Uganda decreased the number of depressive episodes by 6.2% without or 15.8% with booster sessions. The incremental cost-effectiveness ratio for group CBT with booster sessions was $1.150 international dollars per quality-adjusted life year compared with no intervention. This incremental cost-effectiveness ratio for group CBT with booster sessions falls below the threshold for cost-effectiveness in Uganda.
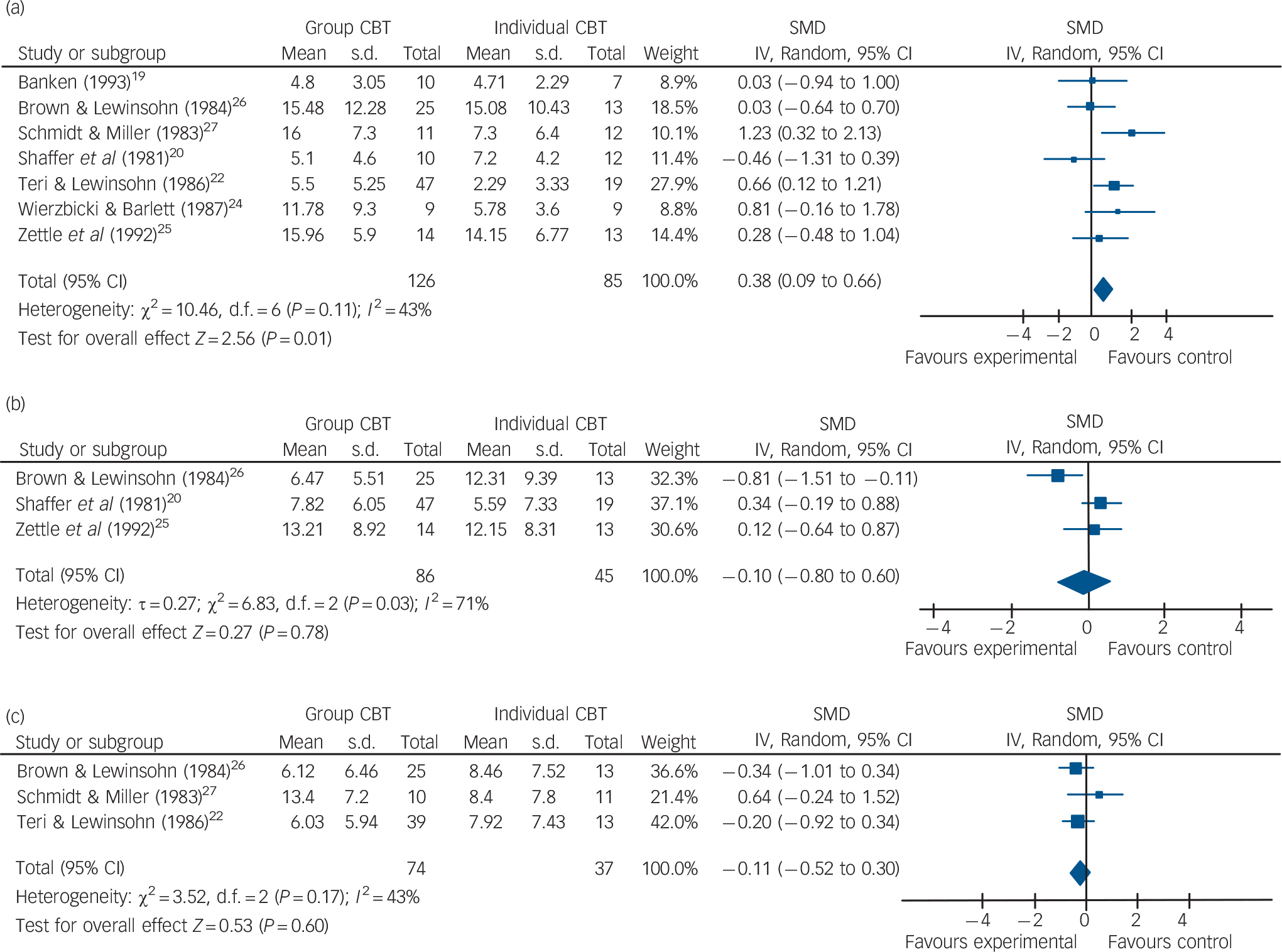
Fig. 3 Group cognitive–behavioural therapy (CBT) v. individual CBT (a) immediate post-treatment, (b) short-term follow-up, (c) medium- to long-term follow-up. SMD, standardised mean difference.
Discussion
Main findings
The purpose of this review was to assess the benefits of group-based psychological therapies compared with the main alternatives that may be available in primary care settings. Despite the Improving Access to Psychological Therapies initiative in England, the availability of individual therapy remains limited and very few people receive individual CBT in the form recommended by NICE (16–18 sessions from a trained therapist). Reference Glover, Webb and Evison35 For most people the most relevant comparison is between group-based therapy or usual primary care alone. Although acknowledging that the volume of papers is small and the quality of data variable, with many studies showing considerable risk of bias and other methodological problems, the results show that group CBT does indeed confer some immediate benefit to individuals with depression above that of usual care alone. By the short- and medium- to long-term the benefits appear to be maintained, although the evidence is less robust because of the small number of papers providing follow-up data.
Table 1 Results of studies not included in meta-analysisFootnote a
| Group cognitive–behavioural therapy | Usual care | ||||
|---|---|---|---|---|---|
| Intervention type | Mean (s.d.) | n | Mean (s.d.) | n | Mean difference (95% CI) |
| Group dialectical behavioural therapy | |||||
| Lynch et al (2003)Reference Lynch, Morse, Mendelson and Robins 28 , Footnote b | 12.93 (9.38) | 17 | 16.86 (12.93) | 17 | –3.93 (–11.92 to 3.66) |
| Feldman et al (2009)Reference Feldman, Harley, Kerrigan, Jacobo and Fava 29 | 11.30 (5.31) | 10 | 17.11 (6.23) | 9 | –5.81 (–11.04 to –0.58) |
| Group interpersonal therapy | |||||
| Bolton et al (2003),Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe 30 Bass et al (2006)Reference Bass, Neugebauer, Clougherty, Verdeli, Wickramaratne and Ndogoni 32 | 6.1 (6.3) | 103 | 20.6 (9.0) | 113 | –14.50 (–16.56 to –12.44) |
| Bolton et al (2003),Reference Bolton, Bass, Neugebauer, Verdeli, Clougherty and Wickramaranthe 30 Bass et al (2006)Reference Bass, Neugebauer, Clougherty, Verdeli, Wickramaratne and Ndogoni 32 , Footnote c | 6.1 (7.5) | 103 | 20.5 (10.1) | 113 | –14.40 (–16.76 to –12.04)Footnote c |
| Group self-monitoring | |||||
| Rehm et al (1981)Reference Rehm, Kornblith, O'Hara, Lamparsky, Romano and Volkin 34 | 9.33 (6.1) | 12 | 14.27 (7.09) | 16 | –4.94 (–9.84 to –0.04) |
a All results are for immediately post-treatment, except where indicated.
b Medium- to long-term data (6 months) were available for Lynch et al as dichotomous data: 75% v. 31% remission (group dialectical behavioural therapy v. usual), χ2=6.15, P=0.01).
c Medium- to long-term follow-up (6 months).
The studies comparing group CBT to individual CBT had a high risk of bias and very small sample sizes. Notwithstanding these limitations, these data suggest that individual CBT might be superior to group CBT in the immediate period following treatment. There was no evidence of difference at short- and medium- to long-term follow-up, but again the available data are very limited.
Relevant cost-effectiveness data are lacking but there are indications that group psychological therapies may be cost-effective, at least in low- and middle-income countries. The lack of data about cost-effectiveness of group therapy within any high-income country is striking, given that increased cost-effectiveness is a key justification for treating people in groups.
Strengths and limitations
This review focuses on studies of group CBT in the context in which it is most likely to be delivered within the National Health Service in the UK, that is in primary care and the community. Many organisations provide group-based psychological therapy, but systematic reviews of the evidence to support this development have been lacking.
Our review has a number of limitations. The vast majority of the identified studies allowed participants to take concomitant antidepressant medication, which makes it difficult to isolate the effect of the group psychological therapies alone on depression. Reference Cuijpers, van Straten, van Oppen and Andersson36 However, this is in line with the most recent guidance from NICE, which advocates a stepped-care model with a multifaceted treatment approach including medication and psychological therapies. 1 There was considerable heterogeneity between the effect sizes of different studies. This may reflect differences in severity of depression at baseline. More recent studies tended to be of better quality but, generally, the quality of studies was low and sample sizes were very small. The lack of follow-up data is a serious problem that makes it difficult to use this research to inform evidence-based policy about how best to deliver psychological therapy services. This is compounded by the lack of data about cost-effectiveness.
In their recently updated guidance on the management of depression, NICE identified five trials of group CBT v. waiting-list control or treatment as usual. 1 There was a significant effect of group CBT in lowering depression scores at end-point (SMD =–0.60 (95% CI –0.84 to –0.35)) and at 6 months follow-up (SMD =–0.40 (95% CI –0.83 to 0.02)). The National Institute for Health and Clinical Excellence concluded that there was limited evidence about group CBT but it was an option for people with persistent subthreshold depressive symptoms and mild to moderate depression who declined low-intensity psychosocial interventions. Our review updates the NICE review by including a further nine trials not identified by NICE.
The National Institute for Health and Clinical Excellence argued that group CBT was likely to be less cost-effective than low-intensity interventions but more cost-effective than individual CBT, and so was placed between them in the stepped-care model. However, NICE did not identify any trials or provide any analysis of the cost-effectiveness of group CBT v. either usual care or individual CBT. The comparison between group and individual CBT was not directly addressed by NICE but was addressed by Cuijpers et al. Reference Cuijpers, van Straten and Warmerdam37 Their review compared group psychological therapies v. individually delivered therapies in a range of settings, with the most recent included study being published in 2005. Our results support the findings of that review, with evidence for increased benefit from individually provided therapies compared with group sessions immediately post-treatment but not over a longer follow-up period.
Group-based psychological therapies are rapidly being rolled out across England in response to the Improving Access to Psychological Therapies initiative. Our systematic review has highlighted that the evidence to support this development is limited but auspicious. There will always be individuals who will not like or respond to group therapy but for those that it does suit, group therapy may be a reasonably cost-effective approach.
There are several good reasons to believe that delivering psychological therapies in groups may be appropriate. Group interventions allow people to support each other as well as to re-invigorate natural social networks. Reference Yalom and Leszcz38 Group therapy is a good way of increasing access by making it possible to treat more people from the same resource. This may also make group-based therapy potentially more cost-effective, at least from the perspective of a commissioner of services. However, it is important to bear in mind that small differences in effectiveness, as well as consideration of overall costs (of which direct treatment provision is only one part) mean that group interventions may or may not be more cost-effective than individual care at a health service or societal level. This review highlights the need for high-quality trials of group-based psychological therapy, including economic analysis, in high-income countries such as the UK in order to inform policy about provision of psychological therapies in the community.
Funding
This study was funded by South West GP Trust.






eLetters
No eLetters have been published for this article.