



Overweight and obesity rates in children and adolescents are increasing(1); in Australia, for example, it has been estimated that 25 % of those aged 5–17 years are now overweight or obese(2). The negative effects of children’s obesity and overweight are significant and include a variety of psychosocial problems alongside debilitating physical health consequences(Reference Black, Victoria and Walker3). Indeed, clusters of cardiovascular risk factors have been detected in children as young as 5 years old(Reference Ebbeling, Pawlak and Ludwig4). Due to their weight status(Reference Hayden-Wade, Stein and Ghaderi5), overweight and obese children may also experience victimisation and isolation by peers and adults(Reference Daniels, Jacobson and McCrindle6), which may lead to undesirable psychological outcomes such as depression and low self-esteem(7,Reference Puhl, Peterson and Luedicke8) . In light of these barriers, obese children often become unwilling to participate in physical activities (PA) in social settings and this maladaptive cycle of physical inactivity and social isolation is frequently observed to last into adulthood(Reference Puhl, Peterson and Luedicke8,Reference Puhl and Brownell9) .
Obesity during childhood and adolescence is both preventable and treatable through regular PA, a well-balanced diet(Reference Ebbeling, Pawlak and Ludwig4) and limited sedentary time(Reference Epstein, Paluch and Gordy10). Therefore, it is important to recognise the significant role that parents play in shaping children’s PA, dietary and sedentary behaviours. Parents are key role models for their children(Reference Bandura and Berkowitz11), and parenting styles, attitudes and behaviours are central in determining children’s PA patterns, eating behaviour and body weight regulation(Reference Golan and Crow12–Reference Sledden, Gerards and Thijs14). Parent–child interactions contribute significantly to children’s health habits and behaviours(Reference Savage, Fisher and Birch15); for instance, children display similar dietary behaviour to their parents(Reference Seagren and Terry16), and parental support for PA may contribute significant variance in children’s PA levels(Reference Davison, Cutting and Birch17,Reference Gustafson and Rhodes18) .
Researchers have, for several decades, examined the psychological (e.g. beliefs and attitudes), environmental (e.g. neighbourhood design) and interpersonal (e.g. social support) factors that might contribute to individuals’ weight and health status(Reference Jimenez-Cruz, Bacardi-Gascon and Castillo-Ruiz19,Reference Patrick and Nicklas20) . Recently though, research evidence has emerged regarding one psychological factor correlated with individuals’ health and weight status, and that may be relevant for understanding the ways through which parents contribute to their children’s health(Reference Berli, Lorentini and Radtke21,Reference Glock, Muller and Krolak-Schwerdt22) . This psychological factor refers to compensatory health beliefs (CHB), and it is to one particular type of CHB that we direct our attention to in this study.
Broadly, CHB represent cognitions that the negative consequences of an unhealthy behaviour can be compensated for thorough engaging in a healthy behaviour(Reference Knäuper, Rabiau and Cohen23) and are different from compensatory health behaviours—which represent the compensatory act in which a person engages(Reference Radtke and Scholz24) One might hold the belief, for example, that smoking two or three cigarettes each day is ‘okay’ if one is also regularly physically active. CHB originate out of an attempt to resolve the cognitive dissonance that arises when short-term goals (e.g. to enjoy hedonically pleasurable but unhealthy food, such as chocolate) conflict with one’s long-term interests (e.g. to lose weight or improve one’s health)(Reference Festinger25,Reference Rabiau, Knäuper and Miquelon26) . Accordingly, the activation of CHB allows individuals to ‘indulge’ without suffering negative affective or self-perceptual repercussions (e.g. guilt), through a logical reasoning process relying on the perception that the healthy behaviour ‘neutralises’ the unhealthy one. With particular relevance for the present study, CHB have, in some instances, been studied under the term of ‘licensing’(Reference Taylor, Webb and Sheeran27). Licensing, while applicable to other domains (e.g. moral licensing)(Reference Taylor, Webb and Sheeran27), is defined in this study as representing the belief that unhealthy behaviours (e.g. prolonged sedentary time and unhealthy food choices) are justified following, or in anticipation of, engagement in a healthy behaviour (e.g. exercise).
It has been reported that over 75 % of people endorse some kind of CHB and that the endorsement of compensatory behaviours may be associated with poorer personal health choices(Reference Moshier, Landau and Hearon28). For example, Kronick and colleagues(Reference Kronick, Auerbach and Stich29) reported that dieters who scored relatively high on endorsement of CHB also reported greater energetic intake. In a separate study targeting smoking-specific CHB, the endorsement of smoking-specific CHB correlated negatively with smokers’ readiness to cease smoking(Reference Radtke, Scholz and Keller30). Researchers have begun to study the implications of CHB—there is evidence, for example, indicating that parents’ CHB predict both intentions and behaviour towards vaccination for their children(Reference Neter, Levi and Miller31,Reference Alm and Olsen32) . However, researchers have yet to study the extent to which parents hold these beliefs regarding their children’s involvement in PA. It is possible, for example, that parents who endorse licensing for their own ‘good’ behaviour (e.g. ‘I plan to exercise, so I can have some chocolate’) might also endorse the same principle for their children (e.g. ‘my child went to swimming, so it’s okay for him/her to have confectionary and/or TV time’). Research on self-licensing has shown that these beliefs may align with poorer health choices and outcomes(Reference Moshier, Landau and Hearon28). As a result, when parents endorse the notion of rewarding their child with prolonged sedentary time and/or unhealthy food/drinks following, or in advance of exercise, this belief may align with negative health consequences for the child.
Scholars have offered interesting insight into the nature and development of CHB, and our understanding of these beliefs has improved considerably in recent years. Nevertheless, existing models and definitions are limited in scope to the rationalising of one’s own behaviour, and not the behaviour of others. Given that potential mechanisms underpinning the development and operation of CHB may differ between self- and other-focus, we sought to explore our data unguided by existing frameworks and definitions. Importantly, there are several processes through which parental licensing beliefs (regarding their children’s involvement in PA) may be problematic for children. First, it is possible that parents who endorse licensing with unhealthy food/drinks for their children around their PA may overcompensate (e.g. allow greater energetic intake than the energetic expenditure achieved during exercise), which, over time, may lead to overweight or obesity. It has been shown, for instance, that individuals tend to overcompensate in terms of acute energy intake after exercise(Reference Finlayson, Bryant and Blundell33). Second, even if parents are able to balance the energetic expenditure and intake of their children around exercise (i.e. resulting in no net energetic deficit), there may be negative health outcomes associated with unhealthy food and drink consumption that cannot be offset by exercise engagement (e.g. cholesterol levels)(Reference Hellénius, de Faire and Berglund34,Reference Daubenmier, Weidner and Sumner35) . Similarly, there may be an independent health risk associated with prolonged sedentary time that is not mitigated by exercise engagement(Reference Hamilton, Healy and Dunstan36–Reference Koster, Caserotti and Patel38). Third, if licensing beliefs are activated in advance of planned exercise, stimulating parents to relax their usual rules regarding unhealthy ‘treats’ or sedentary (e.g. screen) time may result in negative outcomes in instances where the planned activity is not actually performed. There is substantial evidence to indicate that intentions do not always translate into behaviour(Reference Rhodes and Bruijn39), meaning that licensing beliefs in advance of planned exercise may be particularly detrimental in cases when the exercise does not actually take place. Finally, it is possible that parent licensing—when it results in the regular provision of prolonged sedentary time and/or unhealthy food/drinks for children—might contribute to the formation of undesirable (and persistent) lifestyle habits among children. There is substantial evidence that automaticity and behavioural habituation occur with repeated engagement in, or exposure to, a behaviour(Reference Lally, Van Jaarsveld and Potts40,Reference Wood and Neal41) , resulting in strengthening of the stimulus-response (or cue and action) pairing. That being the case, it is possible that parent licensing beliefs might help shape unhealthy habits among children, which may ultimately come to be performed in the absence of any exercise stimuli.
To date, an emerging body of literature has begun to highlight the antecedents, nature, prevalence and consequences of personal (or self-focused) CHB. At this point, though, despite their significant role in shaping child behaviour, researchers are yet to investigate the extent to which parents may hold or adopt compensatory beliefs regarding their children’s involvement in PA. The aim of this study, therefore, was to explore parents’ perceptions about (a) the presence (or lack thereof) of compensatory beliefs regarding their children’s PA involvement and (b) the factors that might contribute to the activation of such compensatory beliefs. Based on the goal of exploring and understanding ‘lived experiences’ from the perspective of focal individuals(Reference Gratton and Jones42,Reference Schwandt, Denzin and Lincoln43) , an interpretivist approach was adopted. The interpretivist paradigm is based on concepts of epistemological constructionism (i.e. that knowledge is subjective) and relative ontology (i.e. that multiple realities exist and can be explored through human interactions)(Reference Lincoln, Lynham, Guba, Denzin and Lincoln44). Accordingly, in this investigation, we employed a qualitative descriptive approach through interviews and thematic analysis methods.
Methods
Participants
A sample of eighteen parents, with three pairs of parents from a single family unit and all other parents from separate family units (six males and twelve females; mean age = 40·8 (sd 5·4) years; age range 32–52 years; sixteen Australians, one Dutch, one New Zealand; highest level of education achieved: year-10 to post-graduate), were recruited from four different community sport or PA programmes (representing soccer, swimming and two multi-component PA programmes). Inclusion criteria were that (a) parents had a child (or children) between 3 and 12 years and (b) all parents provided written consent for the collection of data. No incentives were offered for participation.
Procedure
Participants were approached and recruited either in-person by the interviewer or through email via their respective PA programme coordinators. Potential participants were presented with an information sheet that (a) outlined the nature of the study (i.e. aims, participant involvement, benefits and possible risks), (b) emphasised the voluntary nature of participation, (c) clarified participant anonymity in any future presentation of data, (d) notified participants that they were free to withdraw from the study at any time and (e) extended an invitation for any questions to be asked. The lead author, who was also one of the interviewers, then liaised with each participant to arrange an appropriate date, time and venue to conduct a semi-structured, face-to-face interview. At the start of all interview sessions, participants were asked to provide consent and reported brief demographic information (e.g. age, gender, educational levels and age of child/children). Interviews were conducted over a 4-month period, and data saturation was deemed to be achieved at the point that no novel themes were emerging from further discussions. At the point of saturation, participant recruitment and data collection ceased(Reference Green and Thorogood45,Reference Levitt, Bamberg and Creswell46) . Interviews were conducted with a maximum of two participants per interview. Interviews were held at various locations, with consideration given to participant convenience and appropriateness of the venue. In cases when parents had multiple children within the focal age range, they were asked to discuss their perceptions in relation to one of their children, whom parents felt that they would have a ‘typical’ response to their participation in PA.
Interview guide
The lead author facilitated the interviews, with assistance from two co-authors where necessary (both of whom worked within exercise psychology and/or paediatric exercise programmes and had experience with conducting interviews). Prior to the start of the interviewing process, a semi-structured interview guide was developed to direct discussions for parents and to ensure consistency across discussions(Reference Gall, Gall and Borg47). The interview guide was reviewed by all co-authors to assess the suitability and coverage of interview questions and consisted of five broad open-ended questions framed to explore parents’ perceptions about (a) the presence (or lack thereof) of licensing beliefs regarding their children’s PA involvement (e.g. ‘Could you describe what you think and do on days that your child has been, or is going to be, physically active, compared to a day where your child is less active?’) and (b) the factors that might contribute to the activation of such licensing beliefs (e.g. ‘Could you describe the things you take into consideration when deciding about food/drinks and screen time for your child around his/her physical activity?’). Probing questions were employed when deemed necessary to clarify the meaning of a given answer, to explore additional concepts surrounding an answer and gain further explanation regarding a belief(Reference Ritchie and Lewis48,Reference Sparkes and Smith49) . At the end of the discussion, participants were invited to ask any questions about the study, offer any additional information, and provide general feedback. Interview questions can be found in online Supplementary materials S1.
Data analysis and validity
Interviews were audio-recorded, and the recordings transcribed verbatim. All audio recordings were reviewed twice by the lead author to ensure maximum accuracy of transcription. Notes of emerging themes were recorded separately to aid in the coding process. To maintain anonymity, participants were identified via code numbers (e.g. F01) and all names mentioned in the interviews were also de-identified (e.g. F01’s daughter).
Due to the interpretivist nature of the study, an inductive thematic approach was used, with data analysed using computer-assisted and thematic analysis guidelines(Reference Braun, Clarke, Weate, Smith and Sparkes50,Reference Creswell and Creswell51) . Accordingly, upon completion of verbatim transcription, all transcripts were organised and imported into NVivo qualitative data analysis software (QSR International Pty Ltd). Next, the lead author immersed himself in the data by reading through the transcripts several times and making notes of key concepts or ideas. Following this stage, meaning units, representing paragraphs, sentences and phrases containing contextually relevant information regarding the nature and antecedents of parents’ licensing beliefs for their children were identified and coded(Reference Braun, Clarke, Weate, Smith and Sparkes50,Reference Malterud52) . All codes were then grouped into an initial theme structure, whereby codes that shared the same focus were grouped according to their similarity in content. Themes were subsequently named and defined and were reviewed and cross-checked against original transcripts to ensure all themes were represented. Following this process, a ‘critical friends’ approach was used to highlight and challenge any possible weakness in the interpretation of codes and/or assignment to specific themes, and to allow for the exploration of alternative interpretations(Reference Cowan and Taylor53,Reference Smith and McGannon54) . The critical friends method involved a reflexive process whereby the first author met with members of the research team to discuss the initial coding, impression of themes and theme-to-theme relationships. During this reflexive process, the critical friends provided feedback for consideration, challenged assumptions, sought clarification and provided alternative perspectives on initial coding, without aiming to seek complete consensus. As a result of this process, some themes were redefined, reorganised, merged or deleted. Based on the approach adopted, the following judgement criteria (characterising traits(Reference Smith and McGannon54)) were considered during this process: worthiness of topic (e.g. content reflective of parental licensing beliefs), significant contribution in a practical (i.e. for parents and health practitioners) or conceptual sense (i.e. novel contribution to CHB literature) and meaningful coherence (e.g. capturing the lived experiences of parents and connection of findings with literature)(Reference Sparkes and Smith49).
Results
The interviews generated 156 pages of twelve-point, single-spaced text, with duration of interviews ranging from 14·78 to 30·87 min, and mean interview duration of 24·76 min. Ten parents were interviewed in pairs, and eight parents were interviewed alone. Codes were isolated, and themes created, when parents described their perceptions about (a) the presence (or lack thereof) and nature of licensing beliefs and behaviours regarding children’s PA and (b) the factors that might contribute to the activation of such beliefs or behaviours. In the material that follows, we present themes within these two broad categories.
Nature of parents’ compensatory beliefs
Two distinct themes emerged regarding the nature of parents’ compensatory beliefs for their children’s PA. The themes reflected (a) incidence of CHB for children (i.e. parents describing their belief, or not, in compensation, and others’ use of compensation) and (b) types of compensation (i.e. the ways in which these beliefs were employed). Themes, sub-themes and exemplar codes are presented in Table 1.
Table 1 Themes, sub-themes and example codes reflecting the nature of parents’ compensatory beliefs for their children
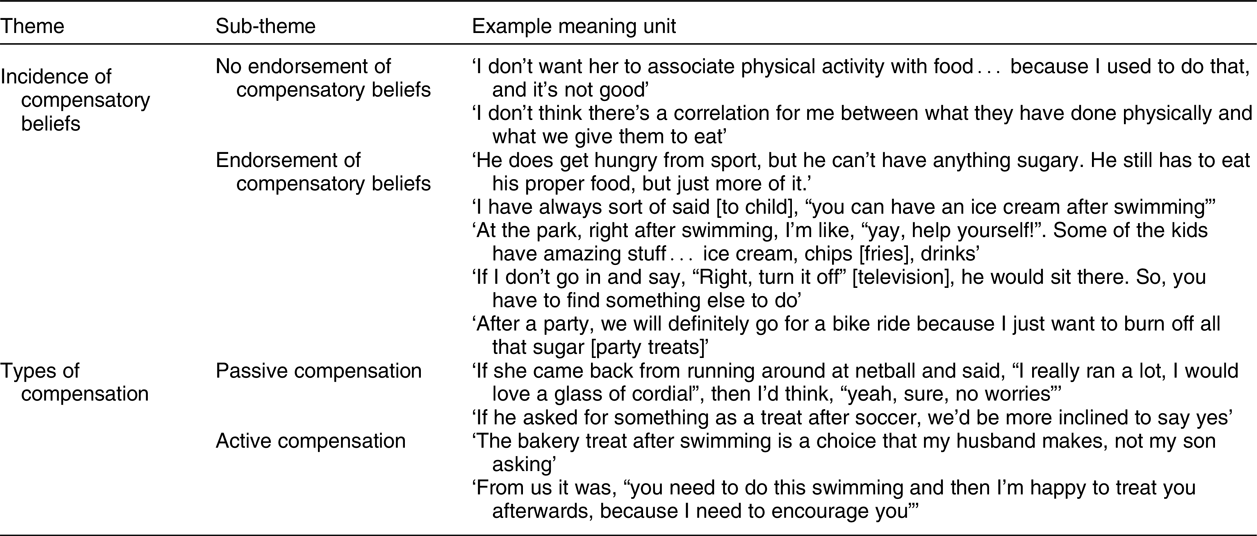
Incidence of compensatory beliefs
Within this theme, codes emerged reflecting both the endorsement and non-endorsement of compensatory beliefs, as well as examples of other parents’ use of compensation. A relatively even proportion of codes emerged that reflected the endorsement v. non-endorsement of compensatory beliefs. With respect to non-endorsement of compensatory beliefs, one parent alluded to a PA ‘cut-off’ below which point licensing was unlikely (‘My son was only active for 14 min, so I wouldn’t say “yep, you can have a Happy Meal [McDonald’s] for lunch”’). Parents also mentioned that although they may license themselves around their own participation in PA, they did not endorse the same approach for their children. One parent commented,
I compensate. If I have more than 2 glasses of wine on a Friday night, I have to run an extra kilometre on Saturday morning… but I don’t want my two kids growing up with those attitudes towards food and things.
With respect to those parents who did (at least, under some circumstances) endorse licensing around their child’s PA, the majority reported licensing with what would typically be considered unhealthy (i.e. hedonically-pleasurable, high-fat, -sugar or -salt) food rather than with extended sedentary (i.e. screen) time. One parent highlighted, for example, ‘he’s going to be running around, so I won’t worry if I’m giving him chocolate’, and another parent commented, ‘I know that at school they run around… so if, on occasion, they want to have lollies [confectionary] then I’m like, “okay, no worries”’. Several parents also provided secondary accounts of witnessing other parents licensing with unhealthy food. One parent commented, ‘One of my friends, they have a rule actually, it’s KFC after swimming all the time’. In these examples, the PA was sequenced (temporally) before the act of compensation; however, there were also some instances of the reverse sequencing whereby the licensing act took place ahead of PA (or was used to justify the need for subsequent PA). One parent explained, ‘If you have had party food, or you are going to be having those treat foods, then we would make sure we go for a bike ride around the lake afterwards’. Another parent mentioned, ‘when you add sugar in the mix with food, like an intense amount of sugar, then they need to go and run around after’.
A minority of parents who endorsed licensing with food described that they preferred to do so with the use of (what they considered) ‘healthy’ foods—by allowing their child to consume more than usual around PA, even though the ‘compensation’ might exceed their child’s energetic expenditure. One parent articulated, for example, ‘tomorrow night he will be starving after soccer… so I have made him his favourite, chicken soup. I’ve prepared an extra bowl today already, in preparation for tomorrow’. Another parent mentioned, ‘when he finishes being active, I’m quite happy for him to have as many strawberries as he likes’.
Compared with the use of food, compensation with sedentary time was not commonly described. Some parents did, however, comment on the use of sedentary time in response to PA. One parent highlighted, for example, ‘when she is tired and has had her swimming lesson… our tendency would have been to give her screen time after physical activity’. Another parent commented, ‘if he’s had a big rugby game, and he’s run around, I’ll give him some time in the afternoon, like early afternoon, to have some screen time’.
Types of compensation
We observed two distinct types of compensation, which we termed ‘passive’ and ‘active’ in nature. When describing these instances of compensation, consistent with the evidence presented above, parents again focused primarily on licensing with food, rather than with sedentary time, and any temporal specificity within these codes indicated that the majority of active and passive compensation occurred after PA.
We used the term passive compensation to characterise instances when parents described the use of compensation in response to a request from their child (rather than being initiated by the parent). One parent described, ‘with the TV, my son walked in and said, “Oh, I’ve been playing soccer”, and so my response was “yes, okay okay, I’ll let you watch it”’. Another parent commented, ‘with my son, after he has been to his swim squad, or he has done five hours of swim races, and says, “I’m starving mum… can I have some hot chips [fries]?”, I’ll say “yeah sure!”’.
We also identified a separate (and smaller) group of codes whereby parents compensated without being prompted or requested by the child; we referred to these incidents as acts of active compensation. When talking about her daughter, one parent highlighted this type of compensation,
with her, it is always like, “you need to get in the water [for swimming], so if it is going to help you to get into the water, then maybe we could go do this after”. It could be anything, could be something as simple as lollies [confectionary] at the end.
Another parent described the active compensation offered by his spouse,
one of my sons, I don’t know why, he’s a struggle to get into this multi-sport program… and he really doesn’t want to go… so, [my wife] made a deal, each time he goes, on the way home, they would call through Red Rooster [Australian fast food restaurant] and get some hot chips [fries] or something.
Reasons for compensation
Three distinct themes emerged in relation to the reasons behind parents’ belief in choosing to compensate or not. These themes were focused broadly around (a) parent considerations of their child’s physical or health status, (b) parent considerations of their child’s psychological characteristics and (c) parents’ own motivation and/or mood state. Themes and exemplar codes are displayed in Table 2.
Table 2 Themes and example codes regarding parents’ reasons for compensatory beliefs
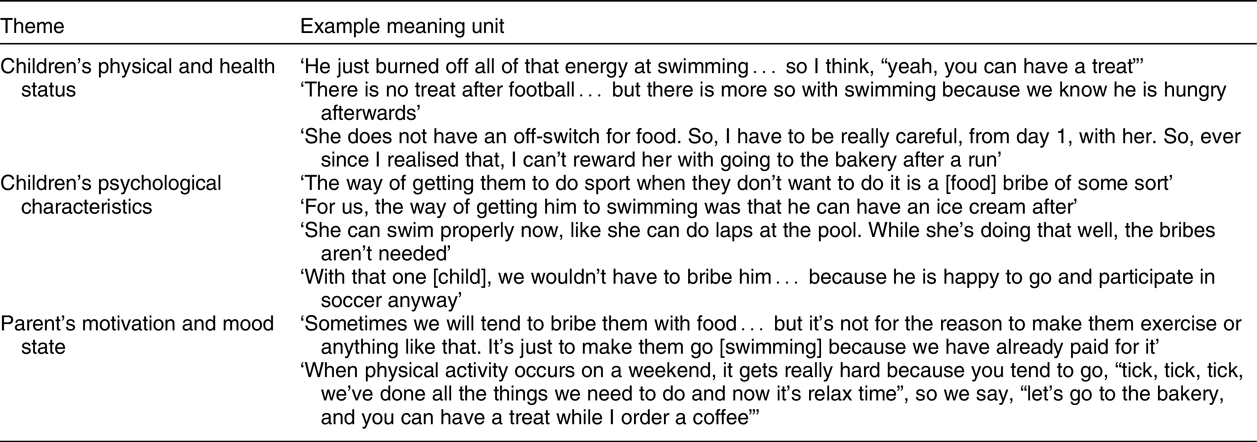
Children’s physical and health status
In this theme, parents described that their use of licensing around PA—and their endorsement (or not) of CHB in this context—was informed by their appraisals about their child’s physical and health status (e.g. their PA levels, diet and fatigue). Parents appeared to be more likely to compensate when they felt that their children had engaged in sufficient (i.e. duration or intensity) PA; one parent commented, for example, ‘if it’s a Saturday morning, and they did two hours of gym… they’re going to be exhausted, so I do let them crash [engage in sedentary time] for the afternoon’. Parents also appeared more likely to endorse unhealthy food rewards when they believed that their child was otherwise ‘healthy’ and regularly physically active. As one parent commented, ‘he will get little food treats, because at the end of the day, we are so active, we always cycle, we always do stuff’.
Children’s psychological characteristics
Codes in this theme reflected the ways parents appeared to modify their endorsement of CHB on the basis of their child’s motivation for, and mood surrounding, the PA in question, or in response to other aspects of their child’s personality. With respect to motivation, several parents described that ‘rewarding’ their child was simply unnecessary because their child enjoyed the PA in question. As one parent commented, ‘he doesn’t need much reward. He loves sports, and it’s very easy to get him to do sports… so he doesn’t really need bribery’. On the reverse, some parents endorsed CHB because they felt that a ‘treat’ or ‘bribe’ was required in order to motivate their child to participate in PA. One parent explained, ‘The thing is, he doesn’t do activities. He comes to this program, and is just being silly, he doesn’t do anything… so I have to bribe him to do the activities’. Another parent commented on the use of unhealthy treats (i.e. confectionary), ‘In the winter, it’s cold. It’s not very warm, and she just doesn’t want to get in the pool. And, we’re paying for it, so it’s like, “you are going for a swim!”. So we will tend to bribe her’.
Aside from their child’s motivation surrounding PA, some parents also appeared to take into account aspects of their child’s general nature or personality when considering compensatory beliefs. On this issue, one parent commented, ‘He’s very good at manipulating, if he knows he’s getting a treat for doing football, he’ll start to manipulate you… so, we’re very careful not to do that’. Taken together, codes in this theme appeared to indicate that CHB may be most likely when parents felt that these rewards were required for a motivational purpose and were less likely when children were (a) already happy to participate in the PA or (b) likely to use the reward for manipulative purposes in the future.
Parent’s motivation and mood state
In this theme, parents described that their compensatory beliefs were dependent, at times, upon factors associated with their own motivation or mood state. Parents noted, for example, that they were more likely to endorse compensation with unhealthy treats when they were pleased with their child’s accomplishment in PA. For example, one parent noted, ‘Compensating probably is something we do for sport… because it’s almost like we are in a good mood with him because he has done something well’. Parents also described being more likely to compensate with unhealthy food not only when they took pleasure from their child’s PA involvement but also when they took pleasure from consuming the licensed ‘treats’ together. One parent commented, for instance, ‘I do like to share it [the treat] with her, it’s something that I would also want. I like cooking, I like baking, so I’ll make cake and biscuits and things for us’.
Parents also described endorsing compensatory beliefs in cases when they (personally) felt that the PA was of practical value to their child; one parent described, ‘we are pushing to do what needs to be done with swimming. So, that’s where the bribe comes into it’. In other cases, a financial investment appeared to heighten parents’ motivation to ensure their child participated in the PA programme, which, in some cases, appeared to stimulate compensation. On this issue, one parent commented, ‘we tend to bribe them… it’s to make them go in the pool because we have already paid for it!’. Aside from compensating as a result of these considerations (e.g. due to pleasure at one’s child’s achievements, or the practical or financial value of PA), parents also cited convenience as a factor that shaped their compensatory beliefs. One parent highlighted the convenience of having unhealthy snacks nearby the PA facility, commenting, ‘we’ll buy him a packet of sweet biscuits after he’s been swimming, down at the canteen, just down there, and that’s a bit of a reward for him’ (for another example of ‘convenience’, see Table 2).
Discussion
There is a developing literature that documents the nature, antecedents and health implications associated with CHB. Researchers have demonstrated the presence of these CHB with respect to PA participation—most notably in relation to the licensing of unhealthy foods and drinks around exercise(Reference West, Guelfi and Dimmock55)—and we are also beginning to learn about the associated negative health consequences. To date though, scholarly attention in this area has been directed towards understanding the way in which individuals (do or do not) justify their own health decisions around PA(Reference Berli, Lorentini and Radtke21,Reference Kronick, Auerbach and Stich29) . Although there is evidence indicating a negative relationship between adolescents’ own CHB and intentions towards PA(Reference Berli, Lorentini and Radtke21), it is surprising, given the critical role parents play in shaping their children’s dietary and sedentary behaviours around PA, that there is little evidence regarding parents’ compensatory beliefs surrounding their child’s involvement in PA. We sought to address this research gap by eliciting information from parents as to (a) the presence (or lack thereof) of licensing beliefs regarding their children’s PA involvement and (b) the factors that might contribute to the activation of such compensatory beliefs. In doing so, we sought not only to allow parents to discuss the licensing of unhealthy foods or drinks but also to consider whether they provided extended sedentary (screen) time—another factor that is independently important for children’s health aside from PA and dietary factors(Reference Epstein, Paluch and Gordy10).
Our analyses revealed that, similar to existing perspectives on CHB(Reference Rabiau, Knäuper and Miquelon26), parents did engage in experiencing motivational conflict, which resulted in the formation of compensatory beliefs around their child’s PA participation. More specifically, although some parents appeared not to endorse such beliefs, the most common form of compensation that we observed reflected the provision of (primarily) unhealthy ‘treat’ foods, or a quantity of ‘healthy’ foods that exceeded the energetic needs of the child, following a child’s involvement in PA. Parents appeared to provide these treats in different forms—either with (passive compensation) or without (active compensation) an explicit request from their child, and typically after the child’s involvement in PA. These findings are interesting from a conceptual perspective inasmuch as they represent the first documented evidence of the different types of compensatory beliefs parents may hold around their child’s PA, and from a practical perspective insofar as they may carry important health implications for children and families. In addition, we also documented some of the reasons behind parents’ compensatory beliefs. Parents cited a range of child- (e.g. physical and psychological considerations) and self-focused (e.g. motivation) reasons for endorsing compensation, and in doing so, provided evidence to support previous findings on factors underpinning people’s self-licensing decisions and actions. Moshier et al.(Reference Moshier, Landau and Hearon28), for example, presented evidence that individuals tend to license with food around PA due to a desire for reward, recovery or relief (see, e.g., the child physical and psychological factors that were cited as reasons for parent compensation in this study). Given that we provide some of the first evidence regarding the nature and antecedents of parent compensatory beliefs around children’s PA, in the material that follows we reflect upon what we consider to be some of the more noteworthy conclusions—and associated future research directions—stemming from these findings.
First, we found it noteworthy that some parents described that they did not endorse licensing beliefs around their child’s PA involvement. It is entirely possible that these parents did indeed not modify their dietary and sedentary behaviour practices in response to their child’s involvement in PA. Our findings also point to another potential explanation, however, that should be examined further in future work. Specifically, although some parents noted that they did not endorse licensing beliefs, the vast majority of the parents interviewed in this study provided several accounts of other parents engaging in licensing with unhealthy food or drinks. This potential willingness to share licensing examples from other families, but not one’s own family, emphasises the sensitive nature of this topic, but might also be due (at least in part) to parents not being explicitly aware of their own behaviour around this issue, or perhaps parents wanted to portray a socially desirable (e.g. healthy) image of their family. In addition, despite our attempt to focus on licensing from both a dietary (e.g. unhealthy treats) and sedentary behaviour (i.e. screen time) perspective, parents focused very little attention on the use of extended screen time for their children around PA. In much the same way that parents may not always be explicitly aware of their dietary decisions, allowing one’s child to relax in front of a screen for longer than usual may not be particularly memorable or accessible for parents when attempting to recall incidents (particularly in comparison with, e.g., driving through a fast-food restaurant on the way home from PA). With this issue in mind, there may be interesting methodological approaches that could be used in the future to allow for greater insight into these licensing reactions. One such approach for addressing this issue might be to develop or use nonconscious (e.g. implicit attitude(Reference Glock, Muller and Krolak-Schwerdt22)) tests for parents to examine their implicit associations(Reference Cameron, Reed and Ninnemann56) between children’s PA and licensing (both dietary and sedentary) responses. In addition, it might also be valuable to employ repeated assessment protocols (e.g. ecological momentary assessment(Reference Li, Lansford and Dubow57)) that enable parents to provide insight into the ways in which, e.g., children’s PA and parent decisions around screen time are linked.
Second, we were intrigued by some evidence of a perceptual ‘cut-off’ that some parents appeared to employ in order to gauge the acceptability of licensing with unhealthy food. As might be expected, we observed that parents were more likely to endorse compensatory beliefs in the form of unhealthy treats when they felt that their child had ‘earned’ such foods. In the future, experimental research may be suitable to examine the exercise characteristics and perceptual factors that contribute to the setting of any licensing cut-off. There exists evidence to suggest that exercise modalities can impact adults’ own compensatory decisions(Reference Inauen, Radtke and Rennie58), and it would be interesting, for example, to examine how different exercise modalities (e.g. duration and intensity) might play into parents’ compensatory decisions for their children. It would be fascinating to also identify whether appraisals about psychological factors might also shape the point at which any cut-off is set. Researchers might examine, for instance, whether a given ‘dose’ of PA for children is more likely to result in parent compensation (with unhealthy treat food) when the child is assumed to have been highly anxious or unmotivated (relative to low anxiety or high motivation) regarding the performance of the activity. Similarly, large-scale observational studies might also provide insight into the variation in cut-offs adopted by different parents/families, indicating whether some parents require only minimal PA with limited energy expenditure to ‘qualify’ for compensation, while others require relatively more sustained or intense activity. Such work could also shed light on the potential moderators of such variation (e.g. parent PA and fitness levels, parent dietary behaviour and child weight).
Third, although active compensation can lead to an increase in PA engagement, incentivising engagement through the promise of unhealthy food (prior to participation in particular) may be counterproductive. Especially in instances when external tangible rewards are perceived as controlling in nature, these strategies can undermine children’s intrinsic motivation for PA (e.g. enjoyment of PA(Reference Fenton, Duda and Barrett59)). Indeed, many parents cited that when their child highly enjoyed his/her PA participation, there was little need to offer rewards in the form of unhealthy snacks or extended screen time. As a result, it is possible that the use of these ‘bribes’ (as many parents referred to them) may create a negative motivational ‘spiral’ insofar as children strive to reach PA achievements predominantly for the treat or reward that is on offer, rather than for the enjoyment or value associated with that achievement.
Finally, although most licensing acts took place after the PA bout, we did observe some evidence that licensing may occur in advance of planned PA. This particular sequencing may have important practical and psychological implications and warrants further attention. From a practical perspective, in instances when PA is subsequently performed as planned, there is likely little difference in one’s overall net position regardless of whether licensing occurs before or after PA. In light of the well-established intention-behaviour gap, though(Reference Rhodes and Bruijn39), it is possible that the intended PA may not be carried out. In such instances, the provision of unhealthy treats in advance of a planned PA session that does not actually eventuate may be problematic from a health perspective (if this pattern is repeated often). Meanwhile, it would be interesting to study whether the provision of unhealthy treats consistently in advance of PA might change children’s views on (i.e. motives for) their participation in PA. To illustrate, consider the scenario where parents provide unhealthy food relatively frequently in advance of planned PA, and begin to ‘pair’ the provision of such food with the need to subsequently be active. In such a scenario, the way parents communicate to their child about PA may be less than optimal and might be accompanied by messages that are perceived by children as guilt-inducing or coercive (e.g. ‘we all treated ourselves to that cake at lunchtime, but now we have to get out and be active to work it off’). It would be interesting to study whether such a licensing arrangement—if it is present in any households—could be associated with heightened introjection (e.g. guilt) and external regulation for PA among children.
The findings of this investigation provide an interesting first step into studying the nature and psychological underpinnings of parent compensatory beliefs surrounding their children’s PA participation. The contributions of the study, though, should be considered alongside important limitations. First, our design precluded drawing robust conclusions relating to the ways in which cultural, social desirability, personality and demographic factors (e.g. nationality, child age, number of children, marital and socio-economic status) might moderate parents’ compensatory beliefs; future efforts to consider such questions appear worthwhile. As one example, it would be interesting—given that we recruited parents of children ranging in age from 3 to 12 years—to use a quantitative approach to test how child age might influence parents’ compensatory beliefs. In addition, we did not aim to examine the health or behavioural outcomes (for child or parent) associated with these beliefs. As such, although we presented evidence for the nature and antecedents of parent compensation, we cannot yet be confident that these beliefs will have similar effects to those that have been begun to emerge in the research on personal or self-licensing among older cohorts(Reference Amrein, Rackow and Inauen60–62). We encourage researchers to begin to chart the correlates of parent compensatory beliefs and, in doing so, examine the extent to which children develop perceptions about licensing that may mirror those held and displayed by their parents.
Conclusions
In closing, we feel it is important to qualify briefly the evidence presented and discussed above. Our treatment of parents’ compensatory beliefs surrounding their children’s PA is not intended to appear critical of parents and their child-rearing practices. Indeed, all of the parents who participated in this study should be recognised for the substantial time and effort devoted to enrolling their children in, and transporting them to and from, various PA programmes. Moreover, we are not seeking to advocate that the provision of (often highly sought after) foods, drinks and screen time to children should be eliminated altogether from a child’s development; there is little doubt that these licensing behaviours, in moderation, are typically enjoyable for children (and likely, parents too) and help contribute to the richness of family life. However, the literature that has developed regarding CHB among older cohorts does indicate that there may be adverse health consequences associated with these patterns of thought and behaviour(Reference Storm, Reinwand and Wienert61), and so our hope is simply that these findings will provide the impetus for increased research attention to be directed towards this unique and interesting form of compensation. From a practical perspective, these findings may help us better understand, and better prevent, the unhealthy beliefs and habits that may form for parents around their children’s involvement in PA.
Acknowledgements
Acknowledgements: None. Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: None. Authorship: K.H.L. was involved in the collection, analysis and interpretation of interview data, drafting and revision of the manuscript, and submission of the manuscript. J.A.D. was involved in conceptualising and designing the study, assisted in data collection and review of data interpretation, and revisions of the manuscript. A.L.T. was involved in study design, reviewing of data, and was involved in the preparation of manuscript. J.C.N. assisted in the analysis and interpretation of data, and the preparation of the manuscript. G.H. assisted in data collection, analysis and interpretation of data, and preparation of the manuscript. D.F.G. was involved in the planning, data interpretation and preparation of the manuscript. K.J.G. was involved in planning, data interpretation and preparation of the manuscript. B.J. was involved in conceptualising and designing the study, assisted in data collection, analysis and review of data interpretation, and revisions of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human participants were approved by the Human Research Ethics Committee at the University of Western Australia. Written informed consent was obtained from all subjects.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020002554




