


Dietary intakes during the periconceptional and pregnancy period have been shown to influence pregnancy outcomes such as fetal growth, preterm delivery and congenital anomalies, the morbidity of the offspring later in life and the well-being and quality of life of the mother herself( Reference Chatzi, Mendez and Garcia 1 – Reference Okubo, Miyake and Sasaki 3 ). However, many adult and adolescent pregnant women fail to meet key nutritional targets, even in industrialized countries( Reference Hure, Young and Smith 4 , Reference Moran 5 ), highlighting the need to understand key determinants of the quality of maternal diet during gestation. The study of specific dietary components may have the drawback of not taking into account the interactions between nutrients and food synergies( Reference Jacobs and Steffen 6 ). Alternatively, assessment of overall dietary intake and its quality in order to examine its effect on disease risk has gained interest over the last years. Evaluation of diet as a whole might represent more accurately food and nutrient intakes and their global effect on health outcomes( Reference Hu 7 ).
The traditional Mediterranean diet refers to the dietary pattern in the Mediterranean olive grove areas at the beginning of the 1960s( Reference Willett, Sacks and Trichopoulou 8 ), characterized by elevated intakes of plant foods such as fruits and vegetables, bread and cereals (primarily whole grain), legumes and nuts, low to moderate amounts of dairy products and eggs, and only small amounts of red meat. However, the Mediterranean diet presents regional variations derived from the same dietary pattern, influenced by various socio-cultural, religious and economic factors( Reference Bach, Serra-Majem and Carrasco 9 ). The Mediterranean diet has consistently been reported to have favourable effects on both physical and psychological health outcomes in pregnant women and the general population( Reference Chatzi, Mendez and Garcia 1 , Reference Timmermans, Steegers-Theunissen and Vujkovic 10 , Reference Trichopoulou, Costacou and Bamia 11 ).
Previous studies have shown that involvement in the neighbourhood during adolescence and high social capital in rural residents are highly associated with consumption of fruit and vegetables( Reference Johnson, Sharkey and Dean 12 , Reference Morgan and Haglund 13 ). In addition, there is adequate evidence for a link between social network structure, social capital and patterns of obesity( Reference Christakis and Fowler 14 – Reference Moore, Daniel and Paquet 16 ). Thus the assessment of social capital and social functioning is of importance in order to maximize the effectiveness of nutrition-related interventions in pregnant women, a potentially vulnerable population group. In this context, the possible effects of social capital on adherence to the Mediterranean diet during pregnancy are not fully understood.
Social capital theory argues that social networks, trusting relationships and reciprocal social exchanges are key determinants for the health and well-being of populations( Reference Kawachi, Subramanian and Kim 17 , Reference Kritsotakis and Gamarnikow 18 ). Proposed mechanisms for this effect include exposure to health-related behaviour norms and attitudes, psychosocial mechanisms such as self-esteem and sense of obligation, and reciprocal social relations through which individuals secure access to information, material assets and personal support, otherwise inaccessible( Reference Hystad and Carpiano 19 ). Social capital has two distinctive attributes that affect health outcomes in different ways( Reference Kawachi, Subramanian and Kim 17 ): cognitive and structural. Cognitive social capital refers to perceptions, beliefs and feelings (e.g. trust, reciprocity, tolerance) while structural social capital explores what people actually do and how they behave in their social environment (e.g. participation, networks).
The aim of the present paper is to estimate the associations of individual maternal social capital and its subscales with adherence to the Mediterranean diet during pregnancy. Our hypothesis is that higher maternal social capital will be associated with higher Mediterranean diet adherence.
Methods
The Mother–Child Cohort in Crete (Rhea Study)
The Rhea Study is a mother–child cohort that examines prospectively a population-based sample of Greek and immigrant pregnant women and their children in Crete, Greece. The study protocol has been summarized previously( Reference Chatzi, Melaki and Sarri 20 , Reference Kritsotakis, Vassilaki and Chatzi 21 ). The ethical committee of the University Hospital in Heraklion, Crete, approved the study and all participants provided written informed consent.
Participants
Women were recruited from four prenatal clinics at the time of the first major ultrasound examination, around week 15 of gestation or before, for one year beginning in February 2007( Reference Chatzi, Melaki and Sarri 20 ). In total, 419 women were eligible for inclusion in the present analysis, having complete information on the social capital questionnaire and dietary intake in pregnancy. Fourteen women with multiple pregnancies and twenty-eight women with implausible values for total energy intake (outside the range of 4184–16 736 kJ/d (1000–4000 kcal/d)) were excluded( Reference Davey, Spencer and Appleby 22 ). Hence, a cohort of 377 women was available for analysis.
Data collection
Dietary patterns during pregnancy (FFQ)
The Rhea FFQ was administered in week 14–18 of gestation, assessing dietary habits over pregnancy( Reference Chatzi, Melaki and Sarri 20 ). The Rhea FFQ is a semi-quantitative questionnaire, containing 250 food items with the following components: intake frequency, dietary supplements, information on organic food consumption, different types of vegetarianism, dietary changes due to pregnancy and conditions of pregnancy that could affect diet and food intake (nausea, vomiting, etc.). The 250 food items recorded in the FFQ were aggregated into seventeen food groups, e.g. ‘fish and seafood’, ‘dairy products’, ‘pulses’, ‘vegetables’, ‘nuts’, etc.( Reference Chatzi, Melaki and Sarri 20 ). For each food item, participants were asked about both the frequency of consumption and the average portion size. The exact frequency of consumption was given per day, per week and/or per month, depending on the food item. Photographs were used to visualize small, medium and large portion sizes for each food item and respondents had to choose one out of three pictures. The intake frequency for each food item was converted to the average daily intake for each participant.
Mediterranean diet score
To evaluate adherence to the Mediterranean diet during pregnancy, we used a scale applied in a large cohort study( Reference Trichopoulou, Costacou and Bamia 11 ). For beneficial components (vegetables, legumes, fruits and nuts, cereals, fish and seafood, dairy products), women whose consumption was below the cohort-specific median were assigned a value of 0 and women whose consumption was at or above the median were assigned a value of 1. For components presumed to be detrimental (meat, including all types of meat), women whose consumption was below the median were assigned a value of 1, whereas women whose consumption was at or above the median were assigned a value of 0. For fat intake (the eighth food category), we used the ratio of daily consumption of monounsaturated lipids to saturated lipids. Because the index had been developed for adults and our study population involved pregnant women, we presumed dairy products to be protective and not detrimental dietary compounds, and did not include alcohol consumption in the index( Reference Chatzi, Melaki and Sarri 20 , Reference Chatzi, Torrent and Romieu 23 ). The total Mediterranean diet score ranged from 0 (minimal adherence to the Mediterranean diet) to 8 (maximal adherence).
Social capital questionnaire
Maternal social capital was assessed by the Social Capital Questionnaire (SCQ)( Reference Onyx and Bullen 24 ). The SCQ has been validated in Greece (SCQ-G) and comprises a general Total Social Capital factor, as well as six factors in thirty-six questions( Reference Kritsotakis, Koutis and Alegakis 25 ): (i) Participation in the Local Community; (ii) Feelings of Safety; (iii) Family/Friends Connections; (iv) Value of Life and Social Agency; (v) Tolerance of Diversity; and (vi) Work Connections. Higher scores on a 4-point Likert-type scale indicate more social capital. The psychometric results support deriving a single total score from the scale as well as a score for each separate factor by adding the scores of the questions that best define each factor( Reference Kritsotakis, Koutis and Alegakis 25 ). In the present analysis, the four questions of the factor Work Connections and one of the factors of Value of Life and Social Agency relating to work were excluded because almost half of the study participants were not working when completing the questionnaire. Thus, thirty-one social capital questions were included in the analysis.
Participation in the Local Community (e.g. Active member of a local organization or club) measures structural social capital. Value of Life and Social Agency (e.g. Local community feels like home), Feelings of Safety (e.g. Feel safe walking down the street after dark) and Tolerance of Diversity (e.g. Enjoy living among people of different lifestyles) measure cognitive social capital.
The SCQ-G was generally completed after the dietary assessment (in most cases up to 6 weeks after the FFQ interview). However, there is evidence to suggest that the cognitive features of social capital (trust, tolerance of diversity) do not change in such a short period of time( Reference Kritsotakis, Koutis and Alegakis 25 ). Regarding the structural characteristics (participation), the SCQ-G mainly assesses what has happened during the last 3 years.
Potential confounders
The following variables were included as confounders as they have an established or potential association with maternal social capital or Mediterranean diet score during pregnancy: maternal age; maternal ethnic origin (Greek/non-Greek); maternal education (low level, ≤6 years of school; medium level, >6 years of school but ≤12 years that are typically needed prior to attending university; high level, university or technical college degree); marital status (married or engaged/other); parity (multiparous/primiparous); working status (yes/no); residence area (urban/rural); physical activity before pregnancy (yes/no); smoking during pregnancy (non-smoker/ex-smoker/smoker); housing tenure (owned/rented); house type (flat/detached); number of rooms in the house; total area of the house (in m2) and maternal energy intake (kJ/d (kcal/d)).
Statistical analyses
Spearman’s ρ correlation coefficient was used to estimate the strength of the association between the SCQ-G and its subscales with adherence to the Mediterranean diet. Bivariate associations between the SCQ-G and categorical variables were studied by using non-parametric statistical methods (Mann–Whitney U and Kruskal–Wallis tests). One-way Fisher’s least significant differences test was used to identify differences between SCQ-G categories and Mediterranean diet score. To explore possible variations of the scale in this sample compared with the general population, we conducted internal reliability tests (Cronbach’s α) for the thirty-one questions of the SCQ-G.
We then performed linear regression analyses to estimate the association between maternal social capital and the outcomes of interest after adjustment for confounders. Estimated associations are described in terms of β coefficients and 95 % confidence intervals (linear regression models). Potential confounders related to both social capital (total or any of the subscales) and the outcomes of interest in the bivariate associations with P<0·05 were included in the multivariable models, except for maternal age and maternal education that were included a priori in all analyses. Moreover, we adjusted for total energy intake in all regression models using the residual method.
Separate models were built having Total Social Capital and each one of the social capital subscales as the exposure. Effect modification was evaluated using the likelihood ratio test. Generalized additive models were applied to explore the shape of the relationships between Total Social Capital and the Mediterranean diet, after adjustment for confounders (P gain defined as the difference in normalized deviance between the generalized additive model and the linear model for the same predictor <0·05).
Effect modification by maternal education, physical activity before pregnancy, residence and total area of the house was assessed through inclusion of the interaction terms in the models (statistically significant effect modification if P<0·05) and stratified analyses.
All hypothesis testing was conducted assuming a 0·05 significance level and a two-sided alternative hypothesis. Statistical analyses were performed using the statistical software package IBM SPSS Statistics 19.
Results
In the reliability tests, Cronbach’s α was 0·83 for the whole SCQ-G. Both Participation in the Local Community and Feelings of Safety had Cronbach’s α of 0·71. Value of Life and Tolerance of Diversity scales had acceptable α values of 0·66. The Family/Friends subscale (two questions) had a low α value of 0·29 and was excluded as a separate subscale in the subsequent analyses. Scales with Cronbach’s α values over 0·60–0·70 are considered to have robust internal reliability properties and can be treated as separate subscales in statistical analyses( Reference Nunnally and Bernstein 26 ).
Table 1 summarizes the demographic characteristics of the women and their relationship with Mediterranean diet scores. The majority of the participants were of Greek origin, married, with a medium or high level of education and residing in urban areas. The women included in the analyses were similar to non-participants and those excluded from the analyses, except that the former were more likely to be of Greek origin and have higher education. They were also more likely to smoke less and be more physically active before pregnancy (results not shown).
Table 1 Population characteristics and associations with Mediterranean diet score in the Rhea Mother–Child Cohort (n 377) in Crete, Greece
Statistical differences based on the Mann–Whitney U test for two independent samples, Kruskal–Wallis one-way ANOVA by ranks and Spearman’s ρ correlation coefficient.
Mediterranean diet score in relation to social capital and its subscales are presented in Table 2. Women reported significantly higher Mediterranean diet scores with increasing Total Social Capital in univariate analysis. The same was true for the subscale Participation in the Community.
Table 2 Associations between social capital and Mediterranean diet score in the Rhea Mother–Child Cohort (n 377) in Crete, Greece; univariate analysis
Ref., reference category.
Social capital has been classified as follows: the upper 10 % as the high social capital group, the middle 80 % as the medium and the lowest 10 % as the low social capital group.
* P value of one-way Fisher’s least significant differences test.
† P value of Kruskal–Wallis one-way ANOVA by ranks.
Table 3 presents the estimated associations between social capital as a continuous scale and Mediterranean diet scores after adjusting for confounders. Total Social Capital and Tolerance of Diversity were positively associated with Mediterranean diet scores (β coefficient=0·02, 95 % CI 0·00, 0·04 and β coefficient=0·17, 95 % CI 0·03, 0·30, respectively). Participation in the Community was marginally significant in the adjusted model (β coefficient=0·04, 95 % CI −0·01, 0·08).
Table 3 Associations between social capital as continuous scales and Mediterranean diet score in the Rhea Mother–Child Cohort (n 377) in Crete, Greece; multivariable linear regression models

β, β coefficient.
* All crude models were adjusted for total energy intake during pregnancy.
† Also adjusted for maternal age, maternal education, physical activity before pregnancy, residence and total area of the house in m2.
Analyses having the Mediterranean diet score as a continuous outcome variable and social capital as a three-category exposure variable are presented in Table 4. High maternal social capital was associated with an increase of almost 1 point in Mediterranean diet score (highest v. lowest group: β coefficient=0·95, 95 % CI 0·23, 1·68), after adjustment for confounders. An analogous dose–response effect was noted for the scale Tolerance of Diversity (highest v. lowest group: adjusted β coefficient=1·08, 95 % CI 0·39, 1·77).
Table 4 Associations between social capital as three-category exposure variables and Mediterranean diet score in the Rhea Mother–Child Cohort (n 377) in Crete, Greece; multivariable linear regression models

β, β coefficient; Ref., reference category.
Social capital and subscales have been classified as follows: the upper 10 % as the high social capital group, the middle 80 % as the medium and the lowest 10 % as the low social capital group.
* All crude models were adjusted for total energy intake during pregnancy.
† Also adjusted for maternal age, maternal education, physical activity before pregnancy, residence and total area of the house in m2.
Generalized additive models examining the shape of the relationships between maternal social capital and Mediterranean diet scores (Fig. 1) showed no significant departures from linearity (P gain=0·099).
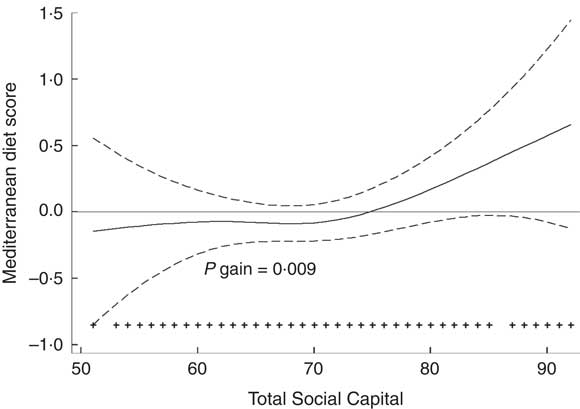
Fig. 1 Lowess smoothing of the adjusted association between Mediterranean diet score and Total Social Capital in the Rhea Mother–Child Cohort (n 377) in Crete, Greece (++++, observation of Total Social Capital; ——, spline; – – – –, 95 % confidence intervals). Predicted values were estimated by restricted quadratic spline models, adjusted for maternal age, maternal education, physical activity before pregnancy, residence and total area of the house in m2
Discussion
The present cross-sectional study reported the associations of individual social capital during pregnancy with adherence to the Mediterranean diet. We evaluated cognitive and structural social capital dimensions, i.e. Total Social Capital, Participation in the Community and Tolerance of Diversity. Consistent with our research hypothesis, we concluded that women with higher social capital had higher adherence to the Mediterranean diet during pregnancy. Similarly, the cognitive social capital subscale Tolerance of Diversity showed a positive dose–response relationship with Mediterranean diet adherence. A marginal effect was noted for Participation in the Community, a structural dimension of social capital. All associations were adjusted for a wide range of possible confounding variables and established measurement tools assessed both social capital and Mediterranean diet score.
Our findings support the relationship between social capital and nutrition behaviours noted in prior studies( Reference Johnson, Sharkey and Dean 12 , Reference Moore, Daniel and Paquet 16 ). It may be the case that women with high social capital (a higher sense of trust, respect and reciprocity) may exhibit a higher sense of obligation to themselves and others, including their unborn child, which results in an increased concern about diet and health outcomes. This concern may then result in engagement in proactive health- and nutrition-related activities, a finding confirmed in cohesive family units in the general population( Reference Moxley, Jicha and Thompson 27 ). In current literature, there is robust evidence that the quality of food purchases is highly dependent on socio-economic status, the income of consumers and the availability of healthy food options( Reference Darmon and Drewnowski 28 ). Healthy nutrient-dense foods are far more expensive sources of energy than the less healthy energy-dense diets( Reference Darmon, Darmon and Maillot 29 ). To limit the possibility that the association of social capital with Mediterranean diet is confounded by income or availability of healthy food choices, we adjusted for different indicators of socio-economic status (e.g. education, total area of the house in m2) and place of residence (urban/rural); the results remained largely unchanged or were more supportive to our hypothesis. Social capital may provide the motivation, by means of obligation, reciprocity and self-control, to invest in future family health.
There is a vast literature suggesting that experiencing different types of personal or institutional discrimination has detrimental effects on health, including nutritional risk( Reference Grollman 30 , Reference Nadimpalli and Hutchinson 31 ). In the present study it was revealed that intolerance of diversity had negative associations with the Mediterranean diet score and thus the healthy dietary patterns of the participants. What is of importance is that the one who embodies and manifests the health-damaging behaviour is not the exposed individual, but rather the exposé, the one who expresses these negative feelings and attitudes towards others. If intolerance of diversity is an internalized attitude, a pattern of life, and this intolerance extends to lifestyle, including diet, then it would be very difficult for individuals to adjust their daily diets to the recommended nutritional intake, especially in places with different nutritional norms. Konttinen et al. ( Reference Konttinen, Sarlio-Lähteenkorva and Silventoinen 32 ) examined which motivational factors account for the education and income inequalities in dietary intake. They concluded that it was not only price, but also familiarity that mediated the effects of socio-economic status indicators on diet. Individuals with lower levels of education and income attached greater importance to familiarity when purchasing food( Reference Konttinen, Sarlio-Lähteenkorva and Silventoinen 32 ).
This explanation may be especially relevant for Crete and Greece because increasing evidence suggests that the traditional Mediterranean diet patterns of people in this region are changing and a more Western-style and less healthy diet is progressively being adopted( Reference Angelopoulos, Kourlaba and Kondaki 33 , Reference Vardavas, Linardakis and Hatzis 34 ). Thus, the norms about dietary patterns are deteriorating and women have to make an effort to adjust to the new, in essence old, healthier recommendations. Less tolerant women may not provide the opportunity to anything that does not have specific and pre-chosen characteristics and is outside their usual everyday routine – in this case, new and different nutritional recommendations – to become part of their regular diet.
Higher participation in the community was associated with higher Mediterranean diet scores in both bivariate and multivariable analyses, although not statistically significant in the adjusted models. Participation is anticipated to secure diffusion of information and knowledge about nutritional requirements in pregnancy and healthy eating choices and access to social support through various personal and community networks and social ties. It may be the case that it is not the quantity of information that makes women adhere to the Mediterranean diet but rather women’s motivation to adopt better health practices. Moreover, increased participation may also lead to additional obligations and responsibilities for the pregnant woman. If there is no social or another kind of support available to reciprocate with responsibilities, pregnant women may face practical limitations. For example, they may not have adequate time to shop and prepare heart-healthful meals( Reference Barbiera, Attree and Todd 35 ).
Limitations
Notwithstanding the important outcomes, the present study comes with the limitations of a cross-sectional analysis in which associations are not an indication of causality. In theory, social characteristics are more likely to influence dietary patterns than vice versa. It is less plausible that women with higher Mediterranean diet scores result in being more tolerant to diversity but their temporal relationship cannot be explored in the current study. Many researchers also suggest that the ability to adopt a healthier diet may have less to do ‘with motivation than with economic means’ (p. 1112)( Reference Darmon and Drewnowski 28 ). In the Rhea cohort we did not record the income of the participants and thus omitted variable bias cannot be excluded. However, to limit this possibility we did adjust for a number of probable indicators of socio-economic status and the results remained largely unchanged. As in most studies on diet and health, we used self-reported diet during pregnancy and therefore information bias could have occurred. However, studies of nutrition in pregnancy suggest that food frequency methods present valid and reproducible estimates of the dietary intakes in pregnant women( Reference Meltzer, Brantsaeter and Ydersbond 36 ). The most deprived section of our study population (the uneducated immigrant and Greek women) has not completed the questionnaire, but this probably underestimates the associations noted in the study. Social capital indicators were not recorded at the community level. Thus, there is the possibility that omitted community-level variables account for the noticed associations.
Conclusion
Food choice and adherence to a healthy dietary pattern is a multifaceted process. The present study suggests that social capital and tolerance of diversity are associated with a dose–response effect on adherence to the Mediterranean diet in pregnant women. Higher social capital may result in an increased concern about diet and health outcomes that may, in turn, result in engagement in proactive health- and nutrition-related activities. Furthermore, less tolerant women may not provide the opportunity to new healthier nutritional recommendations to become part of their regular diet. This is particularly relevant in contexts where the norms about dietary patterns are deteriorating. Nevertheless, future research should apply a longitudinal design to investigate whether social capital is a mediator of positive changes in nutritional behaviour during pregnancy, to test these assumptions.
Acknowledgements
Financial support: This work was partly supported by the European Union Integrated Project NewGeneris, 6th Framework Program (contract FOOD-CT-2005-016320), and by the European Union-funded project HiWATE, 6th Framework Program (contract FOOD-CT-2006-036224). The funders had no role in the conduct of the research or in the design, analysis or writing of this article. Conflict of interest: None. Authorship: G.K. conceived the study design for this article, participated in the statistical analysis and wrote the paper; L.C. participated in the study conception and design, the statistical analysis and in the critical revision of the paper; V.G. and M.V. participated in the analysis and interpretation of the results and in drafting of the manuscript; A.E.P. participated in the study design for this article and critically revised the manuscript; A.K. and M.K. conceived the study, participated in its design and helped to draft the manuscript and to revise it critically. All authors contributed substantially to the study and have personally reviewed and approved the submitted manuscript. Ethics of human subject participation: The study was approved by the ethical committee of the University Hospital in Heraklion, Crete, Greece and all participants provided written informed consent after a complete description of the study.





