


Anaemia, defined as reduced blood Hb concentration, is one of the most important diseases in the world due to its high prevalence and the harm that it causes to the health of individuals( 1 – Reference Olivares and Walter 3 ). Although there are various forms of anaemia, according to the different aetiologies, the one caused by Fe deficiency (Fe-deficiency anaemia) is the most prevalent. The WHO estimates that 42 % of anaemia cases in children would likely be corrected with Fe supplementation( 1 ).
Anaemia is one of the most prevalent nutritional deficiencies in Brazil. Since 2005, under the National Policy on Food and Nutrition, a prevention and control programme called the National Program for Iron Supplementation (NPIS) has been implemented. It consists of prophylactic supplementation with ferrous sulfate, nutritional education, food fortification with Fe and folic acid, and providing guidance manuals for health professionals in primary health care( 4 ).
In Alagoas, one of the Brazilian states with the worst social indicators in the country, it was found that anaemia affected 45·1 % of pre-school children( Reference Vieira, Ferreira and Costa 5 ). That survey was conducted in the same year (2005) in which the Ministry of Health established the NPIS. A similar survey was conducted again in 2015, thus enabling analysis of the temporal evolution in anaemia prevalence and possibly contributing to evaluation of the effectiveness of the actions undertaken.
The present work aimed to identify the prevalence and temporal trend (2005–2015) of anaemia in children from Alagoas State, Northeast Brazil.
Materials and methods
Survey overview
The present study was based on two household surveys that were integrated into a larger project called the ‘Diagnosis of Maternal and Child Health of the Population of Alagoas State’ that was carried out in 2005 and 2015 (Survey I and Survey II, respectively). In both cases, the purpose of the sampling was to obtain a representative sample of children aged 6–60 months from Alagoas State. The following parameters were adopted to calculate the sample size in Survey I: a 40·6 % prevalence( Reference Oliveira, Osorio and Raposo 6 ), 3·5 % error margin and 95 % CI would require 756 children. In Survey II, the sample size was calculated taking as reference the 45·1 % prevalence observed in Survey I( Reference Vieira, Ferreira and Costa 5 ). Admitting a margin of error of 3·5 % and a 95 % CI, 774 children were required.
In the two surveys, the sampling procedure included multiple stages with three steps. In the first survey, twenty of the 102 municipalities in Alagoas State were drawn randomly by systematic sampling with a probability proportional to the size of the population. For this, they were organized in alphabetical order, containing their respective populations (Maceió, the capital of Alagoas, was drawn six times because it has approximately one-third of the state’s population). In the second step, four census tracts by municipality were chosen by a simple drawing (considering the proportion of their respective urban and rural population), and in the third step, a starting point within each sector was randomly designated from which twenty-eight consecutive households were visited. A similar sampling procedure was performed in the second survey.
Ethical aspects
All children aged 6–60 months whose mothers or guardians signed the informed consent form, as provided in the terms of the two projects approved by the Ethics Committee in Research of Alagoas Federal University (process number 010102/03-55 and 09093012.0.0000.5013 for Survey I and II, respectively), participated in the study.
Data collection
Properly trained and supervised interviewers, using forms previously tested in a pilot study, collected demographic, socio-economic, environmental, anthropometric and health data.
Dependent variable
The dependent variable was anaemia, diagnosed as Hb <11 g/dl, and classified as mild (9·0 g/dl<Hb<11·0 g/dl), moderate (7·0 g/dl≤Hb≤9·0 g/dl) or severe (Hb<7·0 g/dl)( 1 ). Hb assays were performed using a HemoCue® Hb 301 (HemoCue Ltd, Sheffield, UK) with a drop of blood obtained by finger prick. After the examination, the mother or guardian for the child received a form with the result and, when anaemia was present, was encouraged to seek the nearest health-care service to get the proper treatment. Health officials in the area were contacted to take notes and support the work and to recognize the form used by the team for specifying the examination results.
Independent variables
To identify the possible factors associated with anaemia, the following conditions were investigated: age (6–12, 13–24, 25–36, 37–48 and 49–60 months; and in dichotomous form, ≤24 months and >24 months), gender, number of family members (≤4; >4), maternal age (≤20 years; >20 years), age at first pregnancy (≤20 years; >20 years), origin of water used for drinking (inadequate (i.e. river, well, spring, rain, etc.); adequate (i.e. public supply or bottled water)), total number of rooms in the house (≤4; >4), number of rooms in the house used for sleeping (≤2; >2), possession of consumer goods (such as television, car, washing machine and refrigerator: ≤2; >2), per capita income (≤$US 57/month; >$US 57/month), area of residence location (rural; urban), maternal schooling (≤8 years of study; >8 years of study), government assistance programmes (e.g. family welfare programme user: yes; no) and the occurrence of diarrhoea in children in the last 15 d (yes; no).
For the cut-off point used to establish the categories of per capita income (≤$US 57/month; >$US 57/month), the new established poverty line of $US 1·90 daily was used and was based on the purchasing power parity in the poorest countries of the world while preserving the real purchasing power of the previous line, $US 1·25 daily( 7 ). The exchange rate used to convert the reported amounts from Brazilian Reals (R$) into US dollars was $US 1·00=R$2·25 in January 2006 (for Survey I) and $US 1·00=R$2·63 in January 2015 (for Survey II).
Statistical analysis
The data were entered independently into a double-entry form created in Epi Info version 3.5.4. After comparing the files and correcting the discrepancies, we conducted the statistical analyses in the statistical software package Stata/SE 12.1 for Windows.
After confirming compliance with the parametric assumptions (using the Kolmogorov–Smirnov test and Bartlett’s test), Student’s t test was used to compare mean Hb values. Pearson’s χ 2 test was used to compare anaemia prevalence.
Evolution of anaemia prevalence observed between the surveys was described as a percentage, [(current prevalence – previous prevalence)/previous prevalence]×100, and by the prevalence ratio (PR) in both crude and adjusted analyses.
To check the factors associated with anaemia at the time of the second survey, the PR and its 95 % CI were used. The associations that obtained a significance of P<0·2 in the crude analysis were subjected to multivariable analysis. This criterion for including covariates in the multivariate analysis has been used by other authors( Reference Leal, Batista Filho and de Lira 8 – Reference Lisbôa, Oliveira and Lamounier 12 ). In the final model, the only remaining variables were those significantly associated with anaemia (P<0·05). The exclusion of non-significant variables occurred through backward processing. The respective PR and 95 % CI were calculated by Poisson regression with robust variance adjustment.
Results
The final sample of Survey I had 666 children with ages ranging from 6 to 60 months (88·1 % of the planned sample size), while 782 individuals composed the sample analysed in Survey II (101·0 % of the planned sample size).
The characteristics and the evolution of the independent variables in the two analysed periods are displayed in Table 1. In 2015, there was a significant increase (P<0·05) in the proportions of children aged >24 months and mothers aged >20 years, in the number of families that had more than two consumer goods and fewer than four co-inhabitants at home, in per capita income >$US 57/month, maternal schooling, houses with more than four rooms and, finally, in the number of families using government assistance programmes.
Table 1 Distribution and evolution of demographic, socio-economic, environmental and health characteristics related to children aged 6–60 months from Alagoas State, Northeast Brazil, 2005–2015
† $US 1·00=R$2·25 in January 2006 (Survey I); $US 1·00=R$2·63 in January 2015 (Survey II).
‡ Diarrhoea on the same day or up to 15 d before the interview.
Table 2 shows data on the prevalence and evolution of anaemia from 2005 to 2015, among the different age groups of children. The prevalence of anaemia was 45·1 % in 2005 and 27·4 % in 2015, representing a decline of 39·1 % (PR=0·61; 95 % CI 0·52, 0·70). There was a reduction in anaemia prevalence in all age groups except 37–48 months; however, statistically significant differences were observed only for the three younger age groups (P<0·001). Compared with the highest age range (49–60 months), the prevalence among the younger age groups (6–12 and 12–24 months) was 3·38 and 2·62 times higher, respectively. In both 2005 and 2015, children aged ≤24 months were more affected than were those aged >24 months: 67·2 v. 27·0 % (P<0·001; PR=2·49; 95 % CI 2·07, 3·00), respectively, in 2005 and 40·7 v. 19·3 % (P<0·001; PR=2·10; 95 % CI 1·68, 2·65), respectively, in 2015.
Table 2 Prevalence and temporal trend (2005–2015) of anaemia in children aged 6–60 months from Alagoas State, Northeast Brazil
PR, prevalence ratio; Ref. reference category.
* Prevalence of anaemia was significantly different from that in 2005 (P<0·001; χ 2).
† Comparison of the prevalence in 2015 v. 2005, considering the respective age group.
‡ Comparison of the prevalence in 2015 in the respective age group v. the prevalence in 2015 in the highest age group (49–60 months), as reference.
Consistent with these findings, there was an increase in mean Hb level, rising from 11·0 (sd 1·5) g/dl in 2005 to 11·6 (sd 1·3) g/dl in 2015 (P<0·01).
There was a significant decline in all anaemia categories, as illustrated in Fig. 1. The near disappearance of the severe form in 2015 is noteworthy, as it was confirmed in only four cases (0·5 %).
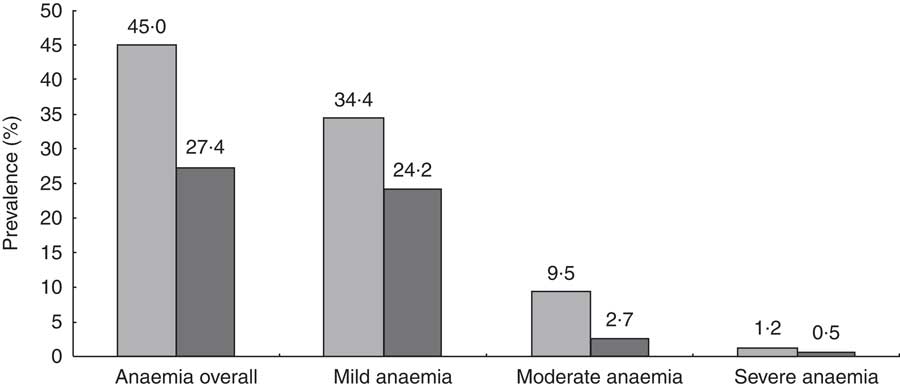
Fig. 1 Prevalence and temporal trend (2005–2015) of anaemia in children aged 0–60 months from Alagoas State, Northeast Brazil. All prevalences observed in 2015 (![]() ) were significantly lower (P<0·01) than the respective values observed in 2005 (
) were significantly lower (P<0·01) than the respective values observed in 2005 (![]() )
)
Data on the prevalence and evolution of anaemia, according to the independent variable categories analysed during the two surveys, are found in Table 3. In 2015, the variables that were associated with anaemia were: age of the child, origin of the water used to drink, consumer goods’ ownership, place of residence, maternal education (number of years of study) and child with diarrhoea. These variables were considered covariates and used in the multivariate analysis. In addition, the following conditions that reached P<0·2 in the crude analysis were considered: age at the first maternal pregnancy, number of rooms in the house and number of rooms used to sleep.
Table 3 Prevalence and temporal trend (2005–2015) of anaemia in children aged 6–60 months, according to demographic, socio-economic, environmental and health characteristics, Alagoas State, Northeast Brazil
PR, prevalence ratio; Ref. reference category.
* Prevalence of anaemia between the two categories in 2015 was significantly different (P<0·05; χ 2 test).
** Prevalence of anaemia between the two categories in 2015 showed a significance level greater than 5·0 % but less than 20·0 % (0·05<P<0·2).
† Comparison of the prevalence in 2015 v. 2005, in the respective category of the independent variable.
‡ Comparison of the prevalence in 2015 in the respective category of the independent variable v. the prevalence in 2015 in the other category of the independent variable, as reference. All variables that presented *P<0·05 or **P ≥0·05 to <0·2 were included in the multivariate Poisson regression model. However, the variables with a lower level of significance were successively excluded (backward stepwise elimination), so that, in the final model, only those with P<0·05 remained (adjusted PR).
§ $US 1·00=R$2·25 in January 2006 (survey in 2005); $US 1·00=R$2·63 in January 2015 (survey in 2015).
║ Diarrhoea on the same day or up to 15 d before the interview.
The variables that remained significantly associated with anaemia after adjusted analysis in 2015 were the age of the child, maternal education and the origin of the water used to drink. More specifically, the categories that were identified as independent risk factors for anaemia were: being ≤24 months old, being the child of a mother with ≤8 years of study and not having access to good-quality water to drink.
It is important to note that, even after adjusting for all these factors, the reduction in anaemia prevalence between 2005 and 2015 remained statistically significant (PR=0·64; 95 % CI 0·55, 0·74; P<0·001).
Discussion
The WHO classifies anaemia in children as a severe public health problem when its prevalence is over 40 %, with values between 20 and 40 % characterizing a situation of moderate importance( 13 ). Given this, the decline from 45·1 to 27·4 % found in Alagoas in the year 2015 shows that despite the change in baseline (severe to moderate), the disease is still a legitimate health problem in this population.
The noted decline placed the prevalence of anaemia in Alagoas at a lower level than both the overall estimate (42·6 %) published by the WHO for pre-school children( 1 ) and the values recorded in surveys conducted in other states in Northeast Brazil (36·5 % in the state of Paraiba( Reference Gondim, Diniz and Souto 10 ) and 33·0 % in the state of Pernambuco( Reference Leal, Batista Filho and de Lira 8 )).
The prevalence did not differ significantly from those reported in recent studies (the last 10 years) conducted among children from the South/Southeast of the country, where the states are distinguished from those of the Northeast because they are economically more developed and have better social and health indicators. In these studies, the prevalence ranged from 30·2 to 45·4 %( Reference Assuncao, Santos Ida and Barros 14 – Reference Silla, Zelmanowicz and Mito 19 ).
Internationally, the prevalence now found is higher than that estimated for developed countries, such as the USA, Canada and Europe (7·0–19·3 %), but lower than the verified prevalence (42·0–60·2 %) in poor countries or in developments located in Asia or Africa( 1 ).
When analysing the temporal trend for the prevalence of anaemia, there are other studies conducted among populations in the Northeast region of Brazil( Reference Leal, Batista Filho and de Lira 8 , Reference Gondim, Diniz and Souto 10 , Reference Vasconcelos, Cavalcanti and Leal 11 ); however, the data in these surveys were collected eight or more years ago, making it difficult to compare them with our results. In the state of Paraiba, one study reported a marked increase in cases in the period between 1982 and 1992 (from 19·3 to 36·4 %) and a stabilization in the period from 1992 to 2007 (36·4 v. 36·5 %), but at a high level( Reference Gondim, Diniz and Souto 10 ). In the state of Pernambuco, there was a reduction of approximately 19·3 % in anaemia prevalence, from 40·9 % in 1997 to 33·0 % in 2006( Reference Leal, Batista Filho and de Lira 8 ).
Compared with 2005, significant changes were observed in 2015 in several variables that could be associated with the prevalence of anaemia in Alagoas (i.e. the proportions of children aged >24 months and mothers aged >20 years, the number of families that had more than two consumer goods and with less than four co-inhabitants at home, per capita income >$US 57/month, maternal schooling, houses with more than four rooms and, finally, the number of families using government assistance programmes). Therefore, for better comparability, it was necessary that the prevalence observed in 2015 be adjusted for all those variables that had an association with a significance level of at least 20 % (P<0·2). According to the multivariate analysis, the risk factors independently associated with anaemia in 2015 in the current study were child age ≤24 months, mother with low education and inadequate source of drinking-water.
Several studies conducted in Northeast Brazil have revealed that children are more susceptible to anaemia in the first 2 years of life( Reference Vieira, Ferreira and Costa 5 , Reference Vasconcelos, Cavalcanti and Leal 11 , Reference Oliveira, Augusto and Muniz 20 ), which is why that age group, as well as pregnant and postpartum women, are the target population for actions of the Brazilian NPIS( 4 ). National and international studies have also shown this association( Reference Leal, Batista Filho and de Lira 8 , Reference Gondim, Diniz and Souto 10 , Reference Lisbôa, Oliveira and Lamounier 12 , Reference Alaofe, Burney and Naylor 21 – Reference Goswmai and Das 23 ).
Several reasons have been presented to explain this increased susceptibility in this age group. Biological demands related to growth and development that generate higher physiological demands for Fe and other nutrients( Reference Konstantyner, Taddei and Palma 24 ) and food-related issues, such as an increased consumption of cow’s milk, feeding complementary to breast-feeding up to 2 years and inadequate and/or early abandonment of exclusive breast-feeding( Reference Oliveira, Osorio and Raposo 6 , Reference Hipgrave, Fu and Zhou 25 , Reference Chandyo, Henjum and Ulak 26 ), cause anaemia to be more prevalent in children under 24 months of age compared with older children( Reference Lisbôa, Oliveira and Lamounier 12 , Reference Velásquez-Hurtado, Rodríguez and Gonzáles 27 ). Moreover, feeding for children older than 24 months tends to be similar to that of their family members, involving greater consumption of foods with high Fe density( Reference Oliveira, Osorio and Raposo 6 ), unlike at younger ages, when milks and farinaceous foods are more commonly given( Reference Vasconcelos, Cavalcanti and Leal 11 ).
Like in our study, low maternal education has been identified in several works performed in Brazil( Reference Oliveira, Osorio and Raposo 6 , Reference Leal, Batista Filho and Lira 9 , Reference Leite, Cardoso and Coimbra 28 – Reference Monteiro, Szarfarc and Mondini 30 ) and other countries( Reference Alaofe, Burney and Naylor 21 , Reference Goswmai and Das 23 , Reference Velásquez-Hurtado, Rodríguez and Gonzáles 27 , Reference Ewusie, Ahiadeke and Beyene 31 – Reference Agho, Dibley and D’Este 35 ) as an important risk factor for anaemia in children. Better maternal education is a variable that is associated with a higher socio-economic status and higher income, which enables access to adequate nourishment and other items related to health and quality of life( Reference Oliveira, Osorio and Raposo 6 , Reference Monteiro, Szarfarc and Mondini 30 ).
As already mentioned, in the present study, an improvement in maternal schooling was observed between 2005 and 2015. Consistent with our findings, research conducted by the Brazilian Institute of Geography and Statistics (National Survey by Household Sample) revealed an important decline in the rate of illiteracy in the country, with a more intense decline in the North and Northeast of the country( 36 ), where the worst social indices were observed.
Beyond the perspective of financial accessibility, a higher educational level can provide mothers with a better understanding of the environment, health and feeding of the child( Reference Pasricha, Drakesmith and Black 37 ). Exploring data from 10 137 children aged 0–6 years from north-eastern India, it was found that children of literate mothers had a lower risk of developing severe anaemia( Reference Dey, Goswami and Dey 33 ).
When considering an inadequate source of drinking-water as a risk factor for anaemia, there are many divergences in the literature, possibly because of the several ways in which this variable is obtained in different studies and the huge network of interactions it has with socio-economic and environmental factors.
In a study conducted with secondary data from Encuesta Demográfica y de Salud Familiar (ENDES), which occurred in Peru between 2007 and 2013, it was found that not previously boiling water used for drinking was a factor associated with anaemia( Reference Velásquez-Hurtado, Rodríguez and Gonzáles 27 ). In Pernambuco (Brazil), an association was established between anaemia and drinking-water that has not been submitted to any treatment process( Reference Leal, Batista Filho and Lira 9 ).
A study performed by Calegar et al.( Reference Calegar, Nunes and Monteiro 38 ) in a municipality in the semi-arid region of Northeast Brazil showed a higher infection rate by entamoeba (an intestinal parasite that affects intestinal nutrient absorption) among individuals who drank rainwater collected from roofs.
The quality of drinking-water as a risk factor for anaemia is not an exclusively Brazilian problem and has been identified in studies conducted in several countries( Reference Khan, Awan and Misu 22 , Reference Zhao, Gao and Li 39 , Reference Surdu, Bloom and Neamtiu 40 ).
Water has become a scarce resource and its quality has been compromised in some areas by the contribution of deforestation, erosion/sedimentation of surface waters, and discharges of effluent, industrial and domestic waste. In developing countries, this problem is aggravated due to the low coverage of the population with quality water supply services( 41 , 42 ), a key condition for family health and the expansion of local economies( 43 ). Access to safe water is a human right, but its limited realization around the world often has disproportionate impacts on the poor and on women and children in particular( 42 ).
Even after adjusting for the associated factors, the reduced anaemia prevalence in 2015 remained statistically significant, suggesting that other factors are related to the downward trend. Some of these factors may be related to the actions undertaken in the NPIS. Through this programme, the Brazilian Ministry of Health has introduced a number of measures, such as fortification of wheat and corn flour with Fe; ferrous sulfate supplementation for children aged 6–18 months, pregnant women from the 20th week of gestation and mothers until the third month postpartum; the promotion of breast-feeding; nutritional education; and school feeding programmes( 4 , Reference Ferreira, Bezerra and Assuncao 44 ).
As shown in Table 1, the number of families using government assistance programmes increased from 28·7 % in 2005 to 65·5 % in 2015.Footnote * More than 90 % of these were users of the ‘Bolsa Família’ Program, one of the strategies developed to try to eliminate famine and poverty of families in Brazil through the direct transfer of cash. The expectation is that this financial increase will also result in an improvement in the nutritional status of the children. Analysing the evolution of nutritional status of Brazilian pre-schoolers from 1996 to 2007, Monteiro et al.( Reference Monteiro, Benicio and Konno 46 ) verified that the prevalence of undernutrition fell by approximately 50 % (from 13·5 % in 1996 to 6·8 % in 2007). According to these authors, 21·7 % of this reduction was attributable to increased purchasing power of families. Although started in 2003, it is considered that the Bolsa Família programme was the main factor responsible for improving the purchasing power of families. A more recent study carried out in Brazil concluded that the Bolsa Família programme’s impact on food availability among low-income families was higher food expenditure and higher availability of fresh foods and culinary ingredients, including those foods that increase dietary quality and diversity( Reference Martins and Monteiro 47 ).
Thus, although the association between anaemia and the use of government assistance programmes lost statistical significance in the adjusted analysis, there is evidence suggesting that part of the reduction now observed in anaemia prevalence is explained by the increase in household purchasing power via the ‘Bolsa Família’ Program.
It is important to highlight that, in addition to the direct transfer of cash, the Bolsa Família programme presents some conditionalities that must be fulfilled by the beneficiary families and by the municipal government and that, in the set of actions, could be responsible for the possible impact of the federal programme. These conditionalities include actions such as children’s school attendance, compliance with the immunization schedule, monitoring of growth and development, and the participation of pregnant women in prenatal care( 48 ).
According to Oliveira et al.( Reference Oliveira, Augusto and Muniz 20 ), this Brazilian programme, together with other strategies to combat anaemia, has contributed significantly in reducing the prevalence of this disease. In evaluating the programme, however, it is argued that such a contribution could be higher in all Brazilian municipalities if the supplement distribution system was fully accessible to the target group( Reference Azeredo, Cotta and Silva 49 ) and if there were more training and motivation activities for the professionals involved in their execution( Reference Azeredo, Cotta and Silva 49 , Reference Oliveira, Nascimento and Moreira 50 ).
A reduction in anaemia prevalence may be a new epidemiological trend( Reference Vasconcelos, Cavalcanti and Leal 11 ), and the progress in socio-economic and educational conditions between 2005 and 2015 observed in the present study may have contributed to this reduction. The lack of recent population-based surveys conducted in Brazilian states affected the comparability of our results and the confirmation of such an ‘epidemiological trend’. Given the socio-economic, cultural and environmental similarities between the states in the Brazilian north-east, however, it is possible that the anaemia prevalence may also be decreasing in the respective populations in such states.
A process of nutritional, epidemiological and demographic transition has been observed throughout the national territory( Reference Belik 51 ). Big changes in Brazil started just before the 2005 survey. The fertility rate fell from 2·09 in 2005 to 1·72 in 2015( 52 ). If children younger than 24 months is a risk factor for anaemia, then the decline in fertility that occurred would mean a smaller proportion of the overall population was at risk of anaemia. Such alteration could indirectly lead to a decline in the proportion of individuals with anaemia. The same would be true for the reduction in the number of teenage mothers, mothers with low education and extremely poor families, among other favourable changes occurring in the period.
A limitation of the present study was not investigating differences in the pattern of food consumption in both analysed periods, particularly in relation to Fe intake adequacy, which hinders the understanding of the factors involved in the analysed outcomes. However, the study presents updated data on anaemia prevalence and its temporal trend, which were obtained in a well-planned and representative sample of children in a Brazilian state.
The prevalence of anaemia in children from Alagoas State has been declining at a significant rate and is no longer considered a severe public health problem but one of moderate magnitude; however, it remains above the acceptable level (5 %) according to WHO criteria. The risk factors independently associated with anaemia were being less than 24 months old, being the child of a mother with a low educational level and not having access to good-quality drinking-water. These characteristics should be considered by professionals and managers of public health policies. Between 2005 and 2015, there were significant improvements in the socio-economic and public education conditions, characteristics that, combined with the actions of the NPIS, possibly contributed to the decline in the prevalence of anaemia. These results justify the maintenance and implementation of prevention and control actions.
Acknowledgements
Financial support: H.S.F is a research fellow of the National Research Council (CNPq; grant number 302732/2015-2) and R.C.S.V. is a PhD scholarship fellow at the Foundation for Suppport to Research of the Amazonas State (process number 252/2014). This work is part of the II Health Diagnosis of Maternal Population of Alagoas State, carried out with funds from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (process number 474381/2011-0), Fundação de Amparo à Pesquisa do Estado de Alagoas (FAPEAL)/CNPq (process number 20110818-006-0018-0017) and FAPEAL/CNPq/Secretaria de Estado da Saúde (SESAU)–Programa de Pesquisa para o Sistema Único de Saúde (PPSUS) (process number 60030.000716/2013). The funders had no role in the design, analysis or writing of this article. Conflict of interest: The authors declare that they have no conflict of interest. Authorship: R.C.S.V. participated in designing the study, in analysis and interpretation of the data, and drafting the article. A.R.S.L., M.S.C.C., C.M.X.F., T.R.S. and M.L.A. took part in the acquisition of data, data entry, analysis and interpretation, and writing. H.S.F. took part in the project’s conception, obtained the respective financial support, coordinated all implementation steps and realized the final review of the article. All authors approved the final version to be submitted. Ethics of human subject participation: The surveys were approved by the Ethics Committee in Research of Alagoas Federal University (process numbers 010102/03-55 (Survey I) and 09093012.0.0000.5013 (Survey II)). The mothers or guardians of all participating children aged 6–60 months signed an informed consent form.




