



Introduction
Performing artist refers to an artist who is involved in a theatrical presentation that incorporates various art forms, such as dance, sculpture, and music. The subtlety of performances by artists speaks of the time dedicated to learning and perfecting the intricate movements in the performance. However, their performances may be debilitated by many medical conditions such as neuromuscular injury, tendinitis, and focal dystonia. Reference Lederman1
Dystonia is the commonest movement disorder encountered in performers. It is characterized by sustained, involuntary, and repetitive contractions of muscles causing abnormal posturing or twisting of a body part. Reference Albanese, Bhatia and Bressman2–Reference Tarsy and Simon5 Focal task-specific dystonia (FTSD) refers to continuous, involuntary muscle contractions of a single body part that manifests during a particular activity and results in abnormal posturing of the body part. Reference Lo and Frucht6
Task-specific dystonias have been described among performing artists. The term “musicians’ dystonia” refers to task-specific dystonia among musicians while playing musical instruments. Among performing artists, focal dystonia of hand has most commonly been described among the musicians. However, task-specific dystonia among musicians is not limited to hands alone. Musicians playing embouchure instruments and those playing lower limb percussion instruments and singers who extensively use their vocal cords are also at risk of developing FTSD of the overused muscles. These dystonias include embouchure dystonia (ED), lower limb drummers’ dystonia, and singer’s dystonia (SD). The literature is replete with the vast repertoire of knowledge of phenomenology, pathogenesis, and therapies in the field of musicians’ hand dystonia, while knowledge in the rarer forms of dystonia in performing artists has been relatively limited. This review aims to highlight the lesser known FTSDs among performing artists –ED, lower limb drummers’ dystonia, and SD. Although task-specific dystonia of lower limb has also been seen among dancers, this dystonia has not been discussed in view of paucity of literature. The first part of the review delineates the phenomenology and diagnosis of these dystonias, and the second part discusses the pathogenesis of ED and FTSD of lower limb. The possible pathogenetic mechanisms behind the decreased propensity of lower limbs to develop task-specific dystonia in musicians are also discussed.
Search Strategy
Search for relevant articles was carried out using PUBMED database on 18 July 2020, and the references were selected based on relevance to this topic. Using the terms “embouchure” and “dystonia,” the search results showed 34 articles, of which 25 articles were selected.
Using the terms such as “percussionist,” “drummer,” and “dystonia,” 21 articles were found out of which 5 articles were selected. Certain case series on FTSD of lower limb have included percussionist dystonia. To identify these articles, search terms such as “lower limb” and “dystonia” were used, showing 393 results out of which 3 articles were selected.
Search using the terms such as “singer” and “dystonia” yielded 78 results. Six articles were relevant to this review and were selected.
Clinical Features
Embouchure Dystonia (ED)
Embouchure refers to muscles of lips, tongue, jaw, and face that function harmoniously to modulate airflow into mouthpiece of an instrument. Reference Termsarasab and Frucht7 ED refers to dystonia of the perioral and facial muscles that occurs in musicians while playing embouchure instruments. Reference Frucht, Fahn and Greene8 Task-specific dystonia involving the oral muscles has been reported in prayer-induced lingual dystonia Reference Ilic, Pötter, Holler, Deuschl and Volkmann9 and auctioneer’s jaw. Reference Scolding, Smith, Sturman, Brookes and Lees10
Epidemiology
The exact incidence of ED is not known. In a study conducted by Moura et al., of the 2233 musicians studied, 318 musicians were identified to have motor control disorders. Among them, 49 musicians (2.2%) were classified as having musicians’ dystonia. Among 22 wind players, 16 reported ED (70%). Reference Moura, de Carvalho Aguiar, Bortz and Ferraz11 In another study of 119 musicians with musician dystonia (MD), ED was observed in 19% of the patients. Reference Schmidt, Jabusch and Altenmüller12 In a study of 585 brass musicians, 68% of musicians reported embouchure problems. Reference Steinmetz, Stang, Kornhuber, Röllinghoff, Delank and Altenmüller13 The age of onset of ED ranged from 16 to 66 years. Reference Termsarasab and Frucht7,Reference Frucht, Fahn and Greene8,Reference Frucht14–Reference Brandfonbrener16 Among these individuals with ED, the age of starting the training ranged from 8 to 22 years. Reference Frucht, Fahn and Greene8,Reference Frucht14 Individuals with ED reported performance impairment 1 month to 27 years after the onset of symptoms. Reference Termsarasab and Frucht7,Reference Frucht14 Among musicians with ED, 70%–78% of the patients were males. Reference Termsarasab and Frucht7,Reference Frucht14
Precipitating Factors
Unlike musicians’ hand dystonia where a triggering factor such as ulnar, median, or posterior interossei neuropathy, Reference Schuele and Lederman17,Reference Charness, Ross and Shefner18 or recent change in the intensity or pattern of practice Reference Brandfonbrener16,Reference Schuele and Lederman17 has been documented, the association between the similar trigger factors and ED is weak. Patients have reported an increase in practice time or precision in practice prior to the onset of ED, Reference Frucht, Fahn and Greene8 but the number of patients reporting this change is negligible. Reference Frucht14 In a study by Frucht, history of trauma to the oral cavity was reported by 2% of the patients. Reference Frucht14
Phenomenology
Embouchure instruments have been classified into brass (French horn, trumpet, trombone, and tuba), single reed (clarinet and saxophone), double reed (oboe and bassoon), and flute. Reference Termsarasab and Frucht7,Reference Frucht, Fahn and Greene8,Reference Frucht14 Extremely high force of 50–100 pounds per square inch is used while playing high-register brass instruments that could be a cause for the abnormal distortions. Reference Conti, Pullman and Frucht19
Classification of Phenomenology
The phenomenology of ED has been classified into six phenotypes – embouchure tremor (ET), lip-pulling phenotype, lip-locking, Meige’s syndrome, jaw dystonia, and tongue dystonia. Reference Termsarasab and Frucht7,Reference Frucht14 The lip tremor appears while performing the task, rather than assuming the position of playing the instrument. Reference Frucht, Fahn and Greene8 Both upper and lower lips are involved, and the frequency of oscillation is very high. In the lip-pulling phenotype, lateral deviation of the lip or angle of mouth, and outward protrusion of one or both lips are seen. In the lip-locking phenomenology, lips involuntarily seal around the mouthpiece of the instrument resulting in airflow impairment. Reference Frucht, Fahn and Greene8
Jaw dystonia phenotype includes jaw tremor, jaw closure, and anterior or lateral movement of jaw. Reference Frucht, Fahn and Greene8,Reference Frucht14 The dystonia phenotype is dictated by the instrument that is played (Table 1). Register of an instrument refers to the pitch of the sound produced by the instrument. The pitch of the sound emanating from a low-register instrument is lower than that produced by a high-register instrument. Embouchure instruments are classified into low-register and high-register instruments. Low-register brass instruments’ players such as trombone and tuba report lip-locking movements, whereas high-register brass instruments such as trumpet and brass horn show lip-pulling movements and ET. Tongue dystonia and jaw dystonia are most commonly seen in woodwind instrument players. The jaw plays an important role in playing reed instruments and hence jaw dystonia phenotype is commonly seen in these musicians. Reference Termsarasab and Frucht7 Apart from instrument specificity, the dystonia is register-specific (i.e., dystonia develops while playing at a particular pitch), speed-specific as well as technique-specific. Reference Frucht20 Register and technique specificity were observed in 62.1%–71% and 41.3%–51% of the musicians with ED, respectively. Reference Termsarasab and Frucht7,Reference Frucht14 As the disease progresses, other registers eventually get affected. Reference Frucht14
Table 1: Phenomenology and epidemiology of ED
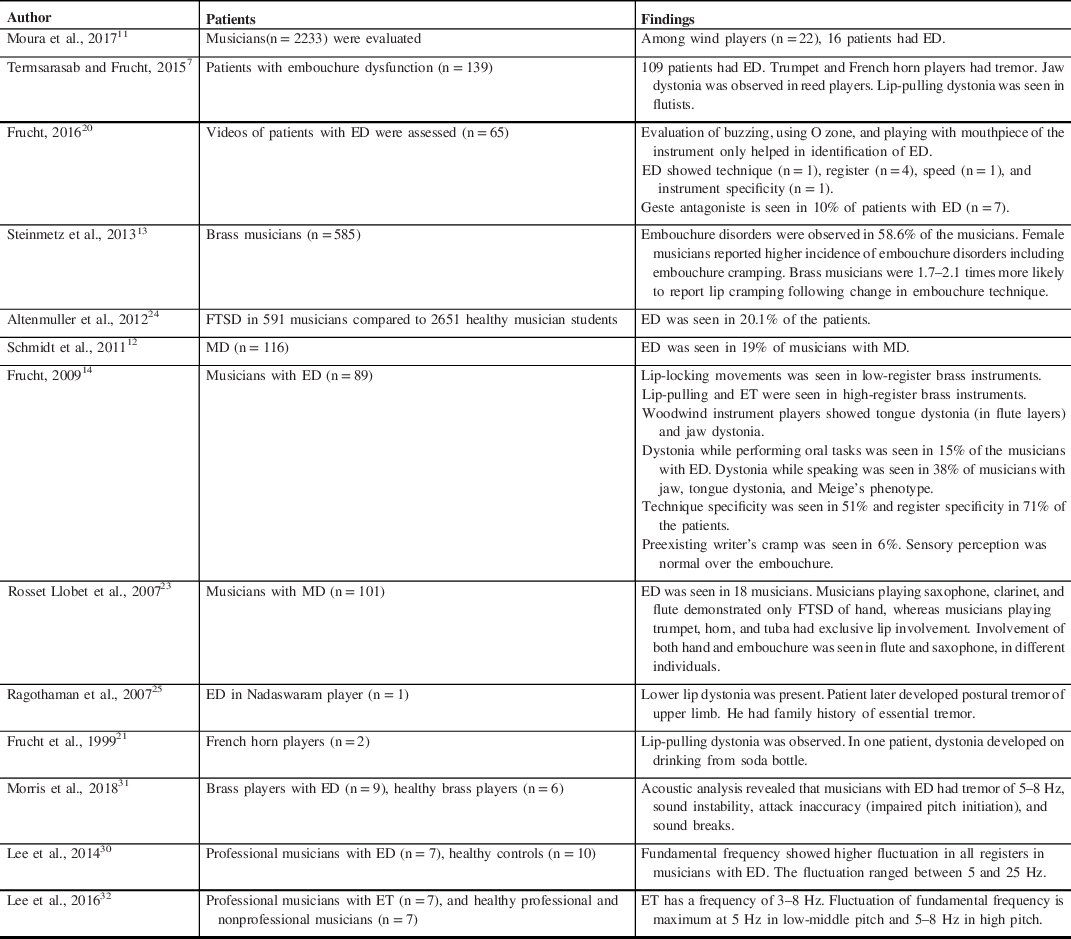
ED = embouchure dystonia; ET = embouchure tremor; MD = musician dystonia; FTSD = focal task-specific dystonia.
Spread of Dystonia in ED
ED has been reported to spread to activities such as speaking, eating, Reference Termsarasab and Frucht7 and drinking from bottle with small aperture. Reference Frucht, Fahn and Greene8,Reference Frucht14,Reference Frucht, Fahn and Ford21 It is most commonly associated with jaw dystonia phenotype. Reference Termsarasab and Frucht7,Reference Frucht, Fahn and Greene8,Reference Frucht14 Spread of dystonia has also been observed among patients with ED who have tongue dystonia and Meige phenotype. Reference Frucht14 Meige syndrome has also been reported as a consequence of spread of ED. Reference Termsarasab and Frucht7,Reference Frucht, Fahn and Greene8,Reference Frucht14 Fifteen percent of patients reported dystonia while performing other oral tasks. Thirty-eight percent of patients with jaw, tongue dystonia, and Meige phenotype reported dystonia while speaking. Reference Frucht14 However, this spread of dystonia is not observed in lip-locking and ET. Reference Termsarasab and Frucht7 Coexisting FTSD of hand has also been reported Reference Frucht20 with few musicians developing focal hand dystonia many years (up to 19 years) prior to the onset of ED, indicating the possibility of genetic predisposition. Reference Frucht, Fahn and Greene8
Geste Antagoniste and Pain in ED
Geste antagoniste, reflecting the effect of internal sensory input on the sensorimotor plasticity, is rarely observed in ED. Reference Frucht20 Geste antagoniste was seen in 10% of patients with ED in one study. Reference Frucht14 However, when it is effective, the response is almost dramatic. Reference Frucht20 Cooling of periorbital area has resulted in transient improvement in ED in a tuba player. Reference Kim, An, Lee and Kim22 Although pain is characteristic in embouchure disorders such as Satchmo syndrome, pain is observed in 12%–16% of patients and oral discomfort is observed in 35%–42% of patients with ED. Reference Frucht, Fahn and Greene8,Reference Frucht14
Hand Dystonia in ED
Wind instrument players have been reported to develop musicians’ hand dystonia. Reference Conti, Pullman and Frucht19,Reference Rosset-Llobet, Candia, Fàbregas, Ray and Pascual-Leone23 Flutists engage in more complex finger movements hence explaining higher chances of focal hand dystonia compared to the brass musicians. Reference Altenmüller, Baur, Hofmann, Lim and Jabusch24 In one case report, a Nadaswaram (an Indian double-reed instrument made of wood with metal at the end of the instrument) player with ED initially presented with ET and task-specific upper limb tremor but later developed postural tremor of upper limb. Reference Ragothaman, Swaminath, Pal and Muthane25 The laterality of involvement is dependent on burden on the fingers. Reference Altenmüller, Baur, Hofmann, Lim and Jabusch24,Reference Jabusch and Altenmuller26
Differential Diagnosis of ED
Common complaints in ED include difficulty in playing, inability to control the movement of embouchure, tremor, and fatigue of lips. Reference Frucht, Fahn and Greene8 ED needs to be differentiated from other disorders affecting the embouchure. Commonest non-dystonic affliction of embouchure includes infraorbital neuropathy, Satchmo syndrome (orbicularis oris tear), and overuse syndrome. Infraorbital neuropathy results in sharp, localized pain over cheek while playing an instrument and is occasionally associated with paraesthesia. Overuse syndrome is characterized by pain over cheek, fatigue, and numbness while playing. In Satchmo syndrome, the presentation is acute onset of pain, numbness, and difficulty in playing an instrument. Reference Termsarasab and Frucht7 Mechanical injury to the embouchure also needs to be ruled out. Reference Frucht20 Stress-induced velopharyngeal incompetence characterized by air leak through nose while playing an instrument has been described. Reference Malick, Moon and Canady27 Playing instruments requiring high intraoral pressure is associated with this disorder. Reference Gordon, Astrachan and Yanagisawa28,Reference Schwab and Schultze-Florey29 The symptoms develop 30 minutes after playing the instrument. Reference Malick, Moon and Canady27
Diagnosis
Evaluation of ED is difficult due to challenges in visual inspection, especially when tongue and larynx are involved, unlike FTSD of hand that is readily visible. Reference Lee, Furuya, Morise, Iltis and Altenmüller30 Evaluation of patients with ED is augmented when musicians are examined while buzzing (an exercise wherein musicians vibrate their lips while performing embouchure tasks), while using an O piece (a device which allows the musician to observe their own lips while practicing), and when musicians are using only the mouthpiece of the instrument. Reference Frucht20 Palpation of the embouchure is essential to look for tenderness or nodules in order to rule out other causes of embouchure discomfort. Reference Termsarasab and Frucht7 Quantification of severity of ED can also be attempted based on acoustic measures Reference Lee, Furuya, Morise, Iltis and Altenmüller30,Reference Morris, Norris, Perlmutter and Mink31 (Table 1). On studying the acoustic analysis, high registers are most severely affected. Reference Lee, Furuya, Morise, Iltis and Altenmüller30,Reference Lee, Voget, Furuya, Morise and Altenmüller32
ED carries a high risk of relentless progression and high chances of spread of dystonia to other tasks particularly in jaw phenotype. Reference Termsarasab and Frucht7,Reference Frucht, Fahn and Greene8,Reference Frucht14 Hence, musicians with ED must be strongly advised to discontinue playing the instrument. Reference Frucht14
Lower Limb Dystonia
FTSD in Drummers
Epidemiology
The exact incidence of FTSD of lower limbs among drummers is not known. In a study of 591 instrumentalists with FTSD, FTSD of lower limb was found in 4 musicians. They were more likely to be percussionists according to the study. Reference Altenmüller, Baur, Hofmann, Lim and Jabusch33 Lederman reported musicians’ hand dystonia in 6 percussionists out of 139 musicians with dystonia. Reference Lederman34 However, none of these patients had lower limb drummers’ dystonia. Four drummers with FTSD of lower limb have been described in other series. Reference Altenmüller, Baur, Hofmann, Lim and Jabusch24,Reference Katz, Byl, San Luciano and Ostrem35,Reference Rosset-Llobet, Fabregas-Molas and Pascual-Leone36
Precipitating Factors
In a case series of lower limb drummers’ dystonia, the onset of dystonia closely followed a recent modification of practice, Reference Rosset-Llobet, Fabregas-Molas and Pascual-Leone36 which is a well-known trigger factor in musicians’ hand dystonia. Reference Schuele and Lederman17,Reference Conti, Pullman and Frucht19 In another case series, the drummer developed symptoms when he began playing double bass pedal (alternate foot movements were used to push respective pedals for drum percussion). Reference Lee and Altenmuller37
Phenomenology
FTSD of lower limb among drummers has been commonly observed in distal lower limb. Reference Rosset-Llobet, Fabregas-Molas and Pascual-Leone36 However, FTSD of proximal lower limb muscles has also been reported. Reference Lee and Altenmuller37 Symptoms reported by these individuals include impaired dexterity, incoordination, and loss of rhythmicity of foot movements while playing the pedal, difficulty in performing alternate foot movements, sensation of involuntary tension over knees, legs, and ankles, and tightness of thigh muscles. Involuntary posturing of toes and feet and locking of knees were also reported. Symptoms were aggravated when the beat frequency was high and during alternate foot movements. Symptoms relieved with lowering the rapidity of limb movements and unilateral limb movements. Reference Lee and Altenmuller37 Katz et al. reported beneficial effects of geste antagoniste in alleviating FTSD in a drummer. The drummer placed the toes on a higher surface and used the heel instead, for drumming Reference Katz, Byl, San Luciano and Ostrem35 (Table 2).
Table 2: Phenomenology of focal task-specific lower limb dystonia
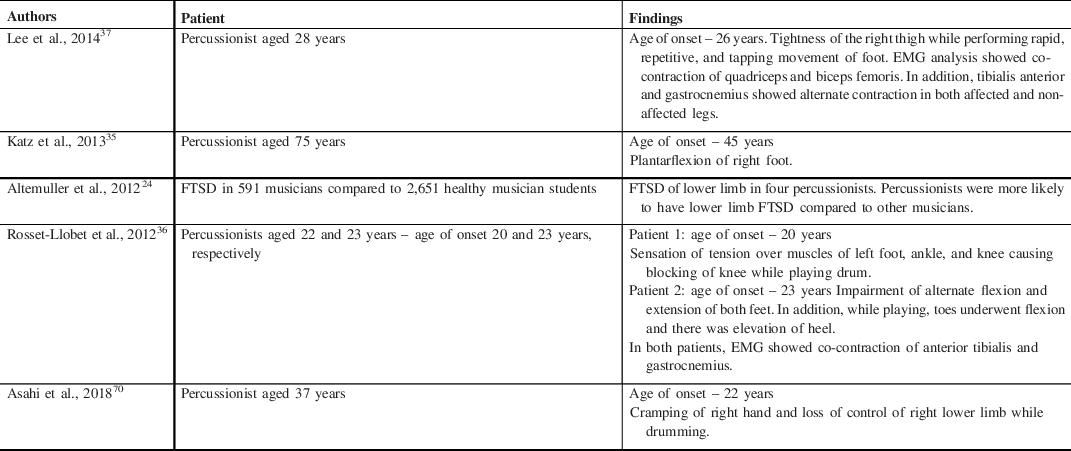
EMG = electromyogram; FTSD = focal task-specific dystonia.
Spread of dystonia to other tasks has been seldom reported in FTSD of lower limb of drummers. Only one case series narrates an account of a drummer who reported inward twisting of left toe during ambulation. Reference Katz, Byl, San Luciano and Ostrem35
Diagnosis
FTSD of lower limb needs to be differentiated from paroxysmal kinesigenic dyskinesia. Dystonia in paroxysmal exercise-related dyskinesia develops after few minutes of exertion unlike FTSD that develops immediately after initiation of task. Reference Rosset-Llobet, Fabregas-Molas and Pascual-Leone36 Routine electromyogram is normal in FTSD of lower limbs and is essential to rule out myogenic and neurogenic causes of lower limb movement impairment. However, electromyogram performed during task performance gives way to the diagnosis.
Electromyogram performed while performing the task shows contraction of agonist-antagonist (anterior tibial and gastrocnemius muscles) of lower limb Reference Rosset-Llobet, Fabregas-Molas and Pascual-Leone36,Reference Lee and Altenmuller37 (Table 2). In the patient with proximal lower limb involvement, electromyogram (EMG) revealed overflow of activity into the thigh resulting in co-activation of both quadriceps and biceps femoris muscles. Reference Lee and Altenmuller37
Singer’s Dystonia
SD finds its mention particularly in otorhinolaryngology practice. SD is a rare task-specific dystonia in singers with features of spasmodic dysphonia while singing only. While speaking, voice remains normal in these individuals Reference Aranguiz, Chana-Ceuvas, Alburquerque and Leon38,Reference Chitkara, Meyer, Keidar and Blitzer39 This is in contrast to spasmodic dysphonia, wherein the dystonic element affects the vocal cord when the patient is speaking. The voice is normal in individuals with spasmodic dysphonia when they are singing or laughing. Reference Halstead, McBroom and Bonilha40
Phenomenology
Symptoms of SD include cracking of voice at a particular pitch, instability at a particular register, difficulty in producing notes at a particular pitch with one patient reporting voice breaks, and requiring to cough and take a breath to continue. Patients also complain of breathless quality of voice when singing at a particular pitch. Voice fatigue while speaking has been reported. Reference Halstead, McBroom and Bonilha40 Other symptoms include unsteadiness, tightness of voice while singing certain ranges, loss of vibrato (slight variation of pitch while singing), and resonance. Reference Chitkara, Meyer, Keidar and Blitzer39 One of the patients suffered from vocal tremor and torticollis. Reference Halstead, McBroom and Bonilha40 Fabiani and Teive reported a 24-year-old singer who developed alteration of pitch and cervical discomfort while singing that progressed to cause left torticollis with laterocollis, implying the coexistence of SD and task-specific spasmodic torticollis. Reference Fabiani and Teive41 Spread of the dystonia to involve speech resulting in spasmodic dysphonia has also been reported. Family history of similar complaints was reported by one patient. Reference Chitkara, Meyer, Keidar and Blitzer39,Reference Halstead, McBroom and Bonilha40
Diagnosis
SD poses a diagnostic challenge. It can be mistaken for improper singing technique or technical issues such as laryngeal and tongue tension or difficulties during register shift. Reference Halstead, McBroom and Bonilha40 A vocal register indicates a specific set of tones or pitch with similar voice quality that can have varied ranges. Traditionally, three voice registers have been recognized – head voice, chest voice, and middle voice.
Laryngeal EMG in SD reveals dystonia of posterior cricoarytenoid muscles and thyroarytenoid muscles. Adductor-type task-specific dystonia is more common than abductor type of dystonia. Reference Chitkara, Meyer, Keidar and Blitzer39,Reference Halstead, McBroom and Bonilha40 The diagnosis of SD requires (a) task-specific (i.e., singing a particular note) voice instability characterized by alteration in tone and vibrato, which may or may not be associated with pitch specificity, (b) spectrographic analysis of singing samples that reveals aphonic breaks on performing abductor tasks, widely separated vertical striations on performing adductor tasks, and (c) laryngeal EMG that displays increased baseline activity and abnormal discharge of thyroarytenoid and posterior cricoarytenoid muscles at the affected pitch and at rest. Reference Halstead, McBroom and Bonilha40
SD shares similarities with musicians’ hand dystonia in terms of task specificity, affliction of small group of muscles, propensity to spread to other tasks, and its existence among musicians who have dedicated many years to vocal practice. Register specificity is similar to that seen in ED, seen in French horn players. Reference Frucht20 However, certain characteristics differentiate it from musicians’ hand dystonia. Unlike musicians’ hand dystonia or lower limb dystonia, SD does not appear to trigger with a change in singing patterns or recent increase in voice exertion. However, these individuals had spent many hours in practicing singing. This itself could be a predisposing factor for SD. Reference Halstead, McBroom and Bonilha40
Pathogenesis
In a seminal article on the pathogenesis of task-specific dystonia, Byl and co-workers reported that repetitive stereotyped movements might facilitate maladaptive reorganization in the brain that might result in dystonia instead of perfection of the movements. Reference Byl, Merzenich and Jenkins42 They substantiated this statement by performing cortical mapping of adult monkeys exposed to repetitive hand stress. They found an increased overlap in the receptive fields of the skin indicative of degradation of normal precise representations of various areas of the hand. Reference Byl, Merzenich and Jenkins42 Similar results of loss of differentiation and reorganization of somatosensory maps were replicated in a study of musicians’ hand dystonia. Reference McKenzie, Nagarajan, Roberts, Merzenich and Byl43,Reference Rosenkranz, Williamon, Butler, Cordivari, Lees and Rothwell44
Many theories have been proposed as the pathogenetic mechanisms behind musicians’ hand dystonia. These include abnormal plasticity Reference Pascual-Leone, Grafman and Hallett45 leading to enlarged cortical representation Reference Karni, Meyer, Jezzard, Adams, Turner and Ungerleider46 and enhanced undifferentiated excitability of the entire hand motor cortex. Reference Rosenkranz, Williamon and Rothwell47 The aberrant plasticity of the cortical-striato-pallido-thalamo-cortical circuit in dystonia Reference Eidelberg, Moeller and Antonini48 might lead to overactivation of the premotor cortex that is seen in musicians’ hand dystonia. Reference Lim, Bradshaw, Nicholls and Altenmüller49 Weak intracortical inhibition Reference Sohn and Hallett50,Reference Kaňovský, Bareš, Streitová, Klajblová, Daniel and Rektor51 and low gamma amino butyric amino acids levels in motor cortex Reference Levy and Hallett52 explain the mechanism of abnormal cortical excitability.
Pathophysiological Differences in Task-Specific Dystonia of Musicians and Nonmusicians
Comparative studies of FTSD among both musicians and nonmusicians emphasize the differential involvement of motor programs that results in dystonia. A study presented the concept of abnormal organization of network kernel that was representative of altered connectivity in FTSD. They studied differences between SD and spasmodic dysphonia as well as writer’s cramp and musicians’ hand dystonia. They concluded that an important fact distinguishing FTSD among musicians and nonmusicians is the recruitment of subcortical region, that is, cerebellum and thalamus in FTSD of musicians. Reference Fuertinger and Simonyan53 Bianci et al. reported that reduced functional connectivity in parietal operculum, primary somatosensory cortex, supplementary motor area, and superior and inferior parietal lobule is an underlying trait that differentiates the task-specific nature of dystonia in musicians (SD and musicians’ hand dystonia) from non-MD (spasmodic dysphonia and writer’s cramp). Reference Bianchi, Fuertinger, Huddleston, Frucht and Simonyan54
Embouchure Dystonia
The instrument-specific nature of ED indicates that maladaptive plasticity is inflicted upon a specific motor program. Reference Frucht, Fahn and Greene8 An example would be the normal motor program of lip closure that develops aberration culminating into an abnormal motor program of lip-locking dystonia. Reference Frucht, Fahn and Greene8 While playing high-register instruments, high intraoral pressure builds up. To compensate for this pressure, embouchure abnormalities may develop. Reference Frucht, Fahn and Greene8 Abnormalities in the oral cavity and tongue dynamics while playing embouchure are observed in ED Reference Hellwig, Iltis and Joseph55–Reference Iltis, Frahm, Altenmüller, Voit, Joseph and Kozakowski57 (Table 3). These faulty techniques could be related to the faulty motor programs that develop in ED. Further studies are required to decipher whether this is a consequence of ED or it is the faulty practice technique that makes a musician susceptible to aberrant motor program and subsequently to ED.
Table 3: Pathophysiological insights in ED through imaging
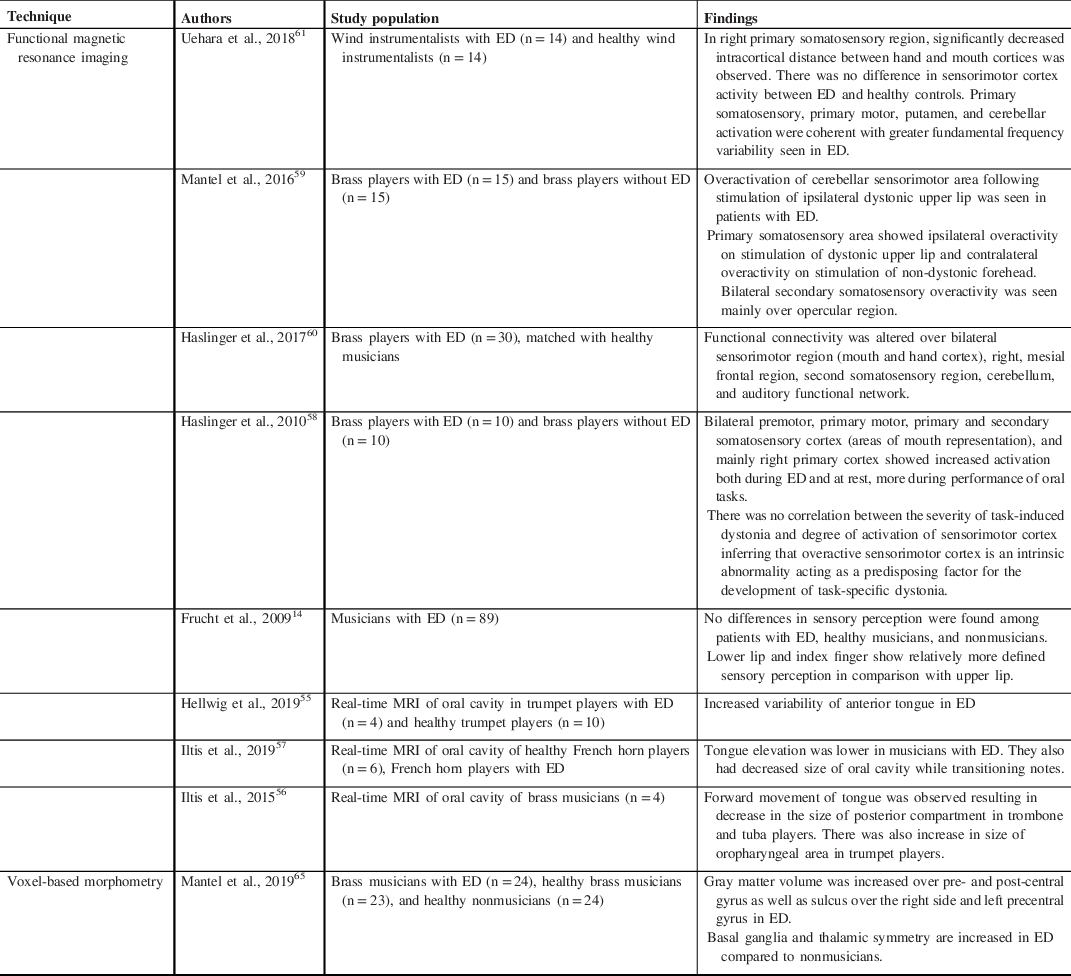
ED = embouchure dystonia.
Several hypotheses have been proposed to explain the pathogenesis of ED. One of the suggested theories is aberrant plasticity of sensorimotor cortex. Functional magnetic resonance imaging (MRI) studies in ED have shown overactivity in sensorimotor region and premotor region, Reference Haslinger, Altenmüller, Castrop, Zimmer and Dresel58 as well as parietal operculum. Reference Mantel, Dresel, Altenmüller, Zimmer, Noe and Haslinger59 Similar results have been replicated in resting-state MRI studies with demonstration of altered functional connectivity in bilateral sensorimotor region over clinically asymptomatic hand cortex, in addition to oral region. Reference Haslinger, Noé and Altenmüller60 The mechanism explaining this finding was maladaptive organization of sensorimotor cortex and altered cortical hyperexcitability. Reference Haslinger, Noé and Altenmüller60 The inappropriate sensory gating by an overactive basal ganglia resulting in abnormal interaction of the somatosensory and motor input is another proposed hypothesis. Reference Haslinger, Altenmüller, Castrop, Zimmer and Dresel58
Structural and connectivity abnormalities of cerebellum have been implicated in ED, Reference Uehara, Furuya, Numazawa, Kita, Sakamoto and Hanakawa61 akin to focal hand dystonia. Reference Delmaire, Vidailhet and Elbaz62–Reference Odergren, Stone-Elander and Ingvar64 In ED, in addition to involvement of primary motor cortex, primary somatosensory cortex, and putamen, activity within cerebellum was associated with dystonic features. Reference Uehara, Furuya, Numazawa, Kita, Sakamoto and Hanakawa61 Gray matter changes Reference Mantel, Altenmüller and Li65 and distorted homunculus Reference Hirata, Schulz, Altenmüller, Elbert and Pantev66,Reference Bulica, Sidiropoulos, Mahajan, Zillgitt, Kaminski and Bowyer67 have also been described in ED (Tables 3 and 4).
Table 4: Pathophysiological insights in ED through electrophysiological studies

MEG-CSI = magnetoencephalography-coherence source imaging; ED = embouchure dystonia.
Upper Limb and Lower Limb Involvement in FTSD
Many factors explain the predisposition of the hand for FTSD. Studies on somatotropic organization of striatum revealed a greater degree of overlap in the hand and mouth areas compared to that of foot. Another possible explanation could be that the area for motor control of hands and face is larger than that of leg. Reference Gerardin, Lehéricy and Pochon68
The rarity of lower limb task-specific dystonia in comparison with the upper limb dystonia could also be due to differential degree of plasticity that occurs in the motor cortex. Reference García-Ruiz, Val, Losada and Campos69
Bassists have not been reported to have musicians’ hand dystonia. They play widely separated notes and hence simultaneous activation of digits while playing seldom occurs. This could prevent overlapping and blurring of cortical representation of digits that are implicated in musicians’ hand dystonia. Reference Conti, Pullman and Frucht19 A similar concept could explain the low incidence of lower limb dystonia. Percussionists have comparatively more focused muscle group activity involving the ankle and hence have a higher predisposition toward dystonia of lower limb. When the focused task becomes concentrated to a smaller group of muscles and becomes intense, the artists are at risk of developing FTSD.
Brain Changes in SD
In a study that compared the functional and structural aberrations among various FTSDs, compared to focal hand dystonia, patients with SD had gray matter volume abnormalities over the cortical representation for the larynx, that is, left superior parietal lobule, right inferior frontal gyrus, and anterior insula. In addition, white matter integrity was impaired in the ventral area of the precentral gyrus in SD and hand area of precentral gyrus in focal hand dystonia. Reference Bianchi, Fuertinger, Huddleston, Frucht and Simonyan54 Another study also found that superior parietal cortex is involved in laryngeal dystonia. They also reported prominent network connectivity between the parietal cortex and frontal and occipital regions in patients with laryngeal dystonia. Superior parietal cortex is essential for higher-order sensorimotor integration. Hence, in patients with laryngeal dystonia, cortices involved in sensorimotor processing are preferentially affected, while focal hand dystonia is characterized by abnormal representation of motor execution cortices that include primary motor cortex and cerebellum. Reference Fuertinger and Simonyan53
Conclusion
ED, FTSD of lower limb in drummers, and SD, although rare, cause significant morbidity among performing artists. Misdiagnosis has been frequently reported in the literature, more so in ED and lower limb dystonia. The symptoms have been frequently ascribed to have musculoskeletal or psychogenic basis. Careful inspection aided with surface EMG will help in diagnosis. Further functional studies will be able to ascertain the differential involvement of motor programs in FTSD of lower limbs in percussionists and nonmusicians.
Conflicts of Interest
There are no conflicts of interest.
Statement of Authorship
Acquisition and interpretation of data and drafting of the review were undertaken by SR. Concept and design of the review and revisions of the manuscript were undertaken by PKP.




