



As a key modifiable risk factor for many chronic metabolic diseases, diet holds considerable potential for clinical and population benefit. It is a factor that people of all ages can theoretically change and improve, particularly with the rising prevalence of obesity and cardiometabolic conditions worldwide(Reference Willett, Rockstrom and Loken1). A better understanding of diet and its malleability could point the way to more effective interventions targeting obesity and metabolic diseases(Reference Gasser, Kerr and Mensah2).
In many studies, dietary intakes are typically assessed at single time points, in part due to the complexity, time and labour-intensive nature of capturing and assessing diets. It is, however, increasingly recognised that the foods people consume can change over time, particularly when people go through different life stages and transition periods. Evolving developmental and nutritional needs and a dynamic food environment would mean that repeated assessment of diet over time rather than a single assessment (at one time point) will be necessary to provide a more accurate representation of dietary exposures or patterns over time. The evolution of diets or dietary changes over time or age is also commonly known as dietary trajectories.
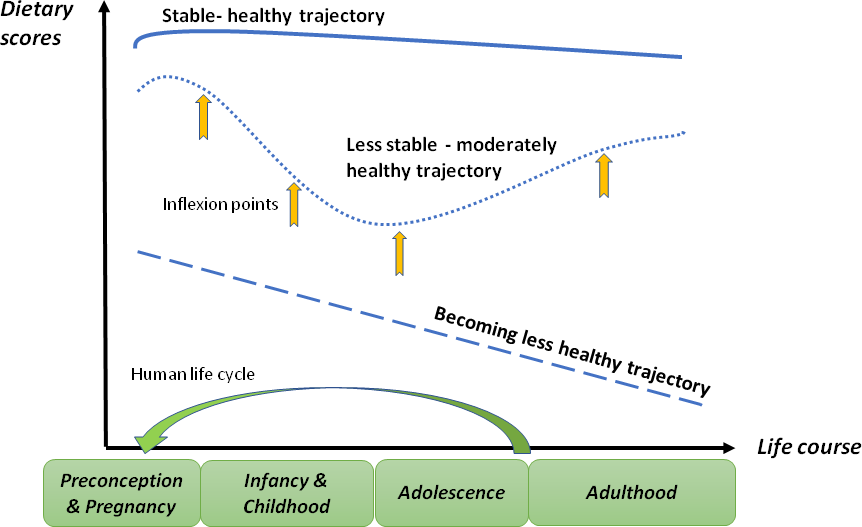
Following the development of several approaches to model longitudinal data(Reference van der Nesta, Lima Passosa and Candela3), the examination of health trajectories (the evolution of health outcomes over age or time) have gained traction over the past decade(Reference Burton-Jeangros, Cullati and Sacker4). Some of these approaches have been applied to examine dietary trajectories, although in limited number of studies(Reference Movassagh, Baxter-Jones and Kontulainen5,Reference Winpenny, Penney and Corder6) . The recent emergence of the group-based trajectory modelling (GBM) method(Reference Nagin7) appears to have turned the tide and since 2019, there has been a stark increase in publications examining dietary trajectories. Unlike previous longitudinal analyses methods which tend to describe trends in dietary intakes or behaviours as a group average over time, GBM accounts for between-individual variation when describing the continuity of different behaviours in a cohort of individuals over time. This approach recognises that subgroups of individuals may present distinct developmental/dietary patterns that vary from the group average and enables subgroups at risk of poor dietary intake to be identified(Reference Doggui, Ward and Johnson8). Additionally, inflexion points (time periods) when individuals experience significant dietary changes are also distinguishable when diets are captured over an extended time frame or across critical life transition periods.
Utilising longitudinal diet data from studies, typically cohort studies, enables the study of the dynamic patterns of dietary changes or stability across different stages of the life course and provide important information about when and in whom to intervene with nutritional interventions, and the likely population that will benefit. It also yields information about the different impact distinct trajectories of dietary patterns have on later health, and the determinants that influence or alter these dietary trajectories. This creates a deeper understanding of the complexity of diet and their patterns and can help in defining which foods and/or diets are amenable to change and at which stage of life(Reference Manohar, Hayen and Do9).
To date, studies which examined dietary trajectories have used different diet parameters to model dietary trajectories. In recent years, the use of empirically derived (generated) dietary patterns and dietary indices appears to be the most common(Reference Appannah, Murray and Trapp10–Reference Wu, Pahkala and Juonala13), although some studies have chosen to focus on specific food groups(Reference Manohar, Hayen and Do9,Reference Winpenny, Winkler and Stochl14) or nutrients(Reference Zhang, Zhang and Du15).
In this article, recent observational studies are reviewed to describe evidence on dietary trajectories through the different life stages, covering early life, adolescence to young adulthood and from mid-to-late adulthood. Accompanying this is a discussion on the insights that can be achieved from longitudinal examination of dietary patterns as compared with cross-sectional dietary assessments. This is concluded by a reflection of the challenges faced in this field of research, future directions and a final highlight of the importance of a life course perspective on diet evolution and changes.
Early life and childhood
Recognition of the importance of nutrition in the first 1000 d has led to growing interest in the tracking of diets during early life. Evidence suggests that early food preferences set the foundation for food choices and eating habits in later childhood and adult life and, consequently, contribute to the prevention and risk reduction of chronic diseases. Moreover, children experience significant developmental shifts in diet selection during early childhood, where ages from 2 to 6 years are peak ages for the development of food neophobia(Reference Scaglioni, De Cosmi and Ciappolino16).
Recent studies (from 2019 onwards) examining dietary trajectories in children younger than 10 years old have mostly adopted the GBM method and generally observed strong stability of empirically derived dietary patterns and/or dietary scores over time in the majority of the children(Reference Gasser, Kerr and Mensah2,Reference Dalrymple, Vogel and Godfrey11,Reference Woo, Reynolds and Summer12) , for example, trajectories reflecting consistent poor, medium or good diet quality over time(Reference Dalrymple, Vogel and Godfrey11) or trajectories reflecting dietary patterns that are ‘never healthy’, ‘moderately healthy’, ‘becoming less healthy’ and ‘always healthy’(Reference Gasser, Kerr and Mensah2). These support findings from earlier (and limited number of) studies which captured two to three time points of dietary intakes but adopted different statistical methods for diet tracking(Reference Lioret, Betoko and Forhan17,Reference Okubo, Crozier and Harvey18) .
Of note is the study by Darymple et al., 2021(Reference Dalrymple, Vogel and Godfrey11), a first to investigate mother–offspring diet quality trajectories from as early as pre-pregnancy till mid-childhood (aged 8–9 years) in the Southampton Women Survey cohort. This study observed diet quality trajectories to be largely stable throughout, reinforcing the notion that dietary patterns are established very early in life and remain largely consistent thereafter.
While these studies have been valuable in identifying early life and socio-demographic determinants of various dietary trajectories and their associated health outcomes, for example, childhood adiposity, studies emerging with rather interesting and novel findings tend to be the ones that cover extended (longer) time frames and focus on selected components of the diet.
For example, Manohar et al, 2021(Reference Manohar, Hayen and Do9) constructed dietary scores based on weekly frequency of core and discretionary foods intakes in children from ages 4 months, 8 months, 1 year, 2 years and 3 years in the Healthy Smiles, Healthy Kids (HSHK) cohort in Australia. They observed that while dietary trajectories of healthy core foods were inconsistent with advancing age (e.g. rapid or gradual increase with early or late decrease), dietary trajectories of unhealthy discretionary foods remained relatively consistent. In general, it was observed that core foods consumption continued to decline after the second year of life, while discretionary foods intake increased markedly between 4 months and 2 years of age. In parallel, Woo et al, 2020(Reference Woo, Reynolds and Summer12) identified and evaluated trajectories of dietary quality in children aged from 3 to 7 years in a longitudinal cohort study (Epidemiology of BMI Rebound Study) of non-Hispanic African American and White children in the USA. Using total Healthy Eating Index 2005 (HEI-2005) score and component scores, five HEI-2005 trajectory groups were identified, of which one declined and one improved over time, while the rest remained stable. While total scores showed that diet quality was generally low at the age of 3 years and remained stable up to the age of 7 years, individual components of the HEI-2005 (such as whole fruit, saturated fats and added sugars) differed significantly across the dietary trajectory groups, and these differences were largely maintained between the age of 3 and 7 years.
Taken together, these findings suggest that the establishment of diet pattern and quality likely occurs primarily before 3 years of age, after which children start to gain more independence over their dietary choices and/or influence their parents’ purchasing behaviour(Reference Kerr, Gillespie and Gasser19). Importantly, these findings allude to the value of examining diets using various diet parameters (e.g. specific food groups and components of diet quality indices) to elucidate different aspects of the diet that can be changed or improved to potentially alter trajectories.
Beyond 3 years of age, the next transition period when dietary changes appear to be significant is approximately the period of 7–9 years of age. In a uniquely long-term study that followed children over a substantial period of childhood (> 10 years), Gasser et al, 2017(Reference Gasser, Kerr and Mensah2) derived and compared longitudinal trajectories of dietary scores and patterns from 2–3 to 10–11 years and from 4–5 to 14–15 years of age in the Baby Cohort and Kindergarten Cohort of the Longitudinal Study of Australian Children, respectively. While moderately high stability of dietary scores in both cohorts of children across four trajectories were observed, it was remarkable to note that for the trajectories characterised by changing levels of healthiness or unhealthiness with age, diets tended to change at approximately 7 years of age for both cohorts. For example, the ‘healthy’ factor scores for the ‘becoming less healthy’ trajectories began to worsen rapidly from approximately 7 years of age, while the ‘unhealthy’ factor scores for the ‘becoming unhealthy’ trajectories began to increase rapidly at the age of 7 years for both cohorts, and even more rapidly from approximately 9 years onwards for the Baby Cohort. The authors suggested that this dietary deterioration from the age of 7 years onwards occurred after children had attended primary school for about 2 years, thus likely reflecting another inflection point in the childhood period.
It thus appears that frequent repeated reporting over an extended time frame has the advantage of providing a longer-term picture of children’s diets over time and allows the capture of ‘windows of change’ when diets are likely to change, in part due to influence of peers and other environmental factors.
Adolescence to young adulthood
The period of late adolescence to early adulthood has been suggested to be an important but oft-overlooked age for the establishment of long-term health behaviour patterns. This is the period when individuals experience major transitions, including changes in the home and social environment, moving from family dependence to towards stronger peer networks and financial independence. Many of these factors have shown associations with diet and eating behaviours(Reference Winpenny, Penney and Corder6).
Poor diet quality is common during adolescence and has been linked with the early onset of chronic disease risk factors such as obesity and a high abdominal waist circumference. Poor lifestyle behaviours may become embedded during young adulthood, a high-risk period for excess weight gain. As such, the transition from adolescence to young adulthood is believed to be is a critical period for interventions to reduce chronic disease risk and prevents the transgenerational cycle of obesity and related diseases(Reference Appannah, Murray and Trapp10).
Recent studies have been conducted to fill the knowledge gap in understanding changes in dietary intakes and behaviours between the age of 13 and 30 years, particularly beyond the early twenties. Winpenny and team examined participants aged from 14 to 30 years from the Norwegian Longitudinal Health Behaviour Study, who provided responses to specific questions on intakes of fruit, vegetables, confectionery and sugar-sweetened beverages. Using latent growth curve models, fruit and vegetable intakes were observed to decline from the age of 14 years to the age of 23 and 21 years, respectively, before increasing to the age of 30 years. Sugar-sweetened beverages and confectionery intakes increased to the age of 18 years, before subsequently decreasing(Reference Winpenny, van Sluijs and White20).
Separately, in a study from the Western Australian Pregnancy Cohort (Raine Study)(Reference Appannah, Murray and Trapp10), two major sex-specific diet trajectories were identified (using GBM) from food frequency data collected from participants when they were in the age of 14, 17, 20 and 22 years. A majority of males and females fell into a trajectory of consistently below-average healthy pattern scores, while the remaining showed modest declines in healthy pattern scores after late adolescence, with this being most evident in females. Of greater concern was the trajectory in which the less healthy Western pattern scores showed year-on-year increases from the age of 16 years onwards, particularly in males.
Further insights into the importance of examining sex subgroups can be gleaned from the study by Doggui et al, 2021(Reference Doggui, Ward and Johnson8). They examined trajectories of eating behaviours during adolescence, including breakfast consumption, fruits and vegetables, sugary beverages and fast-food consumption, in Canadian participants of the MATCH study and followed them from the age of 11 to 18 years. While they did not observe an inflection point or age when significant changes were observed, the study highlighted the heterogeneity in eating behaviours among adolescents and the need for sex-specific interventional approaches during adolescence.
Taken together, these and other studies(Reference Movassagh, Baxter-Jones and Kontulainen5,Reference Wu, Pahkala and Juonala13) highlighted a key inflection point during the period of adolescence and early adulthood, during which significant dietary changes would typically occur. While these findings continue to emphasise the importance of establishing a healthy diet from as early as in childhood, they further suggest that the transition from early to middle adulthood may provide another opportunity for interventions to improve diet behaviours and for greater effectiveness, it should be differentiated for sex subgroups.
Mid-to-late adulthood
By mid-adulthood, eating and lifestyle habits are set in place and any modifications would likely to be more challenging to enforce(Reference Todd, Street and Ziviani21). Does this make positive dietary changes in adulthood less important or less urgent? Are there still benefits in making positive dietary changes during mid-life? Recent studies examining dietary trajectories during adulthood (from mid-life to late life) suggest that changes in patterns of dietary intake even during mid-adulthood can have consequences for many chronic conditions in later life.
In the Baltimore Longitudinal Study of Aging, changes in dietary pattern over time were assessed in participants aged 30 to 59 years and associations to subsequent impairments in physical function examined(Reference Talegawkar, Jin and Xue22). Based on adherence to the Alternative Healthy Eating Index-2010 (AHEI), two dietary trajectories were generated – ‘greatly improved’ and ‘moderately improved’. Participants in the ‘greatly improved’ trajectory showed a trend in overall AHEI score from poor/intermediate to good diet categories across dietary assessments with age over time, whereas for those in the ‘moderately improved’ trajectory, the overall AHEI score shifted from poor to intermediate diet categories over time, with the prevalence of the good diet category remaining low. At older age, those in the ‘moderately improved’ trajectory had poorer physical function than those in the ‘greatly improved’ trajectory suggest that improving diet quality even in middle age may contribute to better health outcomes at older ages.
Dietary pattern trajectories were also examined in adults aged 18 years or older from the China Health and Nutrition Survey between 1991 and 2018, in relation to the risk of overweight and obesity(Reference Zhang, Wang and Wang23). It was observed that participants who followed the trajectory with highest initial score and then a slight decrease of the meat dietary pattern (characterised by high intakes of organ meats, poultry, pork and other livestock meat) were associated with greater risk of overweight and obesity when compared with those in the lowest initial score trajectory, suggesting that long-term higher adherence to the meat dietary pattern may increase the risk of overweight and obesity. In contrast, those with high adherence to the southern and modern dietary patterns trajectories (characterised by rice, vegetables, pork and fruits, dairy products and processed foods, respectively) were associated with lower risks of overweight and obesity.
Exemplified by the above two studies, the value of studying dietary trajectories in adulthood appears to be twofold. Firstly, examining long-term diet trends at a population level can reveal shifts in eating patterns as countries undergo epidemiological and accompanying nutrition transitions, which often dynamically change the food environment. Secondly, the longer-term impact or influence of adhering to particular diets on the development of chronic diseases is illuminated and therefore better elucidated when diets are assessed at multiple time points over a longer period, within a life stage and/or across life stages.
Challenges in examining dietary trajectories
Whilst valuable, examining dietary trajectories is not without its challenges and limitations. Most trajectory modelling methods including the GBM require at least three time points or three waves of dietary data, which implies that studies examining dietary trajectories have to be longitudinal in design and ideally continue for a certain number of years in order to capture developmental stages or transition periods.
To study changes in diet over time, the same dietary assessment tool should preferably be administered consistently throughout the time period, so as to minimise the measurement error due to variation in assessment methods. This, however, can be challenging as researchers strike the balance between administering a measure that is not too burdensome for participants and yet captures sufficient detail. This is particularly so for studies administering the FFQ, which is comprehensive but often time-consuming to administer. An added complexity for studies capturing development data is the need to use different age-appropriate FFQ to adapt to the expanding range of foods in the diet.
Some studies have attempted to overcome inconsistencies in assessment tools by using various methods of standardisation, for example, having food groups grouped in the same way(Reference Dalrymple, Vogel and Godfrey11,Reference Wu, Pahkala and Juonala13) or checking that diets have quantitatively similar factor loadings (using Tucker’s congruence coefficient) before tracking them(Reference Lee, Colega and Sugianto24,Reference Lorenzo-Seva and Berge25) .
An alternative is to use abbreviated dietary questionnaires such as capturing frequencies of consumption of only a selected range of food groups of interests, for example, only asking about consumption of a range of twelve to sixteen healthy and less healthy food or drinks consumed in the previous 24 h(Reference Gasser, Kerr and Mensah2) or a few questions on frequency of consumption of certain food groups such as fruits, vegetables, sugar-sweetened drinks and fast food(Reference Winpenny, van Sluijs and White20). These questionnaires have the advantages of brevity and ease of administration. In the Gasser et al study(Reference Gasser, Kerr and Mensah2), the brevity of such abbreviated questionnaire facilitated its quick and high completion rates and, importantly, enabled its repeated administration in this National Longitudinal Study every 2 years. This is a major feat for a diet assessment tool, considering the competing demands from measurements from other domains within a cohort study. An abbreviated dietary questionnaire may also be particularly useful for younger age groups whose amounts of foods consumed maybe harder to quantify and perhaps not be as meaningful compared with understanding the diversity for their diet(Reference Manohar, Hayen and Do9).
The trade-off of an abbreviated dietary assessment tool is that, unless it is validated, it remains unclear how accurately the tool measures actual diet. For example, it is not known if the tool overestimates the healthiness of the trajectories and if more or different dietary patterns would have been yielded from a more detailed capture of total diets(Reference Gasser, Kerr and Mensah2).
It is important to recognise that statistical methods have their limitations and accompanying assumptions. In GBM, the error variance is assumed to be the same for all classes (trajectory groups) and time points, in other words, no inter-individual differences in change within class(Reference Nagin7). Other longitudinal modelling methods should be explored (e.g. in sensitivity analyses) to confirm the reproducibility of the findings from GBM. For example, the use of growth mixture modelling, another latent class modelling technique, allows for a varying covariance structure within each class and thus provides a greater flexibility(Reference Burton-Jeangros, Cullati and Sacker4,Reference Dalrymple, Vogel and Godfrey11) .
Future directions: beyond dietary trajectories
Beyond the focus on the associations of diet trajectories and disease risk, recent emerging studies are using pattern analyses as an integrative approach to investigate the clustering and correlations among various lifestyle factors. Lifestyle patterns are identified and subsequently assessed as predictors of disease risk(Reference Zheng, Lioret and Hesketh26). Some studies have developed lifestyle scores, and in addition to diet, they incorporate several modifiable lifestyle factors such as smoking, obesity and physical activity(Reference Schulz, Oluwagbemigun and Nothlings27).
This holistic approach is in line with growing evidence showing that elements of lifestyle, from diet to movement behaviours and sleep, are inter-related and may act in additive or synergistic ways to influence disease risk and prevention such as obesity development(Reference D’Souza, Kuswara and Zheng28) and cardiovascular risk(Reference Barbaresko, Rienks and Nothlings29).
Of note are recent studies by Zheng et al, 2021(Reference Zheng, Lioret and Hesketh26) who examined longitudinal trajectories of lifestyle patterns and BMI in children aged 18 to 60 months who participated in the Melbourne InFANT Program and Lee et al, 2021(Reference Lee, Yang and Wolever30) who identified distinct health behaviour trajectories in high-cardiovascular-risk populations and determined the trajectory associated with improved cardiovascular risk outcomes a year later.
This widening of perspective, combined with advancing statistical approaches employed in epidemiological research, opens up potential opportunities for integrating other aspects of diet (such as eating behaviours, time of eating and eating locations), high-dimensional biomarkers (such as metabolome and the microbiome)(Reference Johnson, Vanderlinden and DeFelice31,Reference Oluwagbemigun, Foerster and Watkins32) and perhaps even genetic make-up into current diet and lifestyle pattern analyses. The inclusion of these factors may provide deeper insights and contribute to mechanistic understanding of diet–disease relationships and support the development of lifestyle disease prevention recommendations stratified for population groups(Reference Schulz, Oluwagbemigun and Nothlings27).
Conclusion
Science has evolved to focus on the importance of healthy dietary patterns over time. This is reflected in the recent USDA Dietary Guidelines, which for the first time since the 1985 edition, contain specific recommendations for all life stages, including infants and toddlers, and pregnant and lactating women.
It is recognised that each life stage is distinct and has unique needs that influence health and well-being. While early food preferences establish the foundation for food choices and eating habits in later childhood and adult life, it is increasingly clear that every life stage provides an opportunity to make food choices that promote health and well-being, achieve and maintain appropriate weight status, and reduce the risk of diet-related chronic disease(33).
Growing evidence now suggest that the study of dietary trajectories may be more meaningful than single-point dietary measurements. Dietary trajectories have the potential to reveal how improvements in diet at particular life stages can affect health outcomes, which is important considering the global endeavour to close the gap between life expectancy and healthy life expectancy(Reference Cao, Hou and Zhang34). Additionally, by identifying population groups with suboptimal dietary patterns and their associated demographic and environmental factors, these groups can benefit from targeted dietary or lifestyle-modifying interventions to prevent or at least delay the incidence of chronic diseases. As diet continues to be a cornerstone for health promotion and disease prevention strategies, a longer-term understanding of dietary trajectories and the specific time point(s) at which interventions and programmes are promising will be the way forward.
Acknowledgements
Mary Chong is solely responsible for the conceptulization, investigation, methodology, visualization, writing and reviewing of this manuscript.
Nil.
There are no conflicts interest.
