
148 results
53 2-Back Performance Does Not Differ Between Cognitive Training Groups in Older Adults Without Dementia
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 360-361
-
- Article
-
- You have access
- Export citation
2 Higher White Matter Hyperintensity Load Adversely Affects Pre-Post Proximal Cognitive Training Performance in Healthy Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 671-672
-
- Article
-
- You have access
- Export citation
1 Task-Based Functional Connectivity and Network Segregation of the Useful Field of View (UFOV) fMRI task
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 606-607
-
- Article
-
- You have access
- Export citation
78 BVMT-R Learning Ratio Moderates Cognitive Training Gains in Useful Field of View Task in Healthy Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 180-181
-
- Article
-
- You have access
- Export citation
6 Adjunctive Transcranial Direct Current Stimulation and Cognitive Training Alters Default Mode and Frontoparietal Control Network Connectivity in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 675-676
-
- Article
-
- You have access
- Export citation
9 Connecting memory and functional brain networks in older adults: a resting state fMRI study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 527-528
-
- Article
-
- You have access
- Export citation
Advocacy at the Eighth World Congress of Pediatric Cardiology and Cardiac Surgery
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 24 August 2023, pp. 1277-1287
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Promoting occupational justice policies in mental health organizations: A model based on the experiences of mental health rehabilitation consumers and employees
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S539-S540
-
- Article
-
- You have access
- Open access
- Export citation
Patient iPSC-derived neurons reveal mechanisms underlying antidepressant response: a potential diagnostic tool
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S92-S93
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Depression is a leading cause of disability worldwide despite dozens of approved antidepressants. There are currently no clear guidelines to assist the physician in their choice of drug, with existing tools limited to pharmacogenetics that have shown suboptimal response prediction outcomes resulting in a subscription process that is largely a trial and error one. Consequently, the majority of depressed patients do not respond to their first prescribed antidepressant, with >30% not responding to subsequent drugs. We report here on molecular readouts from an in vitro-based platform that provides patient-specific information on antidepressant mechanisms using cortical neurons derived individually from each patient.
ObjectivesTo assess gene expression differences in prefrontal cortex neurons derived from responders and non-responders to two commonly used antidepressants, the selective serotonin reuptake inhibitor Citalopram and the atypical antidepressant Bupropion.
MethodsPatient-derived lymphoblastoid cell lines from the Sequenced Treatment Alternatives to Relieve Depression (STARD) study with known response to Citalopram or Bupropion were reprogrammed and then differentiated to cortical neurons. Differential gene expression analysis was preformed to identify genes that are differentially expressed between drug responders and non-responders.
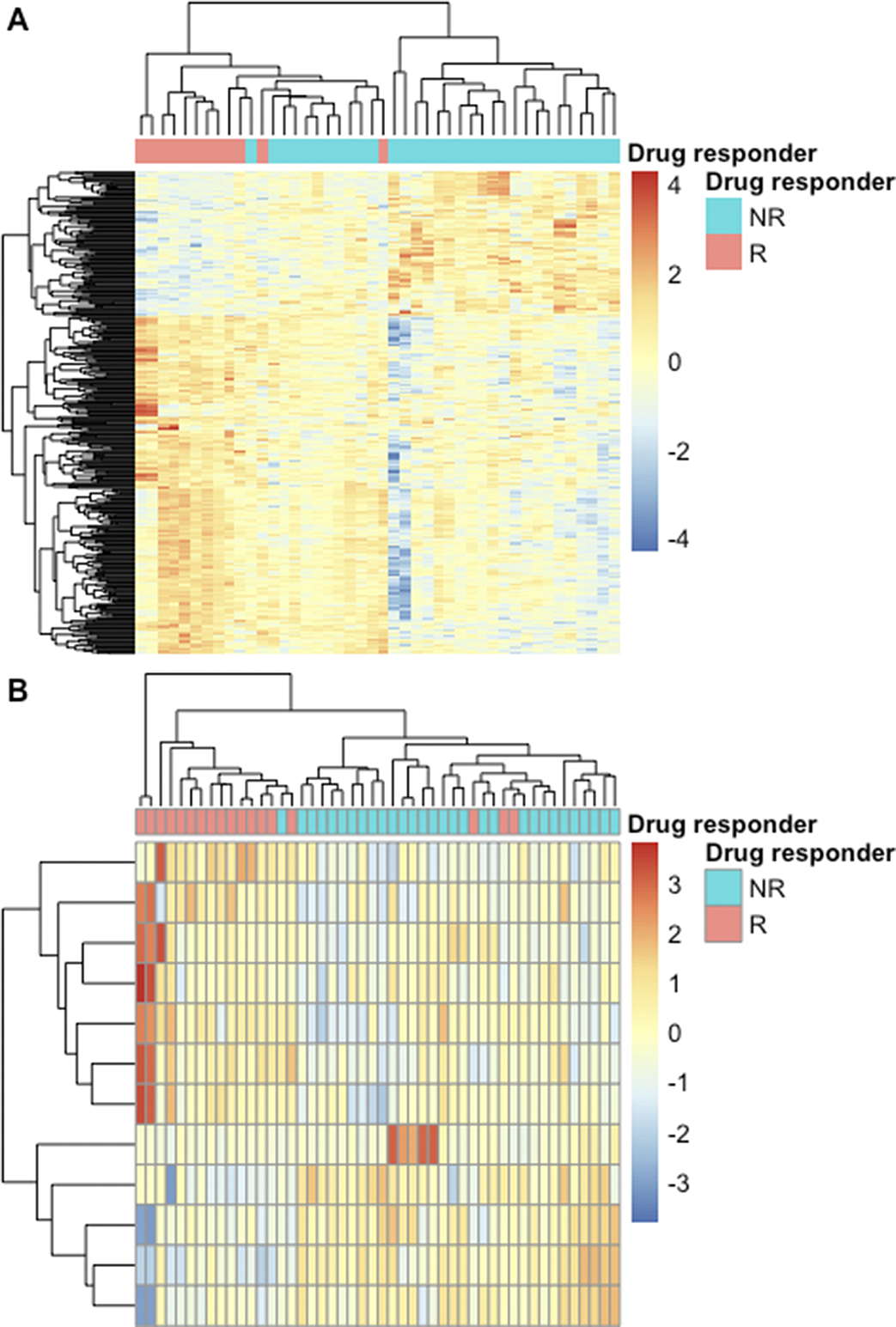
ResultsSignificant differential expression was shown in 359 genes between Bupropion responders and non-responders (Fig1A) and 12 genes between Citalopram responders and non-responders (Fig1B). Clustering on the differentially expressed genes showed high agreement with the known response to both drugs (Fig1). Functional enrichment analysis revealed biologically relevant pathways that differ between responders and non-responders in Bupropion versus Citalopram.
Image:
Figure 1.
Heatmap of the expression of genes that show significant differential expression between neurons derived from Bupropion (A) and Citalopram (B) responders and non-responders. Color is the scaled gene expression; lines are genes and columns are samples. Column side colors represent the known response of the patient. Colum and line dendrograms are unsupervised hierarchical clustering.
 Conclusions
ConclusionsGene expression patterns of neurons derived from patients with depression differ according to their response to two common antidepressants from different groups. The identification of distinct drug response dependent expression patterns in derived neurons can help elucidate mechanisms underlying antidepressant activity, supporting new drug development and response prediction.
Disclosure of InterestNone Declared

Challenges of Documenting Historic Water Systems: Integrating Open-Source Water Data with Archaeological Datasets in Utah
-
- Journal:
- Advances in Archaeological Practice / Volume 11 / Issue 2 / May 2023
- Published online by Cambridge University Press:
- 31 January 2023, pp. 211-223
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A neuropsychologically based employment intervention for women with multiple sclerosis: A quasi-randomized controlled trial
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue 4 / May 2023
- Published online by Cambridge University Press:
- 05 September 2022, pp. 388-396
-
- Article
- Export citation
Direct and indirect predictors of medication adherence by adults with bipolar disorder
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S404
-
- Article
-
- You have access
- Open access
- Export citation
Quantitative Compositional Wavelength-Dispersive Mapping of Particles from the Moon.
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 612-613
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Bacterial infections and antibiotic utilization varies by coronavirus disease 19 (COVID-19) severity in hospitalized cancer patients: Analysis from the first phase of the pandemic
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 26 May 2022, pp. 413-419
- Print publication:
- March 2023
-
- Article
- Export citation
P.059 Results From the Randomized and Open-Label Periods of the CENTAUR Trial of Sodium Phenylbutyrate and Ursodoxicoltaurine in Amyotrophic Lateral Sclerosis (ALS)
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 48 / Issue s3 / November 2021
- Published online by Cambridge University Press:
- 05 January 2022, p. S35
-
- Article
-
- You have access
- Export citation
Direct maxillary irrigation therapy in non-operated chronic sinusitis: a prospective randomised controlled trial
-
- Journal:
- The Journal of Laryngology & Otology / Volume 136 / Issue 3 / March 2022
- Published online by Cambridge University Press:
- 01 September 2021, pp. 229-236
- Print publication:
- March 2022
-
- Article
- Export citation
Variable duration of viral shedding in cancer patients with coronavirus disease 2019 (COVID-19)
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 27 August 2021, pp. 1413-1415
- Print publication:
- October 2022
-
- Article
- Export citation
2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients: Developed in collaboration with and endorsed by the Heart Rhythm Society (HRS), the American College of Cardiology (ACC), the American Heart Association (AHA), and the Association for European Paediatric and Congenital Cardiology (AEPC). Endorsed by the Asia Pacific Heart Rhythm Society (APHRS), the Indian Heart Rhythm Society (IHRS), and the Latin American Heart Rhythm Society (LAHRS).
- Part of
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 11 / November 2021
- Published online by Cambridge University Press:
- 02 August 2021, pp. 1738-1769
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients: executive summary: Developed in collaboration with and endorsed by the Heart Rhythm Society (HRS), the American College of Cardiology (ACC), the American Heart Association (AHA), and the Association for European Paediatric and Congenital Cardiology (AEPC). Endorsed by the Asia Pacific Heart Rhythm Society (APHRS), the Indian Heart Rhythm Society (IHRS), and the Latin American Heart Rhythm Society (LAHRS).
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 11 / November 2021
- Published online by Cambridge University Press:
- 30 July 2021, pp. 1717-1737
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nomenclature for Pediatric and Congenital Cardiac Care: Unification of Clinical and Administrative Nomenclature – The 2021 International Paediatric and Congenital Cardiac Code (IPCCC) and the Eleventh Revision of the International Classification of Diseases (ICD-11)
- Part of
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 7 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. 1057-1188
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
