
113 results
Psychological aspects of vestibular disorders: a national survey of clinical practice
-
- Journal:
- The Journal of Laryngology & Otology , First View
- Published online by Cambridge University Press:
- 22 April 2024, pp. 1-9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The equitable impact of sugary drink taxation structures on sugary drink consumption among Canadians: a modelling study using the 2015 Canadian Community Health Survey-Nutrition
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 15 April 2024, e121
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Increasing the equitability of data citation in paleontology: capacity building for the big data future
-
- Journal:
- Paleobiology / Volume 50 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 28 December 2023, pp. 165-176
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
80 Implications of Body Mass Index on Executive Functioning in Clinically Diagnosed Neurodiverse Children
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 72-73
-
- Article
-
- You have access
- Export citation
The Advancing Mental Health Equality Collaborative: Using Quality Improvement to Advance Equality in Mental Health Care – CORRIGENDUM
-
- Journal:
- BJPsych Open / Volume 9 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 23 October 2023, e199
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Colonization with extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in Botswana
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s81
-
- Article
-
- You have access
- Open access
- Export citation
-
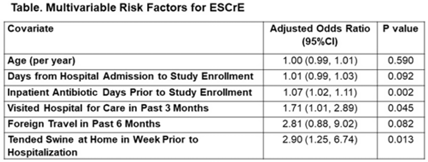
Background: The epidemiology of extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in low- and middle-income countries (LMICs) is poorly described. Although risk factors for ESCrE clinical infection have been studied, little is known of the epidemiology of ESCrE colonization. Identifying risk factors for ESCrE colonization, which can predispose to infection, is therefore critical to inform antibiotic resistance reduction strategies. Methods: This study was conducted in 3 hospitals located in 3 districts in Botswana. In each hospital, we conducted ongoing surveillance in sequential units hospitalwide. All participants had rectal swabs collected which were inoculated onto chromogenic media followed by confirmatory testing using MALDI-TOF MS and VITEK-2. Data were collected via interview and review of the inpatient medical record on demographics, comorbidities, antibiotic use, healthcare exposures, invasive procedures, travel, animal contact, and food consumption. Participants with ESCrE colonization (cases) were compared to noncolonized participants (controls) using bivariable and multivariable analyses to identify risk factors for ESCrE colonization. Results: Enrollment occurred from January 15, 2020, to September 4, 2020, and 469 participants were enrolled. The median age was 42 years (IQR, 31–58) and 320 (68.2%) were female. The median time from hospital admission to date of sampling was 5 days (IQR, 3–12). There were 179 cases and 290 controls (ie, 38.2% of participants were ESCrE colonized). Independent risk factors for ESCrE colonization were a greater number of days on antibiotic, recent healthcare exposure, and tending swine prior to hospitalization. (Table). Conclusions: ESCrE colonization among hospitalized patients was common and was associated with several exposures. Our results suggest prior healthcare exposure may be important in driving ESCrE. The strong link to recent antibiotic use highlights the potential role of antibiotic stewardship interventions for prevention. The association with tending swine suggests that animal husbandry practices may play a role in community exposures, resulting in colonization detected at the time of hospital admission. These findings will help to inform future studies assessing strategies to curb further emergence of hospital ESCrE in LMICs.
Disclosures: None

An approach for collaborative development of a federated biomedical knowledge graph-based question-answering system: Question-of-the-Month challenges
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 14 September 2023, e214
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring potential mental health spillover effects among caregivers and partners of youth in Sierra Leone: A qualitative study
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 10 / 2023
- Published online by Cambridge University Press:
- 18 July 2023, e40
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Advancing Mental Health Equality Collaborative: Using Quality Improvement to Advance Equality in Mental Health Care
-
- Journal:
- BJPsych Open / Volume 9 / Issue S1 / July 2023
- Published online by Cambridge University Press:
- 07 July 2023, pp. S85-S86
-
- Article
-
- You have access
- Open access
- Export citation
Imaging and Molecular Annotation of Xenographs and Tumours (IMAXT): High throughput data and analysis infrastructure
-
- Journal:
- Biological Imaging / Volume 3 / 2023
- Published online by Cambridge University Press:
- 14 April 2023, e11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Expanding mental health services in low- and middle-income countries: A task-shifting framework for delivery of comprehensive, collaborative, and community-based care
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 10 / 2023
- Published online by Cambridge University Press:
- 27 February 2023, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
5 - Working Class: The Essential Workers
- from Part III - Economic Inequality Affects Us All
-
-
- Book:
- The Psychology of Poverty, Wealth, and Economic Inequality
- Published online:
- 13 December 2022
- Print publication:
- 05 January 2023, pp 94-115
-
- Chapter
- Export citation
The impact of actively open-minded thinking on social media communication
-
- Journal:
- Judgment and Decision Making / Volume 13 / Issue 6 / November 2018
- Published online by Cambridge University Press:
- 01 January 2023, pp. 562-574
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An alternative approach for eliciting willingness-to-pay: A randomized Internet trial
-
- Journal:
- Judgment and Decision Making / Volume 2 / Issue 2 / April 2007
- Published online by Cambridge University Press:
- 01 January 2023, pp. 96-106
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Relationship building in pediatric research recruitment: Insights from qualitative interviews with research staff
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 03 October 2022, e138
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
8 - Parent–Child Interaction and Its Impact on Language Development
- from Part One - Factors Influencing Language Development
-
-
- Book:
- Language Development
- Published online:
- 11 August 2022
- Print publication:
- 25 August 2022, pp 166-192
-
- Chapter
- Export citation
Quick and Correlative TOF-SIMS Analysis of Dispersoid Content in Powder Feedstock and Printed Oxide Dispersion Strengthened Alloys
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 954-956
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Multistate outbreak of Salmonella Mbandaka infections linked to sweetened puffed wheat cereal – United States, 2018
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 20 June 2022, e135
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Multi-modal assessment of reward functioning in adolescent anhedonia
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 10 / July 2023
- Published online by Cambridge University Press:
- 17 June 2022, pp. 4424-4433
-
- Article
- Export citation
