
249 results
Testing maternal effects of vitamin-D and omega-3 levels on offspring neurodevelopmental traits in the Norwegian Mother, Father and Child Cohort Study
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 09 September 2024, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Depressive symptoms in adolescence and adult educational and employment outcomes: a structured life course analysis
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 31 May 2024, pp. 1-8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A global pilot comparative, cross-sectional study of clinical research nurses/research midwives: Definition, knowledge base, and communication skills related to the conduct of decentralized clinical trials
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 06 May 2024, e90
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A Systems-Thinking Model of Data Management and Use in US Archaeology
- Part of
-
- Journal:
- Advances in Archaeological Practice / Volume 12 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 20 February 2024, pp. 53-59
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The predictive role of symptoms in COVID-19 diagnostic models: A longitudinal insight
-
- Journal:
- Epidemiology & Infection / Volume 152 / 2024
- Published online by Cambridge University Press:
- 22 January 2024, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Evaluating indwelling devices and other risk factors for mortality in invasive Carbapenem-resistant Enterobacterales infections in Georgia, 2012–2019
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 02 January 2024, e254
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Increasing the equitability of data citation in paleontology: capacity building for the big data future
-
- Journal:
- Paleobiology / Volume 50 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 28 December 2023, pp. 165-176
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
98 On Combining In-Person and Remote National Alzheimer’s Coordinating Center (NACC) Uniform Data Set (UDS) data
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 500-501
-
- Article
-
- You have access
- Export citation
4 Initial Application of Constraint-Induced Cognitive Therapy to Long COVID Brain Fog
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 598-599
-
- Article
-
- You have access
- Export citation
A new view of hillforts in the Andes: expanding coverage with systematic imagery survey
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Infant epigenetic aging moderates the link between Black maternal childhood trauma and offspring symptoms of psychopathology
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 29 September 2023, pp. 1-13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Carbapenemase genes and mortality in patients with carbapenem-resistant Enterobacterales, Atlanta, Georgia, 2011–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s12-s13
-
- Article
-
- You have access
- Open access
- Export citation
-
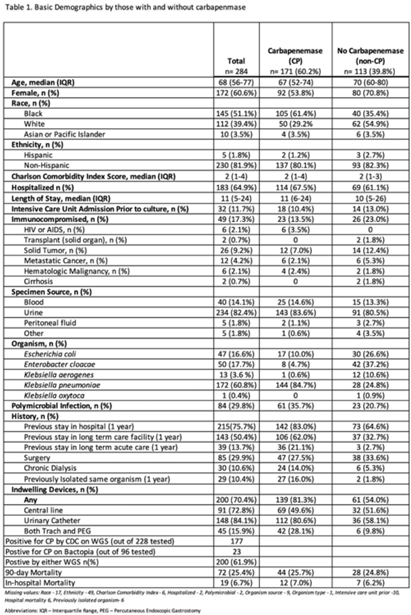
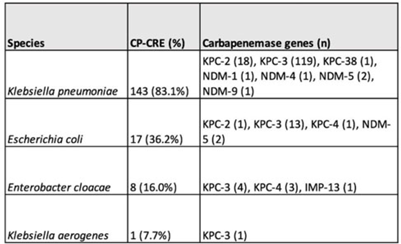
Background: Carbapenemase genes in carbapenem-resistant Enterobacterales (CP-CRE) may be transmitted between patients and bacteria. Reported rates of carbapenemase genes vary widely, and it is unclear whether having a carbapenemase gene portends worse outcomes given that all patients with CRE infections have limited treatment options. Methods: Using active population- and laboratory-based active surveillance data collected by the US CDC-funded Georgia Emerging Infections Program from 2011 to 2020, we assessed the frequency of carbapenemase genes in a convenience sample of CRE isolates using whole-genome sequencing (WGS), and we investigated risk factors for carbapenemase positivity. Only the first isolate per patient in a 30-day period was included. We compared characteristics of patients with CP-CRE and non–CP-CRE. Using multivariable log binomial regression, we assessed the association of carbapenemase gene positivity and 90-day mortality. Results: Of 284 CRE isolates, 171 isolates (60.2%) possessed a carbapenemase gene (Table 1), and KPC-3 was the most common carbapenemase gene (80.7%), with only 7 isolates possessing NDM (Table 2). No isolates possessed >1 carbapenemase gene, and most isolates were from urine (82.4%) (Table 1). Carbapenemase gene positivity was associated with lower age, male sex, black race, infection with Klebsiella pneumoniae, polymicrobial infection, having an indwelling medical device, receiving chronic dialysis, and prior stay in a long-term acute-care hospital, long-term care facility, and/or prior hospitalization in the last year. The 90-day mortality rates were similar in patients with non–CP-CRE and CP-CRE: 24.8% versus 25.7% (P = .86). In multivariable analysis, carbapenemase gene presence was not associated with 90-day mortality (adjusted risk ratio, 0.82; 95% CI, 0.50–1.35) when adjusting for CCI, infection with Klebsiella pneumoniae, and chronic dialysis use. Conclusions: The frequency of CP-CRE among CRE was high in this study, but unlike prior studies, the 90-day mortality rates wer similar in patients with CP-CRE compared to non–CP-CRE. Our results provide novel associations (eg, lower age, male sex, infection with Klebsiella pneumoniae, and indwelling medical devices) that infection preventionists could use to target high-risk patients for screening or isolation prior to CP-CRE detection.
Disclosure: None


Investigation of the first cluster of Candida auris cases among pediatric patients in the United States―Nevada, May 2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s118-s119
-
- Article
-
- You have access
- Open access
- Export citation
Pharmacogenetics of angiotensin modulators according to APOE-ϵ4 alleles and the ACE insertion/deletion polymorphism in Alzheimer’s disease
-
- Journal:
- Acta Neuropsychiatrica / Volume 35 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 22 August 2023, pp. 346-361
-
- Article
- Export citation
Recovery trajectories of IQ after pediatric TBI: A latent class growth modeling analysis
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 3 / March 2024
- Published online by Cambridge University Press:
- 21 August 2023, pp. 273-284
-
- Article
- Export citation
Strategies to build a positive and inclusive Antarctic field work environment
-
- Journal:
- Annals of Glaciology / Volume 63 / Issue 87-89 / September 2022
- Published online by Cambridge University Press:
- 11 July 2023, pp. 125-131
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Stress and Coping Strategies Among Those Affected by Ebola Virus Disease (EVD) Epidemic in Sierra Leone, West Africa
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, pp. s161-s162
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Family involvement, patient safety and suicide prevention in mental healthcare: ethnographic study
-
- Journal:
- BJPsych Open / Volume 9 / Issue 2 / March 2023
- Published online by Cambridge University Press:
- 23 March 2023, e54
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
