
1540 results
Molecular and Epidemiological Characterization of Pediatric and Adult C. difficile Infection in Canadian Hospitals, 2015-2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s10-s11
-
- Article
-
- You have access
- Open access
- Export citation
-
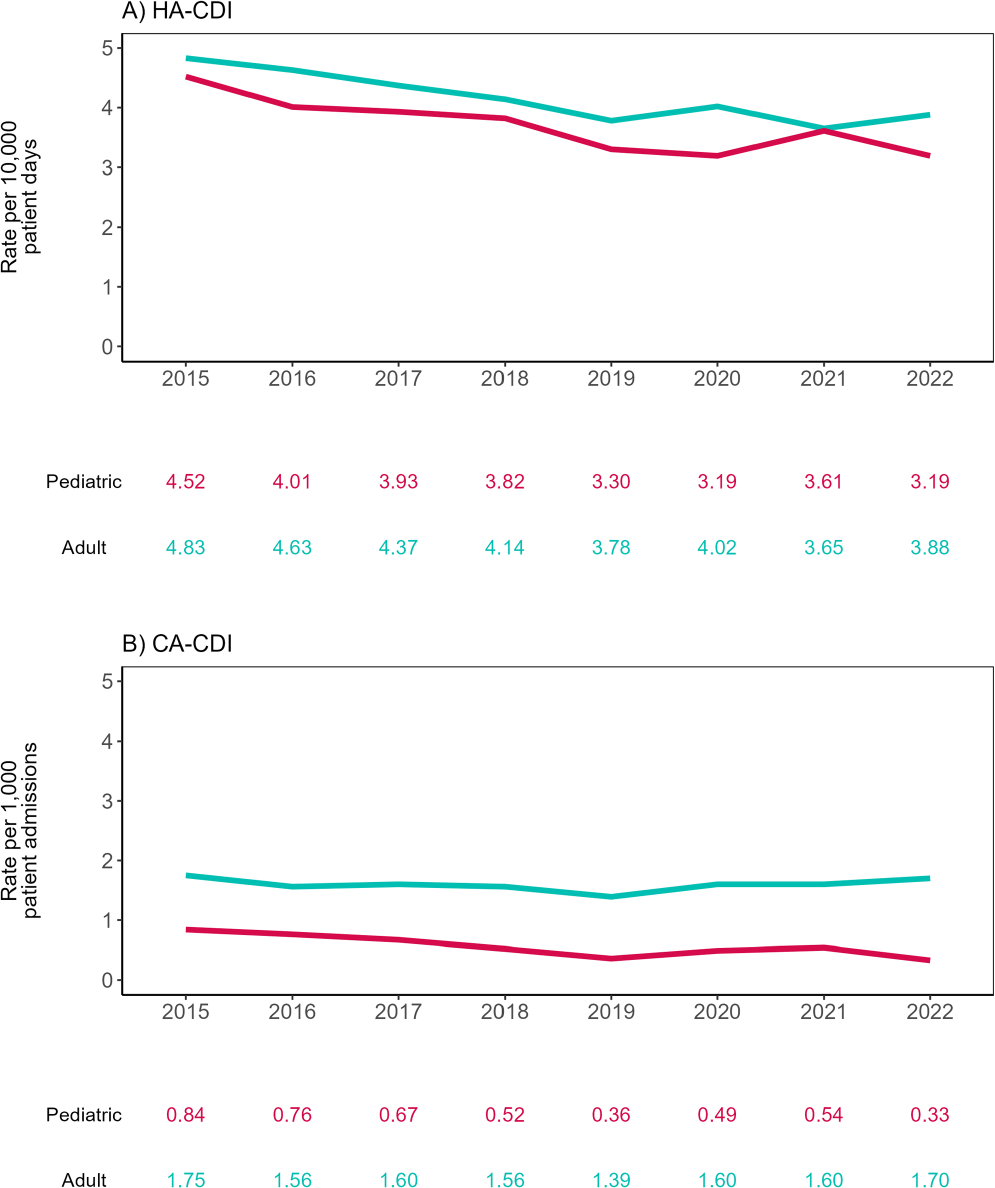
Background: The molecular and epidemiological landscape of C. difficile infection (CDI) has evolved markedly in the last decade; however, limited information is available contrasting differences between adult and pediatric populations. We describe a multicenter study evaluating healthcare-associated (HA) and community-associated (CA) adult and pediatric-CDI identified in the Canadian Nosocomial Infection Surveillance Program (CNISP) network from 2015 to 2022. Methods: Hospitalized patients with CDI were identified from up to 84 hospitals between 2015–2022 using standardized case definitions. Cases were confirmed by PCR, cultured, and further characterized using ribotyping and E-test. We used two-tailed tests for significance (p≤0.05). Results: Of 30,817 cases reported, 29,245 were adult cases [HA-CDI (73.2%), CA-CDI (26.8%)] and 1,572 were pediatric cases [HA-CDI (77.7%), CA-CDI (22.3%)]. From 2015 to 2022, HA-CDI rates decreased 19.7% (p=0.007) and 29.4% (p=0.004) in adult and pediatric populations, respectively (Figure 1). CA-CDI rates remained relatively stable in the adult population (p=0.797), while decreasing 60.7% in the pediatric population (p=0.013). Median ages of adult and pediatric patients were 70 (interquartile range (IQR), 58–80) and seven (IQR, 3–13) years, respectively. Thirty-day all-cause mortality was significantly higher among adult vs. Pediatric CDI patients (11.0% vs 1.4%, p < 0.0001). No significant differences in other severe outcomes were found. Ribotyping and susceptibility data were available for 4,620 samples: 3,558 adult (77.0%) and 1,062 pediatric (23.0%). The predominant adult and pediatric ribotypes (RT) were 106 (12.2/16.2%), 027 (11.4/3.2%), and 014 (8.8/8.2%). Overall, RT027 prevalence significantly decreased from 17.9% in 2015 to 3.2% in 2022 (p=0.003), while RT106 increased from 8.5% to 14.4%. Resistance rates among adult and pediatric isolates were similar for all antimicrobials tested except moxifloxacin (16.2% vs. 6.2%, p < 0.0001, respectively). Adult moxifloxacin resistance decreased from 30% to 6.3% from 2015 to 2022 (p=0.006). Adults with moxifloxacin-resistant CDI were older (median: 74 vs. 69 years, p < 0.001) and had higher thirty-day all-cause mortality (13% vs. 9.8%, p=0.041) and recurrence (10% vs. 5.7%, p < 0.001) compared to those with moxifloxacin non-resistant CDI, while these trends were not observed in pediatric patients. Among RT027 strains, moxifloxacin resistance decreased from 91.0% in 2015 to 7.1% in 2022. There was one metronidazole-resistant pediatric sample in 2018 and no resistance to vancomycin or tigecycline in either population. Conclusion: We have found differences in the epidemiological and molecular characteristics of adult and pediatric CDI, with higher thirty-day all-cause mortality among adults. Overall, RT106 has replaced RT027 as the predominant ribotype with a concomitant decrease in fluoroquinolone resistance.

Viral Kinetics of SARS-CoV-2 in Nursing Home Residents and Staff
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s73-s74
-
- Article
-
- You have access
- Open access
- Export citation
-
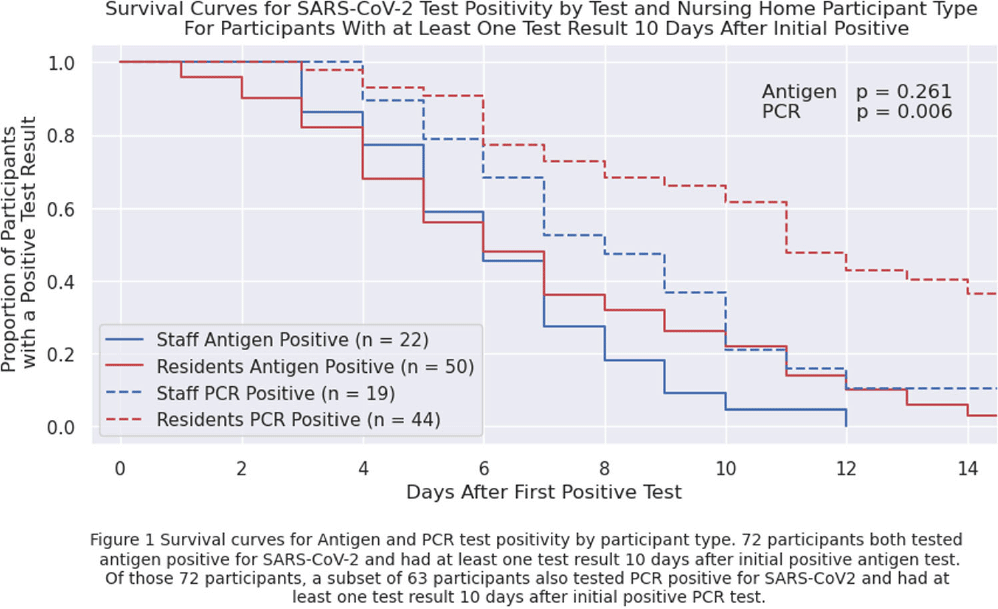
Background: Nursing home (NH) residents are at high risk of COVID-19 from exposure to infected staff and other residents. Understanding SARS-CoV-2 viral RNA kinetics in residents and staff can guide testing, isolation, and return to work recommendations. We sought to determine the duration of antigen test and polymerase chain reaction (PCR) positivity in a cohort of NH residents and staff. Methods: We prospectively collected data on SARS-CoV-2 viral kinetics from April 2023 through November 2023. Staff and residents could enroll prospectively or upon a positive test (identified through routine clinical testing, screening, or outbreak response testing). Participating facilities performed routine clinical testing; asymptomatic testing of contacts was performed within 48 hours if an outbreak or known exposure occurred and upon (re-) admission. Enrolled participants who tested positive for SARS-CoV-2 were re-tested daily for 14 days with both nasal antigen and nasal PCR tests. All PCR tests were run by a central lab with the same assay. We conducted a Kaplan-Meier survival analysis on time to first negative test restricted to participants who initially tested positive (day zero) and had at least one test ≥10 days after initially testing positive with the same test type; a participant could contribute to both antigen and PCR survival curves. We compared survival curves for staff and residents using the log-rank test. Results: Twenty-four nursing homes in eight states participated; 587 participants (275 residents, 312 staff) enrolled in the evaluation, participants were only tested through routine clinical or outbreak response testing. Seventy-two participants tested positive for antigen; of these, 63 tested PCR-positive. Residents were antigen- and PCR-positive longer than staff (Figure 1), but this finding is only statistically significant (p=0.006) for duration of PCR positivity. Five days after the first positive test, 56% of 50 residents and 59% of 22 staff remained antigen-positive; 91% of 44 residents and 79% of 19 staff were PCR-positive. Ten days after the first positive test, 22% of 50 residents and 5% of 22 staff remained antigen-positive; 61% of 44 residents and 21% of 19 staff remained PCR-positive. Conclusions: Most NH residents and staff with SARS-CoV-2 remained antigen- or PCR-positive 5 days after the initial positive test; however, differences between staff and resident test positivity were noted at 10 days. These data can inform recommendations for testing, duration of NH resident isolation, and return to work guidance for staff. Additional viral culture data may strengthen these conclusions.
Disclosure: Stefan Gravenstein: Received consulting and speaker fees from most vaccine manufacturers (Sanofi, Seqirus, Moderna, Merck, Janssen, Pfizer, Novavax, GSK, and have or expect to receive grant funding from several (Sanofi, Seqirus, Moderna, Pfizer, GSK). Lona Mody: NIH, VA, CDC, Kahn Foundation; Honoraria: UpToDate; Contracted Research: Nano-Vibronix

The Impact of Tele-Stewardship on Rural Antibiotic Prescribing Practices
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s57-s58
-
- Article
-
- You have access
- Open access
- Export citation
-
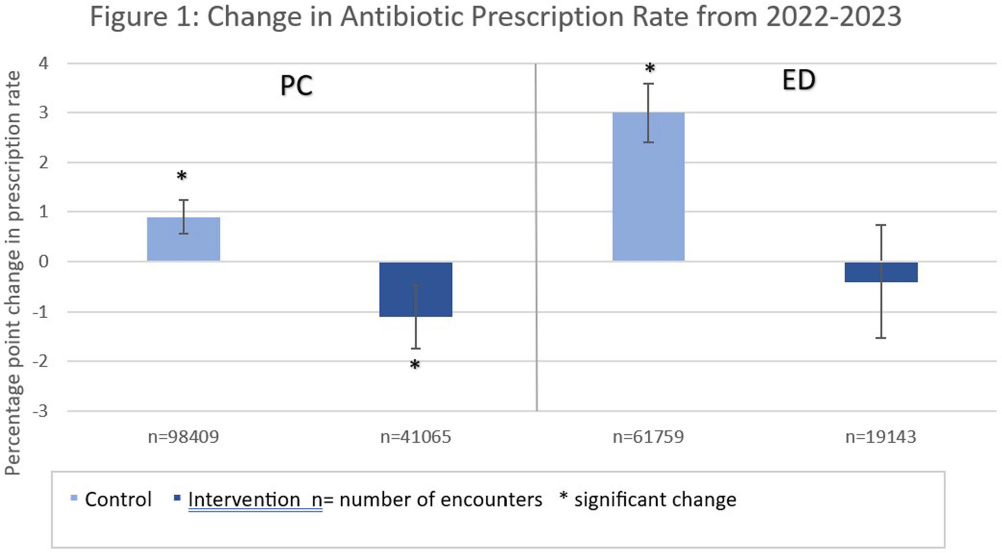
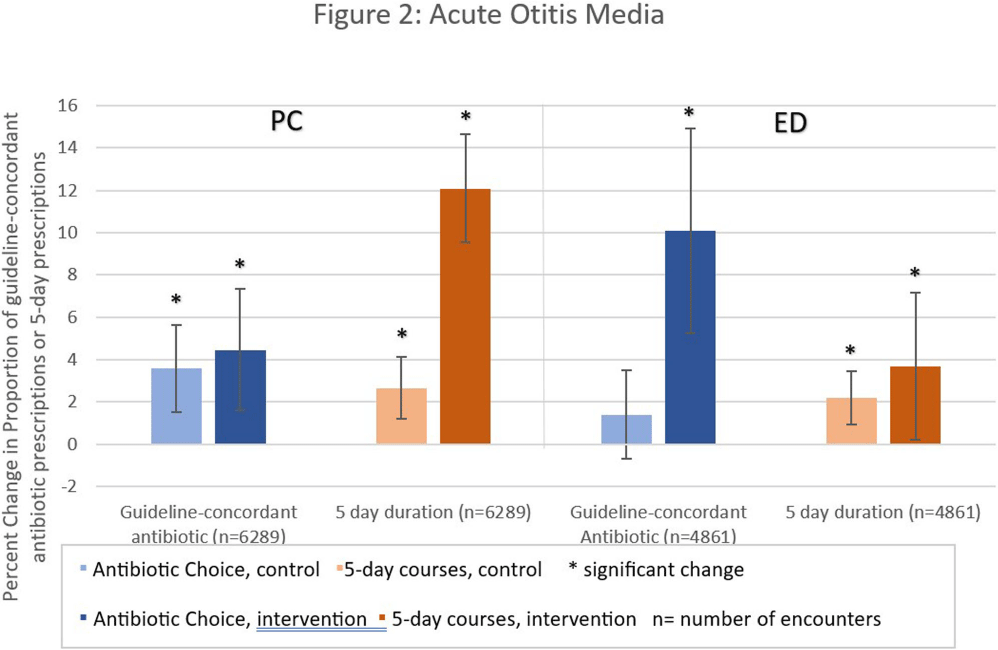
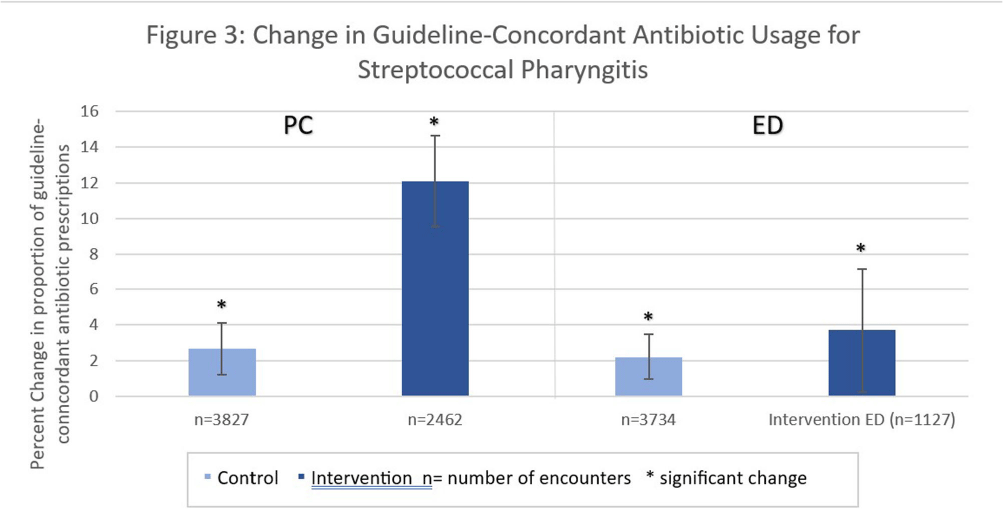
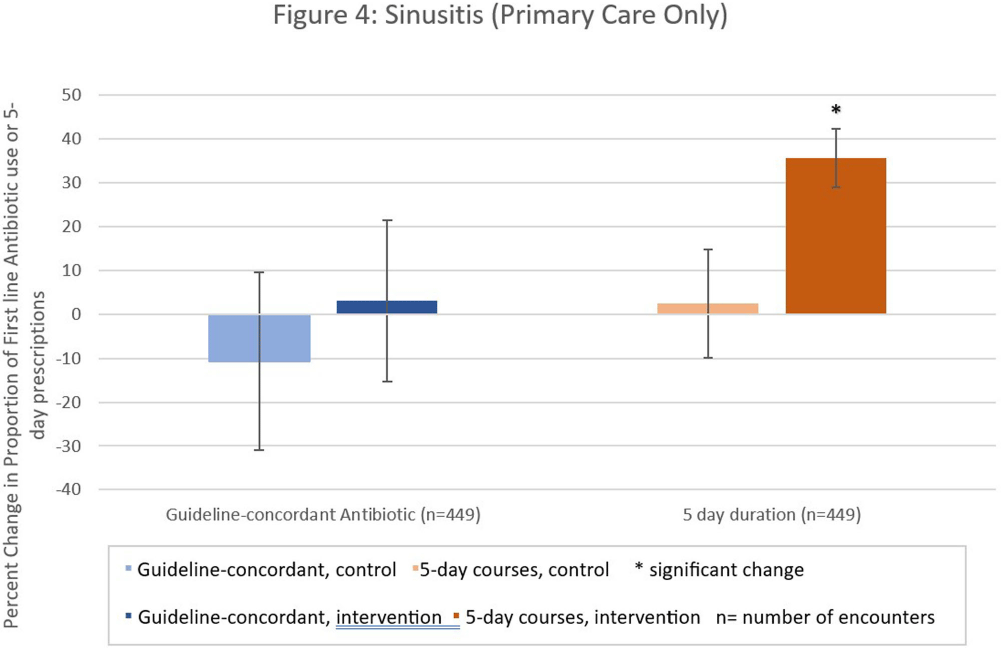
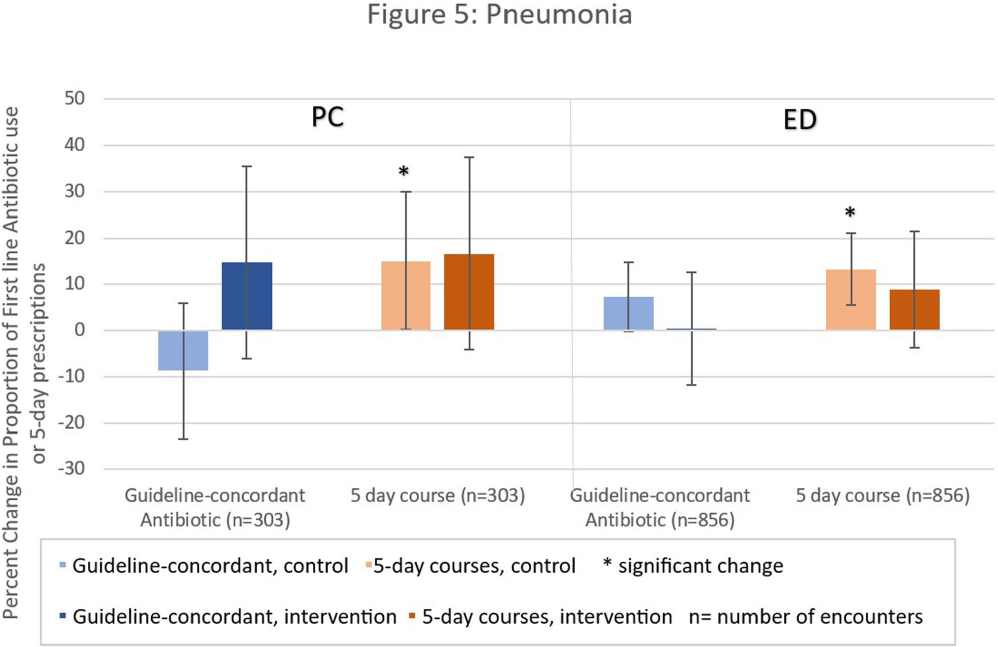
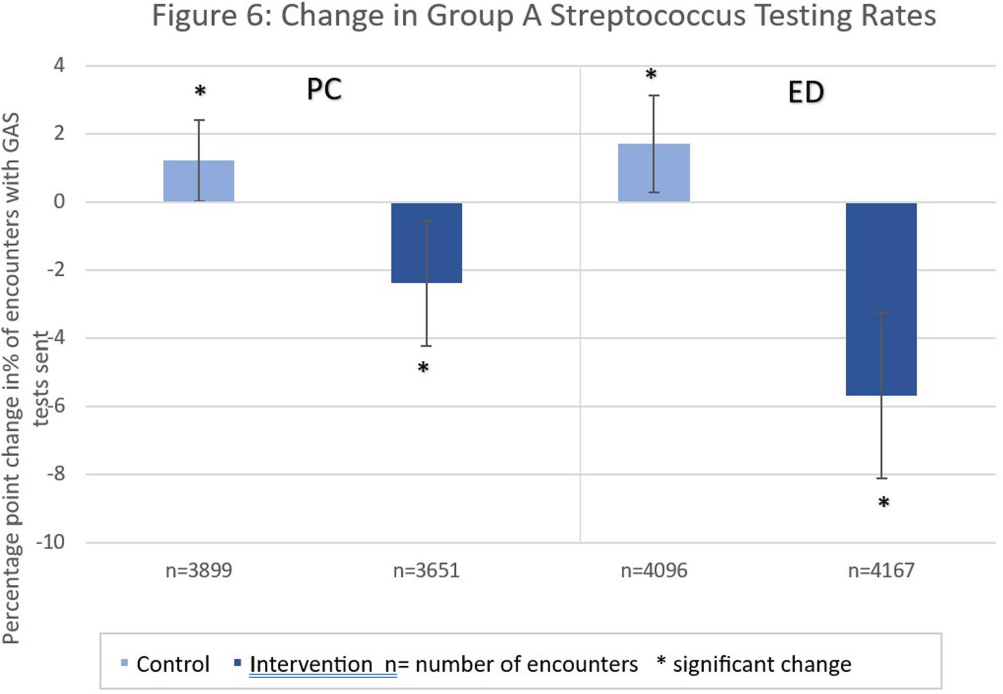
Background: Antibiotic prescribing for children is highest in rural areas. Tele-stewardship allows for implementation of antimicrobial stewardship (AS) via telecommunication with providers. This study addresses need for better AS in rural areas by implementing and evaluating bundled outpatient AS interventions using tele-stewardship in rural pediatric primary care (PC) clinics and emergency departments (EDs) affiliated with Vanderbilt University Medical Center. Methods: The bundle includes (1) patient/guardian educational materials, (2) antibiotic use commitment posters (3) provider education through quarterly teaching pearls and app-based microlearning modules (QuizTime), and (4) quarterly audit/feedback with peer comparison on guideline-concordant antibiotic use via tele-meeting and email. Participants are pediatric prescribers (physician, physician assistant, nurse practitioner). We compared antibiotic prescription data for children < 1 8 years collected during the baseline period (Jan–Dec 2022) to the intervention period (Jan-Sept 2023). Two academic PC clinics and one ED where interventions were not implemented were included as “controls”. The primary outcome is percent of encounters that result in an antibiotic prescription. Secondary outcomes include (1) percent of encounters with guideline-concordant antibiotic choice for otitis media (AOM), streptococcal pharyngitis (GAS), sinusitis, and community-acquired pneumonia (CAP); (2) percent of encounters with 5-day antibiotic duration for AOM, sinusitis, and CAP; and (3) percent of encounters with rapid GAS testing. ED sinusitis data not analyzed due to small N. Significance was determined by calculating 95% confidence intervals for the difference of proportions. Results: There were 139,474 PC encounters (91,706 baseline and 47,768 intervention) and 94,205 ED encounters (54,138 baseline and 40,067 intervention) among 20 PC prescribers and 38 ED prescribers from January 2022-September 2023. Compared to baseline, the antibiotic prescription rate decreased 1.1% in intervention PCs but increased 0.9% in control PCs (Figure 1). Compared to baseline, the antibiotic prescription rate decreased by 0.4% in the intervention EDs but increased 3.1% in the control ED (Figure 1). Secondary outcomes showed significantly increased proportions of guideline concordant ED AOM prescriptions, 5-day PC AOM prescriptions (Figure 2), guideline concordant ED streptococcal pharyngitis prescriptions (Figure 3), and guideline concordant PC sinusitis prescriptions (Figure 4). There was a decrease in GAS tests in intervention PCs and EDs (Figure 6). Conclusions: Interim analysis shows bundled implementation strategies using tele-AS led to significantly decreased overall antibiotic use in rural PC clinics compared to control sites. The study is ongoing and will continue to evaluate outcomes over a longer intervention period to reduce seasonal bias.
Disclosure: Sophie Katz: Research Grant - Pfizer; Research Grant - Dolly Parton Pediatric Infectious Diseases Research Fund; Consultant - Optum






Utility of hybrid whole genome sequencing in assessing potential nosocomial VIM transmission
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 05 August 2024, e106
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A.6 INDIGO: a global, randomized, double-blinded, Phase 3 study of vorasidenib versus placebo in patients with grade 2 glioma with an IDH1/2 mutation (mIDH1/2)
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 51 / Issue s1 / June 2024
- Published online by Cambridge University Press:
- 24 May 2024, p. S4
-
- Article
-
- You have access
- Export citation
Impact of mandatory indications for outpatient antibiotic orders on accurate tracking of antibiotic indications
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 13 May 2024, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cultivating Wellbeing: Traditional Wisdom and Sustainability in Fiji’s Green Schools
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE1 / April 2024
- Published online by Cambridge University Press:
- 07 May 2024, E7
-
- Article
-
- You have access
- Export citation
Lockean Liberalism in International Relations
-
- Published online:
- 13 March 2024
- Print publication:
- 04 April 2024
-
- Element
- Export citation
Provider-ordered viral testing and antibiotic administration practices among children with acute respiratory infections across healthcare settings in Nashville, Tennessee
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 06 March 2024, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of a mentor training curriculum to support LGBTQIA+ health professionals
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 15 February 2024, e44
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Impact of the Size of Bribes on Criminal Sanctions: An Integrated Philosophical and Economic Analysis
-
- Journal:
- Canadian Journal of Law & Jurisprudence / Volume 37 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 17 April 2024, pp. 31-46
- Print publication:
- February 2024
-
- Article
- Export citation
Chapter 2 - Point-of-Care Ultrasound for Obstetrics: Basics and Introductory Chapter
-
-
- Book:
- Obstetric Anesthesia and Uncommon Disorders
- Published online:
- 26 January 2024
- Print publication:
- 01 February 2024, pp 6-13
-
- Chapter
- Export citation
On the scaling and critical layer in a turbulent boundary layer over a compliant surface
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, R2
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of oral vancomycin treatment duration on rate of Clostridioides difficile recurrence in patients requiring concurrent systemic antibiotics
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 717-725
- Print publication:
- June 2024
-
- Article
- Export citation
Influence of Cations on Aggregation Rates in Mg-Montmorillonite
-
- Journal:
- Clays and Clay Minerals / Volume 61 / Issue 1 / February 2013
- Published online by Cambridge University Press:
- 01 January 2024, pp. 1-10
-
- Article
- Export citation
Bacteria-clay interaction: Structural changes in smectite induced during biofilm formation
-
- Journal:
- Clays and Clay Minerals / Volume 57 / Issue 2 / April 2009
- Published online by Cambridge University Press:
- 01 January 2024, pp. 205-212
-
- Article
- Export citation
Granular dilatancy and non-local fluidity of partially molten rock
-
- Journal:
- Journal of Fluid Mechanics / Volume 978 / 10 January 2024
- Published online by Cambridge University Press:
- 27 December 2023, A7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
14 Changes in Service Delivery Models for Children with Neurodevelopmental Disorders During the Covid-19 Pandemic
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 623-624
-
- Article
-
- You have access
- Export citation
90 School-based Implementation of Educational and Neurocognitive Interventions in Children with Neurodevelopmental Disorders.
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 190-191
-
- Article
-
- You have access
- Export citation
