


An 85-year-old man with a history of hypertension, hyperlipidemia, and chronic inflammatory demyelinating polyneuropathy presented with multiple episodes of transient expressive aphasia. He had no residual neurologic deficits between episodes, and magnetic resonance imaging did not demonstrate any restricted diffusion; therefore, these were diagnosed as left hemispheric transient ischemic attacks (TIAs). A cranial CT showed no infarcts and the CT angiogram showed a diminutive caliber of the extracranial and intracranial segments of the left internal carotid artery (ICA) likely due to severe atherosclerotic plaque (Figure 1). Based on CTA criteria, the left cervical ICA beyond the carotid bifurcation was reported as a near occlusion. He was initiated on dual antiplatelet therapy and referred to the Interventional Neuroradiology Clinic for urgent carotid artery stenting (CAS).
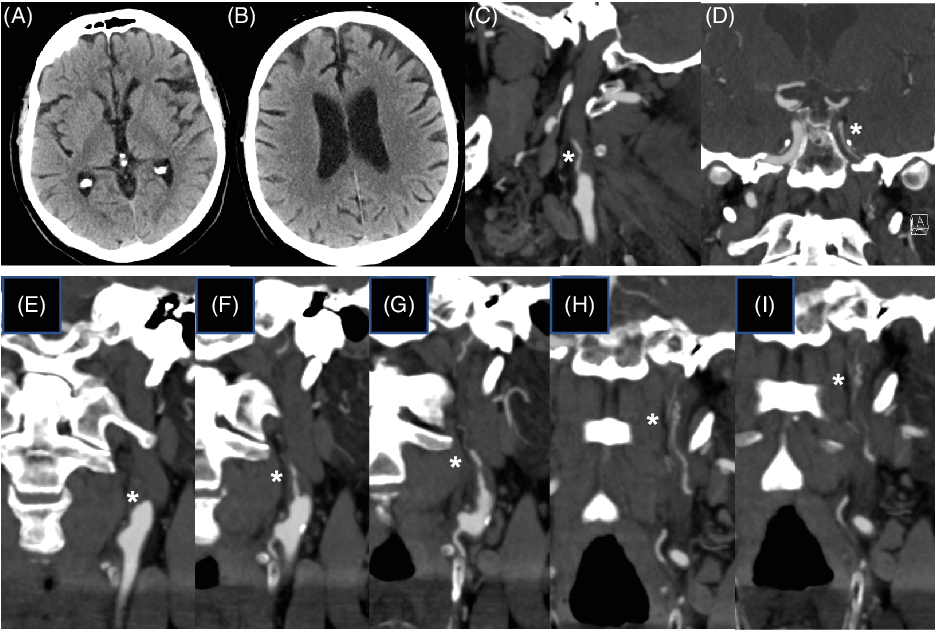
Figure 1. Cranial CT/CTA in a patient with recurrent left hemispheric transient ischemic attacks. (A and B) Non-contrast cranial CT axial images showing no obvious ischemic infarcts. (C and D) CTA showing a diminished caliber of the left cervical ICA extending into the intracranial cavernous ICA. Note: * symbol on the sagittal view (C) and coronal view (D) denotes the severe ICA stenosis. (E–I) CTA sequential coronal views demonstrating the abnormal segment of vessel (*) beyond the occluded ICA.
Diagnostic cerebral angiography demonstrated no opacification of the left ICA lumen (Figure 2). We identified a serpiginous vessel arising from the wall of the cervical ICA distal to the carotid bifurcation, consistent with dilated vasa vasorum. Intracranial views demonstrated faint opacification in the intracranial segments of the left ICA with robust collaterals from the posterior cerebral circulation via a patent left posterior communicating artery. We did not proceed to perform CAS, given this finding. He was discharged home on dual antiplatelet therapy, and months later he suffered another TIA with similar semiology. The patient was then referred to vascular surgery for surgical occlusion of the dilated vasa vasorum. Following successful surgical ligation of the vasa vasorum, he has not had any further cerebrovascular ischemic events.
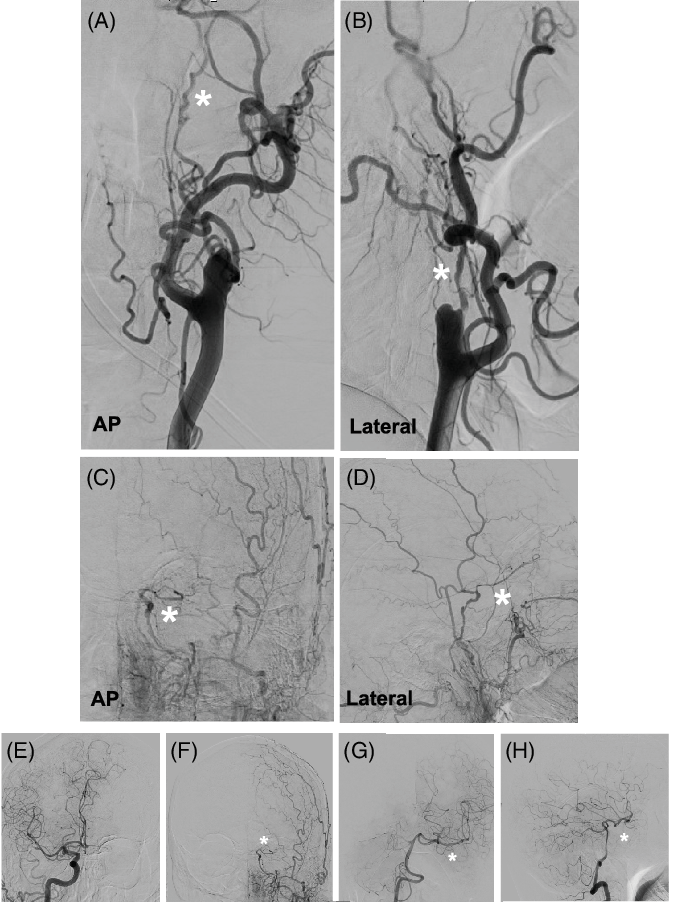
Figure 2. Digital subtraction angiography after selective injection of the left common carotid artery demonstrates an abnormal vessel arising from the anteriomedial wall of the left ICA beyond the occlusion. (A and B): Anteroposterior (AP) (A) and lateral views (B) of the cervical carotid showing the ICA stump distal to the carotid bifurcation with the hypertrophied vasa vasorum arising for the anteromedial artery wall (asterisks *). (C and D): AP (C) and lateral (D) views demonstrate the intracranial course of the dilated vasa vasorum that continues to course intracranially to the level of the ophthalmic segment of the left ICA (*). (E–H): Robust collaterals from the posterior cerebral circulation via the left posterior communicatingartery. Note: E: selective right CCA injection; F: selective left CCA injection, G and F: selective right vertebral artery injection.
Vasa vasorum consists of microvessels located in the adventitia of arteries and supplies the artery with nutrients not received through diffusion from the lumen. Reference Portanova, Hakakian and Mikulis1 Growth of the vasa vasorum can be induced by factors such as increased oxygen demands, thickening of the vessel wall, and angiogenic growth factors. Reference Mulligan-Kehoe and Simons2 Proliferation of the vasa vasorum has been identified in the region of atherosclerotic carotid plaque on both ultrasound and magnetic resonance imaging. Reference Magnoni, Coli and Massimilian3,Reference Kerwin, Oikawa, Yuan, Jarvik and Hatsukami4 A prominent vasa vasorum of the extracranial ICA has also been noted after complete ICA occlusion due to atherosclerosis or dissection. Reference Kemeny, Droste and Nabavi5,Reference Colon, Deveikis and Dickinson6 In this patient, the CTA initially raised the possibility of a left ICA near occlusion; however, the cerebral angiogram demonstrated no filling of the left ICA lumen and instead a hypertrophied vasa vasorum. It is important to distinguish between hypertrophied vasa vasorum and the well-described carotid string sign, where there is collapse of the post-stenotic cervical ICA down to a “string.” Other authors also note that dilated vasa vasorum is more serpiginous than the classic string sign and may also be formed by multiple channels. Reference Martin and Marotta7 We propose calling this finding a carotid corkscrew sign, to distinguish it as a separate pathologic entity. Recognizing the dilated vasa vasorum on cerebral angiography allowed for appropriate avoidance of CAS and referral for surgical occlusion.
Conflicts of Interest
None of the authors have any conflicts of interest or disclosures.


