



Deprived nutritional status is one of the major health and well-being problems in Bangladesh( 1 ). This situation comprises three basic components of insufficiency: being too short for one’s age (stunting), being underweight for one’s age and being dangerously thin (wasting)( 2 ). Undernutrition, however, includes consumption of an inadequate amount of food which is unable to meet the body’s requirements for growth, maintenance and specific functions( Reference de Onis, Monteiro and Akré 3 , Reference Martins, Toledo Florêncio and Grillo 4 ). It is recognized that the first 1000 d are the most crucial period for the brain development and linear growth of a child, which prevents early stunting and underweight( Reference de Onis, Dewey and Borghi 5 ). It is also globally accepted that undernutrition has both short- and long-term consequences( Reference Black, Victora and Walker 6 ). Therefore childhood undernutrition glitches present significant concerns for survival, health development and social economic productivity( Reference Black, Victora and Walker 6 ). Globally, 3·5 million deaths occur per year due to maternal and child undernutrition, while approximately half of all deaths in children under 5 years of age (under-5s) are attributable to undernutrition( Reference Black, Allen and Bhutta 7 , 8 ). This explains that there is preventable loss of many young lives per day. These losses occur widely in low- and middle-income countries, while 80 % of the undernourished children globally live in just twenty countries including Bangladesh( Reference Bryce, Coitinho and Darnton-Hill 9 ).
Worldwide, 22·9 % of under-5s are stunted, 14·0 % are underweight and 7·7 % are wasted( 8 , 10 , 11 ). In South Asia, the prevalence of the three components is quite high at 35·8, 29·8 and 16·0 %, respectively( 10 , 11 ). In Bangladesh, however, 36·1 % of under-5s are stunted, 32·6 % are underweight and 14·3 % are wasted( 1 ). The prevalence of stunting has decreased by only 1·5 percentage points per year (from 51 to 36) between 2004 and 2014 in Bangladesh( 1 ). Besides, the prevalence of underweight has decreased by 1 percentage point per year (from 43 to 33) over the same period, while the prevalence of wasting has remained almost constant. In summary, the annual average reduction in stunting and underweight was just 2·9 and 2·3 %, respectively. Thus, the target of a 40 % reduction in stunting and keeping wasting below 5 % by 2025 set by the World Health Assembly (WHA)( 12 – Reference Ahmed, Hossain and Mahfuz 14 ) becomes immensely challenging. In addition, Bangladesh has shown insufficient progress in the Millennium Development Goal 1 (MDG1) target of reducing underweight( 15 ). Therefore, Bangladesh is less likely to achieve the WHA and MDG1 targets on reducing childhood undernutrition with the current pace of reduction( 1 , Reference Ahmed, Hossain and Mahfuz 14 ).
The mother is generally the principal caregiver in Bangladesh while the father is the predominant decision maker( Reference Naved 16 ). Hence, a more educated mother and father might apparently provide better protection of their child against childhood undernutrition( Reference Semba, de Pee and Sun 17 ). A few studies( Reference Vollmer, Bommer and Krishna 18 – Reference Gupta, Mehrotra and Arora 20 ) have been done previously to assess the relationship between childhood undernutrition and parental education. In the context of Bangladesh, Semba et al.( Reference Semba, de Pee and Sun 17 ) found that a higher level of parental education was related to a lower prevalence of childhood stunting. A recent study( Reference Hasan, Soares Magalhaes and Williams 21 ) found a significant association between childhood undernutrition and maternal education. A most recent study( Reference Musa, Muhammad and Lawal 22 ), on the other hand, found that a higher level of paternal education was significantly associated with a lower level of children’s severe acute malnutrition.
Recently, a study( Reference Sarma, Khan and Asaduzzaman 23 ) found that children from the richest, food secure and improved toilet facilities households had significantly lower odds of being stunted in Bangladesh. These authors also showed that parental education significantly reduces the chance of childhood stunting. Another study( Reference Nahar, Ahmed and Brown 24 ) showed that there is less chance of childhood undernutrition when the father has decent job opportunities, the mother is normal weight, and both father and mother are well educated. Chowdhury et al.( Reference Chowdhury, Rahman and Khan 25 ) identified the risk factors of child malnutrition in Bangladesh. These authors found that factors such as maternal BMI, education, paternal education, place of residence, socio-economic status, community status, religion, region of residence and food security are significantly associated with childhood malnutrition in Bangladesh. Although many authors found that higher parental education is associated with lower prevalence of childhood undernutrition, they did not relate other factors to paternal education. Paternal education is usually related to household income since highly educated fathers earn more money and marry women of a comparable level of education( Reference Naved 16 ). Hence, higher paternal education also leads to the household being food secure, having improved toilet facilities, better nutrition status of family members and being aware of the child’s undernutrition status.
Although policy makers have undertaken a few necessary initiatives to address the lack that relates to high childhood undernutrition prevalence in Bangladesh, still the targets of reducing childhood undernutrition remain unattainable for the country( 1 , Reference Kabir 26 ). We assumed that higher level of parental education can sufficiently reduce the risk of childhood undernutrition in Bangladesh. We also expected that the combination or interaction of higher parental education can increase the pace of the reduction in undernutrition prevalence of the country. The present study addressed and signified these hypotheses by carrying out a comprehensive analysis to identify the true relationship between childhood undernutrition and parental education after adjusting the estimates for potential risk factors in the Bangladeshi context.
Methods
Study site and participants
A secondary data set from the Bangladesh Demographic and Health Survey (BDHS) 2014 was used for the present study. The 2014 BDHS was a nationally representative cross-sectional survey conducted between June and November 2014 which covered all districts and administrative divisions of Bangladesh( 1 ). The base survey was conducted by using two-stage stratified sampling of households. In first stage, 600 enumeration areas (EA) were selected with probability proportional to EA size, with 207 EA from urban areas and 393 EA from rural areas. An EA, however, is a village or a group of small villages or a part of a large village( 1 , 27 ). In the second stage, a systematic sample of thirty households on average was selected per EA to provide statistically reliable estimates of the key demographic and health variables for the country as a whole and for urban and rural areas separately. Data quality measures were implemented through several activities: regular field visits by survey teams, re-interviewing the respondents and spot-checking the completed questionnaire by quality control teams( 1 ).
The 2014 BDHS collected information from 18 000 households, of which 17 863 contained an ever-married woman. These women had a total of 7692 children under 5 years old. A total of 404 children had no information on either height or weight, and 115 children had implausible height or weight measurements. The implausibility was defined based on WHO (2006) standards flag limits of Z-score: for stunting, <−6 or >6; for wasting, <−5 or >5; and for underweight, <−6 or >5( 1 , 27 ). Finally, 7173 children were selected for the present study (Fig. 1). These 7173 children were from 6415 households, where 5687 households (79·3 %) each had a single under-5 child, 698 households (19·5 %) each had two under-5 children and thirty households (1·2 %) each had three under-5 five children.
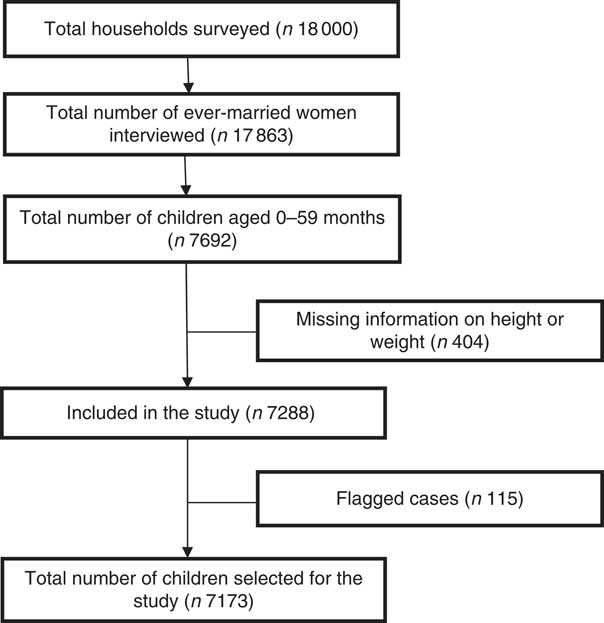
Fig. 1 Flowchart showing the selection of children for the present study from the Bangladesh Demographic Health and Survey (BDHS) 2014 secondary data set
Variables assessed/measured
There were three types of questionnaire in BDHS 2014: household, woman and community. The contents of the household and woman’s questionnaires were based on the MEASURE DHS Model Questionnaires. The purpose of the household questionnaire was to list all the usual members and visitors in the selected household. Basic information was then collected on a few selected characteristics such as age, sex, education and current working status. The main purpose of the woman’s questionnaire was to identify women who were eligible for the individual interview. Women were asked questions on several topics and background characteristics including age, education, religion, work, reproductive history, family planning, fertility preference, husband’s background and child’s background. The woman’s questionnaire was also used to record the height and weight measurements of ever-married women aged 15–49 years and their under-5 children. Detailed information on the assessed and measured variables can be found in the BDHS 2014 report( 1 ).
Outcome measurements
The three basic outcomes variables to define childhood undernutrition are stunting, underweight and wasting( 1 , Reference Vollmer, Bommer and Krishna 18 ).
1. Stunting: A child more than two standard deviations below the median (<−2 sd) of the WHO reference population in terms of height-for-age was considered stunted( 1 , 27 ).
2. Underweight: A child more than two standard deviations below the median (<−2 sd) of the WHO reference population in terms of weight-for-age was considered underweight( 1 , 27 ).
3. Wasting: A child more than two standard deviations below the median (<−2 sd) of the WHO reference population in terms of weight-for-height was considered wasted( 1 , 27 ).
Statistical analysis
Descriptive analysis was performed to assess the distribution of the variables using appropriate cut-offs. The χ 2 test was used for comparing the prevalence of undernutrition among different determinants with 5 % level of significance. To ensure actual representation of nationwide data, sampling weights were used to estimate prevalence. A brief calculation and explanation of sampling weights can be found in the BDHS 2014 report( 1 ). It was not required to use sampling weights while assessing relationships such as regression and correlation coefficients( 1 ), and hence we did not consider weighting when running the regression models. Since the data were nested in nature and there was cluster-to-cluster variation, we considered modified Poisson regression models to truly estimate the association between parental education and childhood undernutrition( Reference Zou and Donner 28 ). In this case, we considered parental education (and other potential confounders) as a fixed effect and cluster variation as a random effect. Parameters of the models were estimated through the generalized estimating equation approach by considering exchangeable correlation structure between clusters. Basically, the initial goal was to run binomial models to establish the relationship. Since the binomial models had a convergence problem with many covariates, modified Poisson regression models were implemented. It is worth mentioning that the modified Poisson regression model is equivalent to the binomial model( Reference Zou and Donner 28 , Reference Zou 29 ). The risk ratio (RR), the exponentiated β coefficient of a modified Poisson model, was used to assess the association between undernutrition and parental education while controlling for confounding variables. The RR and corresponding 95 % CI were estimated by considering the 5 % level of significance, keeping in mind that the OR overestimates the relative risk in the case of prevalence ≥10 %( Reference Wilber and Fu 30 – Reference Cummings 32 ). All analyses were performed using the statistical software package Stata version 13.0.
Results
Sample description
Among the 7173 under-5 study children, more than one-third were from Dhaka division (Table 1). A total of 74·8 % children lived in rural areas and 41·5 % were from poor households (22·7 % poorest, 18·8 % poorer). The ratio of males to females was almost unity while 41·1 % of the children were below 2 years of age. In addition, 61·5 % of children had a mother aged 20–29 years and 46·9 % had a father aged 25–34 years. More than 16 % of children’s mothers had no schooling, while 15·5 % had completed grade 10 or more. Besides, 26·2 % of children’s fathers had no schooling and 20·1 % had completed grade 10 or more. Moreover, 73·8 % of mothers were housewives, while 28·3 % of fathers were servicemen or businessmen and 22·9 % were agricultural workers. A total of 22·0 % of mothers were underweight (BMI<18·5 kg/m2), 59·8 % were normal weight (BMI=18·5–24·9 kg/m2), 15·3 % were overweight (BMI=25·0–29·9 kg/m2) and only 3·0 % were obese (BMI≥30·0 kg/m2; Table 1).
Table 1 Descriptive statistics of Bangladeshi children under 5 years old (n 7173) and their parents, Bangladesh Demographic Health and Survey (BDHS) 2014
* Primary incomplete=grade 1–4.
† Primary or secondary incomplete=grade 5–9.
‡ Secondary or higher=grade 10 or higher.
§ Non-agricultural worker=fisherman, home-based manufacturing, factory worker, carpenter, bus/taxi driver, tailor.
║ Others=rickshaw driver, construction worker, domestic servant, student, unemployed.
Prevalence of childhood undernutrition
The prevalence of childhood undernutrition was found from the study of 2014 BDHS data. Overall, 36·2 % of the under-5 children were stunted, 32·6 % were underweight and 14·4 % were wasted (Fig. 2). Also, 48·2 % of children were suffering any form of undernutrition while 5·4 % were suffering all forms of undernutrition.
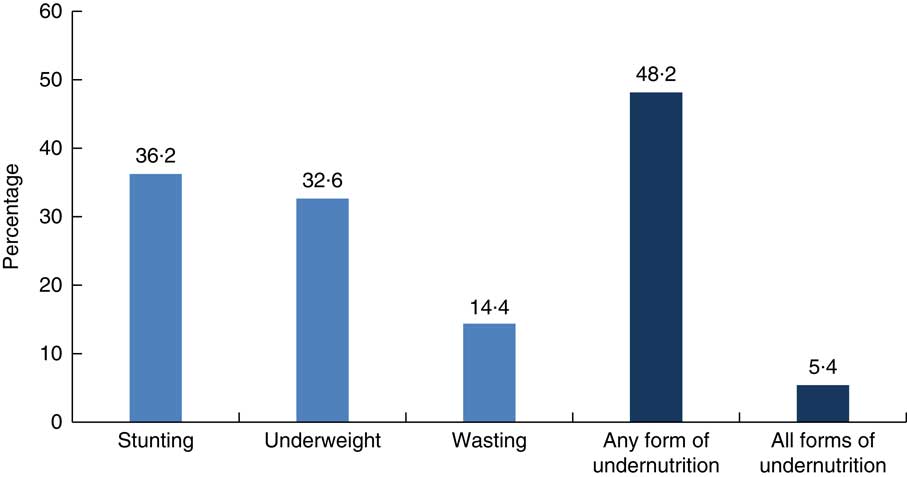
Fig. 2 Prevalence of childhood undernutrition among Bangladeshi children under 5 years of age (n 7173), Bangladesh Demographic Health and Survey (BDHS) 2014
Stunting was higher in Sylhet division (49·9 %) and lower in Khulna (27·9 %; P<0·001; Table 2). Children from rural areas and poor households were more prone to being stunted (rural, 38·1 %; poorest, 49·4 %; poorer, 42·3 %; both P<0·001). As expected, stunting increased with increasing age, except for a decrease from the fourth birthday of the child (P<0·001). There was no significant difference in stunting prevalence between boys and girls, while children of higher birth order experienced higher prevalence (31·7 % for the first child, 35·8 % for the second child and 42·2 % for the third or later child; P<0·001). Besides, stunting increased as maternal age increased although not significantly. But when maternal level of education increased, the prevalence of childhood stunting reduced (P<0·001). Children of mothers who had no schooling experienced 47·5 % prevalence of childhood stunting, whereas the prevalence was 35·5 and 18·4 % among children whose mothers completed grade 5–9 and grade 10 or more, respectively (P<0·001). The prevalence of childhood stunting was significantly lower for children whose mothers worked outside the home than for those whose mothers who were housewives (34·4 and 41·6 %, respectively; P<0·001). Moreover, childhood stunting decreased as maternal BMI increased (P<0·001). Although paternal age was not associated with childhood stunting, paternal education and occupation showed significant associations (both P<0·001). Among fathers who had no schooling, 48·4 % had a stunted child. The prevalence was 34·1 and 20·0 %, respectively, for those children whose father had completed grade 5–9 and grade 10 or more. Besides, children whose father was a serviceman or businessman were significantly less experienced with childhood stunting (29·0 %; P<0·001).
Table 2 Bivariate analysis of household, child and parental characteristics associated with childhood undernutrition in Bangladeshi children under 5 years old (n 7173), Bangladesh Demographic Health and Survey (BDHS) 2014
Similar results were found for childhood underweight. The prevalence of underweight was highest in Sylhet division (40·0 %) and lowest in Khulna (25·6 %; P<0·001). Children from rural areas and poor households were more prone to being underweight (rural, 34·8 %; poorest, 45·5 %; poorer, 38·6 %; both P<0·001). Also, the prevalence increased as child age increased (P<0·001). A similar pattern was also observed for child’s birth order (P=0·001). Nevertheless, there was no significant difference in the prevalence of underweight between boys and girls. In addition, underweight prevalence decreased as mother’s level of education increased (no schooling, 41·9 %; grade 5–9, 32·4 %; grade 10 or more, 17·8 %; P<0·001). Children whose mother was a housewife were less prone to underweight (30·5 %) and the prevalence decreased as maternal BMI increased (P<0·001). Similar to stunting, the prevalence of underweight was the lowest among children from serviceman/businessman fathers and fathers who had completed higher level of education (both P<0·001).
On the other hand, wasting was high in Barisal division (17·7 %), in rural areas (15·1 %) and in poor households (poorest, 17·1 %; poorer, 16·7 %; all P<0·001). Wasting was highest among children aged 0–5 months (19·9 %) and lowest among children aged 36–47 months (11·6 %; P=0·004). However, wasting was merely associated with parental characteristics. Rather than parental age, education and occupation, it was associated only with maternal BMI (P<0·001). Combined estimates of the prevalence of the composite outcome variable, undernutrition, are also shown in Table 2.
Association between parental education and childhood undernutrition
Both maternal and paternal education were highly associated with childhood undernutrition (Table 3). Higher level of parental education was associated with lower levels of stunting and underweight, but not associated with wasting. In models without any adjustment (crude), the risk of childhood stunting and underweight decreased gradually with the increase of maternal and paternal education. When considering grade 10 or more, maternal education was a stronger predictor than paternal education. In contrast, when considering grade 5–9, paternal education, instead of maternal education, showed a greater contribution to the reduction of child stunting or underweight than maternal education. These differences were also seen in the model with child’s age and sex adjusted for (Model 1); were strongly attenuated when further adjusted for maternal age, occupation and BMI, and paternal occupation (Model 2); and even more so when further adjusting for administrative division, place of residence and household wealth quintile (Model 3).
Table 3 Relationship of maternal and paternal education with childhood undernutrition in Bangladeshi children under 5 years old (n 7173), Bangladesh Demographic Health and Survey (BDHS) 2014
RR, relative risk; Ref., reference category.
Model 1 adjusted for child’s age and sex. Model 2 adjusted for child’s age and sex, maternal age, occupation and BMI, and paternal occupation. Model 3 additionally adjusted for administrative division, place of residence and household wealth quintile.
From the fully adjusted model (Model 3), it can be seen that there was 31 % reduction in child stunting when the mother had completed grade 10 or more (RR=0·69, 95 % CI 0·59, 0·81) while it was a 27 % reduction when the father had completed grade 10 or more (RR=0·73, 95 % CI 0·64, 0·84). Similarly, there was a 25 % reduction in child underweight when the mother had completed grade 10 or more (RR=0·75, 95 % CI 0·63, 0·89) while it was a 17 % reduction when the father had completed grade 10 or more (RR=0·83, 95 % CI 0·71, 0·95). In contrast, there was no significant reduction in either child stunting or child underweight when the mother had completed grade 5–9. On the other hand, when the father had completed grade 5–9, the risk of child stunting was 16 % less (RR=0·84, 95 % CI 0·78, 0·92) and the risk of child underweight was 12 % less (RR=0·88, 95 % CI 0·80, 0·96). Notably, parental education to grade 1–4 had no significant effect on reduction of child stunting or child underweight, while wasting was not associated with any level of parental education. Overall, there was 22 % less risk of any form of child undernutrition when the mother had completed grade 10 or more (RR=0·78, 95 % CI 0·69, 0·88), while it was 12 % less when the father had completed grade 10 or more (RR=0·88, 95 % CI 0·80, 0·97). Moreover, there was an 11 % less risk of any form of child undernutrition when father had completed grade 5–9, while maternal 5–9 grade education remained insignificant to reduce the risk of child stunting and underweight.
We further analysed the data to estimate the combined or interaction effect of parental education on childhood undernutrition, and hence run the model with an interaction between maternal and paternal education. Since the main effect on wasting was not associated with parental education, we run the interaction model only for stunting and underweight. The result of the fully adjusted model is shown in Table 4. From Table 4 it is evident that the combined higher level of parental education was significantly associated with low risk of childhood stunting and underweight. When both parents had completed grade 10 or more, there was 47 % less risk of child stunting (RR=0·53, 95 % CI 0·44, 0·64), 33 % less risk of child underweight (RR=0·67, 95 % CI 0·56, 0·80) and 29 % less risk of any form of child undernutrition (RR=0·71, 95 % CI 0·62, 0·81). It is also evident from Table 4 that as level of education increased for both parents, there was monotonic decline of the risk of child stunting and underweight.
Table 4 Interaction effects of parental education with childhood undernutrition in Bangladeshi children under 5 years old (n 7173), Bangladesh Demographic Health and Survey (BDHS) 2014
RR, relative risk; Ref., reference category.
* RR adjusted for child’s age and sex, maternal age, occupation and BMI, paternal occupation, administrative division, place of residence and household wealth quintile.
Discussion
The present study gives a vibrant picture of parental education in relation to the reduction of under-5 children’s stunting and underweight in Bangladesh. We adjusted the final model by different factors including child’s age and sex, maternal age, occupation and BMI, paternal occupation, administrative division, place of residence and household wealth quintile. These adjusted factors were found previously as the factors significantly associated with childhood undernutrition in Bangladesh( Reference Sarma, Khan and Asaduzzaman 23 – Reference Chowdhury, Rahman and Khan 25 , Reference Talukder 33 , Reference Amin, Murimi and Carabaza 34 ). The present study found that both maternal and paternal education are very strong predictors for child undernutrition. The study also found that the higher the level of their education, the greater the reduction in the risk of child stunting and underweight. Most strikingly, the study found that reduction of child wasting was not associated with parental education.
The relationship between grade 10 or more of parental education and child undernutrition was stronger for maternal education than for paternal education when their interaction or the combined level of education was held fixed. Similar results were found by Vollmer et al.( Reference Vollmer, Bommer and Krishna 18 ) for low- and middle-income countries. One possible reason behind this might be that highly educated mothers are usually more empowered and thus they make substantial decisions on family dietary diversity and child health. In contrast, the relationship between 5–9 grade of parental education and child undernutrition was stronger for paternal education than for maternal education. A recent study( Reference Sarma, Khan and Asaduzzaman 23 ) found similar results. Semba et al.( Reference Semba, de Pee and Sun 17 ) also found that the odds of stunting were impressively decreased by increasing paternal education compared with maternal education. The possible reason behind this might be that women who have low social status and less education have very limited influence on household decision making. However, the interaction-only model gives the evidence that the reduction in childhood undernutrition is greater when both mother and father had completed grade 10 or more. Indeed, completing grade 5–9 of education by both the mother and father can reduce the risk of child undernutrition, while it is decreased further when at least one partner has completed grade 10 or more.
Administratively, children of Sylhet division had a higher prevalence of undernutrition. The eventual reason is that there were 26·4 % of women and 40·0 % of men who had no schooling, but only 8·1 % of women and 10·5 % of men who had completed grade 10 or more in this region (Table 5). In contrast, the prevalence of undernutrition was lowest in Khulna. Khulna had comparatively more women and men who had completed grade 10 or more than any other division. This also leads to a plan to educate both mothers and fathers to increase the pace of reduction in childhood undernutrition in Bangladesh.
Table 5 Division-specific percentage of parental education, Bangladesh Demographic Health and Survey (BDHS) 2014
Eventually, underweight mothers could be more likely to have underweight children who simultaneously achieve a low level of education, continuing the cycle. To empower women to make decisions on their own and their children’s health, it is mandatory to educate them( Reference Samarakoon and Parinduri 35 ). Besides, keeping girls in school longer can delay age of marriage and age at first birth and reduce the demand for childbearing, which might be a good way to empower them( Reference Alderman and Headey 19 , Reference Duflo 36 ). Although the mother is the primary caregiver for the child, the father also has a great influence on child health and education in Bangladesh. Our analysis revealed that higher level of education of both mother and father successively reduces the prevalence of childhood undernutrition. Hence, to hasten the reduction in prevalence of undernutrition in Bangladesh and to achieve the WHA target and MDG1 goal of reducing childhood undernutrition, we need to educate both mothers and fathers.
The present study has some limitations. First, it is challenging to investigate the causation from the cross-sectional design and hence only associations are truly estimable. Second, child undernutrition might be exaggerated by maternal and paternal biological factors that are not considered in the current analysis. Finally, both maternal and paternal level of education were self-reported by respondents, hence it was not possible to validate that information.
Very few public health initiatives are currently going on to reduce the prevalence of childhood undernutrition in Bangladesh. More specifically, interventions such as maternal and child health care, intensification of primary health-care facilities, and campaigns such as community and individual-level health campaign are currently being adopted by the Government of Bangladesh to hasten the reduction. Since the mother is the key caregiver for the child, and the father is the fundamental decision maker and earner in Bangladesh, without educating them it is impossible to obtain the WHA and MDG1 targets of reducing undernutrition prevalence in this country. Henceforth, government and non-government policy makers in Bangladesh should ensure formal education for all boys who are the future decision makers and earners, and for all girls who are the future mothers, to reduce significantly the prevalence of childhood undernutrition in Bangladesh. Adopting compulsory education up to secondary level for both boys and girls would be a prodigious technique to reduce the prevalence of undernutrition in Bangladesh. Special attention could be given to specific areas including Sylhet to promote education and health-care facilities. Authorities should increase and introduce quality health services, including medical services and immunization, and sanitary facilities, because malnourished children are physically weak, have less resistance to disease, do less well at school, are less productive as adults and so are vulnerable for the rest of their lives.
Acknowledgements
Acknowledgements: The authors would like to thank and acknowledge the contribution of the Bangladesh Demographic and Health Survey 2014 team for their efforts in providing open access to the data set. Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: None. Authorship: M.B.H. contributed to formulating the research question, analysing the data and drafting the manuscript. M.H.R.K. also contributed to drafting the manuscript and advising the first author in formulating the research question. Ethics of human subject participation: Not applicable.







