


Considered one of the main public health problems worldwide, obesity is a disease that affects individuals in different economic classes and age groups. Among women of reproductive age, the prevalence of obesity is approximately 25 % in Brazil, some European countries and the USA( Reference Seabra, Padilha and Queiroz 1 – Reference Victora, Bahl and Barros 4 ).
Obesity during the pre-conception period tends to persist or worsen during the pregnancy–puerperal cycle, resulting in increased obstetric risks (congenital malformation, gestational diabetes, hypertension, thromboembolism) and continuity of complications during childbirth (premature delivery, dystocia), puerperium and lactation. Regarding lactation, a growing number of publications have demonstrated greater difficulties in initiating and maintaining the practice of breast-feeding among women who are obese during the pre-gestational period( Reference Castillo, Santos and Matijasevich 5 – Reference Thulier and Mercer 8 ).
The association between low lactational performance and high pre-gestational BMI may be due to several causes. These include alterations related to the biological sphere, such as modification of the mammary anatomy; adverse clinical conditions caused by overweight that promote separation of mother and child after birth; psychological factors, such as higher rates of postpartum depression; and physiological causes, such as delayed lactogenesis II due to a lower prolactin response in the first 72 h of the puerperium period( Reference Kair and Colaizy 9 ).
Impaired lactation performance predisposes infants to a higher risk of developing both short- and long-term morbid conditions, such as intestinal infections, respiratory infections, allergies, obesity and type 2 diabetes( Reference Victora, Bahl and Barros 4 ).
On the other hand, recent studies have demonstrated a dose-dependent association between the duration of breast-feeding and decreased risk of obesity in children( Reference Portela, Vieira and Matos 10 , Reference Assunção, Ferreira and Coutinho 11 ), a problem that has become of increasing concern to society, health professionals and policy makers.
The Brazilian state of Alagoas exhibits the worst economic and social indicators in the country( Reference Moreira, Cabral and Ferreira 12 ). Its population has the lowest average income, the highest proportion of people classified below the poverty line and the lowest educational levels. In addition, the state has evolved economically at a slower rate than other Brazilian states(13). Thus, public health in Alagoas in particular could be positively affected by a wider and more effective practice of exclusive breast-feeding.
Changes in the pattern of nutritional problems have resulted in increased obesity in younger age groups. With the aim of preventing those problems through breast-feeding, the present study evaluated whether pre-gestational obesity reduces the duration of breast-feeding in a Brazilian Northeast state.
Materials and methods
The present study was a cross-sectional analysis that utilized the II Diagnosis of Health of Maternal and Child Population of Alagoas State survey, which evaluated 418 children up to 24 months of age and their respective mothers.
To compose the sample, a multiple-stage process was adopted with four stages. In the first stage, twenty municipalities were randomly selected through systematic sampling with a probability proportional to size. For this, the municipalities were organized in alphabetical order according to their respective geographic regions and population sizes. In the second stage, four census tracts were drawn in each municipality with consideration of the proportion between urban and rural sectors. In the third stage, a block was drawn within each census section. In the fourth and final stage, a starting point was drawn within each block and twenty-eight consecutive households were visited.
Inclusion and exclusion criteria
All children under 24 months of age residing in households that were randomly selected were eligible for the study.
Children and/or mothers who presented pathologies at birth that impeded breast-feeding were excluded from the study. These conditions included mothers with HIV and children with a cleft lip. This information was obtained through a questionnaire administered to the biological mother. Thus, being an adoptive mother was an exclusion criterion since breast-feeding under such circumstances is less likely to occur.
Data collection
The fieldwork was carried out between January 2014 and January 2015 by a team of trained and supervised interviewers.
The data were collected through home visits using structured questionnaires that were pre-tested in a pilot study. Data on socio-economic and demographic characteristics, access to public services, the mothers and children, and breast-feeding and infant feeding were collected.
Definition of study variables
Dependent variables
The dependent variables were exclusive breast-feeding (EBF) and breast-feeding (BF), which were defined according to the definitions proposed by the WHO( 14 ). The WHO considers children to be exclusively breast-fed if they receive only breast milk direct from the breast, expressed milk from the mother, or human milk from other sources without other liquids or solids, except for drops or syrups containing vitamins, oral rehydration salts, mineral supplements or medicinal products. The BF period refers to the maximum period during which the child receives breast milk (directly from the breast or expressed milk) regardless of whether he/she receives other foods.
The data collection instrument consisted of a direct question regarding the amount of time that the child was exclusively breast-fed. In addition, questions about the age of introduction of water, tea, milk from sources other than the mother, or any other foods were included to complement the responses regarding the duration of EBF, thus increasing the consistency of the obtained information.
Independent variables
To characterize the sample, the following variables were used: maternal schooling (years of full study by the mother were categorized into primary school (≤4 years of schooling), high school (5–9 years of schooling) and higher education (≥10 years of schooling)), family income per capita according to the minimum wage (computed as the sum of the incomes of all family members residing in the same household in the month prior to the interview), number of prenatal consultations, previous breast-feeding experience, pregnancy complications, use of cigarettes during pregnancy, suckling in the first hour after birth, birth weight and use of pacifiers by the infant.
Maternal nutritional status was assessed by calculating the pre-gestational BMI, which referred to the mother’s typical weight before pregnancy. Subsequently, pre-gestational BMI was categorized according to the criteria adopted by the Institute of Medicine( 15 ): low maternal weight (BMI<18·5 kg/m2), normal weight (BMI=18·5–24·9 kg/m2), overweight (BMI=25·0–29·9 kg/m2) and obesity (BMI≥30·0 kg/m2).
The data were typed into a double-entry form and processed using Epi-info software version 3.5.1. Statistical analysis was performed using PASW Statistics version 18.0. To analyse the median duration of breast-feeding practices, survival curves were constructed using the life table method, representing the cumulative probability of breast-feeding over the months. Children who were breast-fed for at least 30d by mothers spanning the four categories of pre-gestational BMI were considered. Children whose mothers reported not breast-feeding were included in the survival analysis as having breast-fed for 1d. The duration of breast-feeding was assessed retrospectively at 7 and 24 months for EBF and BF, respectively. The association between the independent variables and the duration of breast-feeding was estimated by the Wilcoxon test.
The variables that obtained P<0·20 among the infants who completed EBF (n 381) were entered in the final multiple linear regression model. The basal category for the estimation of the adjusted β value was defined as ‘the one with the lowest risk of compromising the duration of breast-feeding’, i.e. mothers whose nutritional status was normal weight.
The Human Research Ethics Committee of the Federal University of Alagoas approved the study under protocol number 09093012.0.0000.5013. The research objectives and the reliability of the data were explained to the families, and they signed the informed consent form prior to the interviews.
Results
A total of 418 mother–infant dyads were evaluated. The mean age of the mothers and children was 28 (sd 7) years and 15 (sd 6) months, respectively. There was an equal distribution of boys and girls. The mean pre-pregnancy BMI was 23·4 (sd 4·7) kg/m2.
The median duration of EBF was 1·9 months (60d), while that of BF was 8·2 months (250d). Among the children analysed, twenty-nine (6 %) never breast-fed, 214 (45 %) were still breast-feeding and 174 (36 %) had already been weaned. Among children younger than 6 months (n 106), the prevalence of EBF was 84·2 % (Fig. 1).
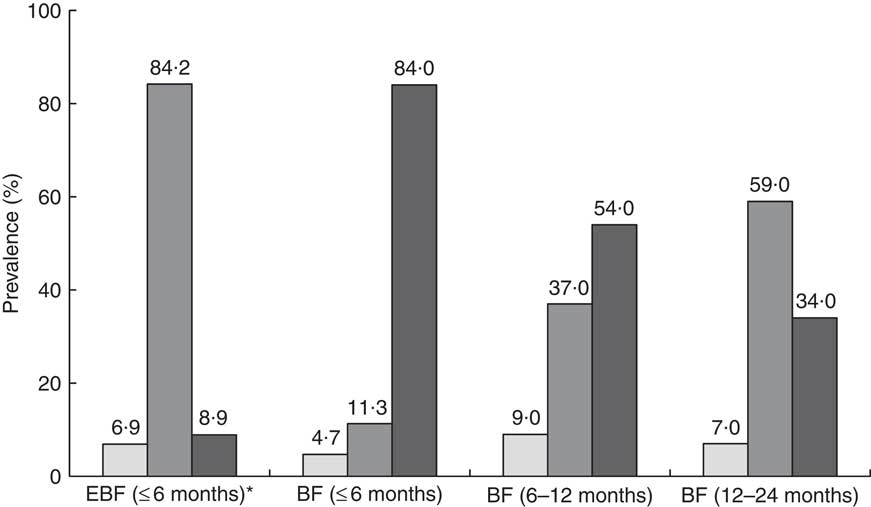
Fig. 1 Practice of exclusive breast-feeding (EBF) and breast-feeding (BF) of infants (![]() , never breast-fed;
, never breast-fed; ![]() , breast-fed;
, breast-fed; ![]() , still breast-feeding) by age group (months), Alagoas, Brazil, 2015. *Including twenty-three (5·5 %) infants (>6 and≤7 months of age) who were exclusively breast-fed
, still breast-feeding) by age group (months), Alagoas, Brazil, 2015. *Including twenty-three (5·5 %) infants (>6 and≤7 months of age) who were exclusively breast-fed
Regarding the nutritional classifications (pre-gestational BMI), 56·2 % of the mothers were normal weight, while 31·6 % had excess weight (21·3 % were overweight and 10·3 % were obese). It was observed that 98·6 % of the mothers underwent prenatal care; of these mothers, 78·9 % had six or more visits, as recommended by the Ministry of Health. Among mothers who had previous experience with breast-feeding, 53·4 % were multiparous and 26·6 % were primiparous. Among the children, 5·7 % were born with a low birth weight and 50·1 % had used pacifiers (Table 1).
Table 1 Associations of the duration of exclusive breast-feeding (EBF) and breast-feeding (BF) with explanatory variables, Alagoas, Brazil, 2015
Minimum wage at the time of the survey was R$724·00.
* Wilcoxon’s test.
† Twenty-eight cases without information.
‡ Thirty-seven cases without information.
§ Six cases without information.
║ Seventeen cases without information.
¶ Twelve cases without information.
** Five cases without information.
†† One case without information.
‡‡ Nine cases without information.
When comparing the survival curves relative to the different breast-feeding practices (Figs 2 and 3) according to the pre-gestational BMI categories, EBF soon after birth was not a universal practice among the children of obese mothers. At the end of the second month of life, only 48 % of the children received breast milk exclusively. In the following months, there was a systematic decline such that by the end of the fourth month, only 24 % of these children were being exclusively breast-fed, and only 4 % obtained this status at the sixth month of life.
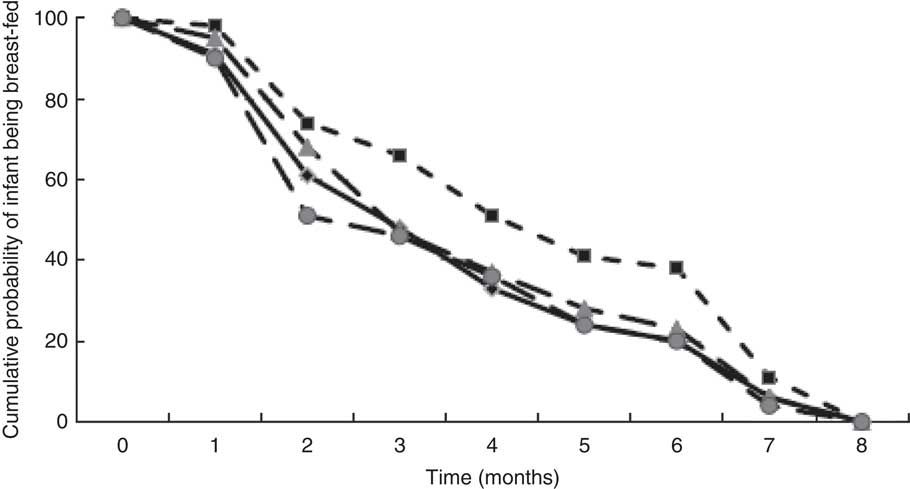
Fig. 2 Exclusive breast-feeding practice* of infants according to pre-gestational BMI† (![]() , low weight;
, low weight; ![]() , normal weight;
, normal weight; ![]() , overweight;
, overweight; ![]() , obesity), Alagoas, Brazil, 2015. *Wilcoxon’s test: P=0·045. †Low weight, BMI<18·5 kg/m2; normal weight, BMI=18·5–24·9 kg/m2; overweight, BMI=25·0–29·9 kg/m2; obesity, BMI≥30·0 kg/m2
, obesity), Alagoas, Brazil, 2015. *Wilcoxon’s test: P=0·045. †Low weight, BMI<18·5 kg/m2; normal weight, BMI=18·5–24·9 kg/m2; overweight, BMI=25·0–29·9 kg/m2; obesity, BMI≥30·0 kg/m2

Fig. 3 Breast-feeding practice* of infants according to pre-gestational BMI† (![]() , low weight;
, low weight; ![]() , normal weight;
, normal weight; ![]() , overweight;
, overweight; ![]() , obesity), Alagoas, Brazil, 2015. *Wilcoxon’s test: P<0·001. †Low weight, BMI<18·5 kg/m2; normal weight, BMI=18·5–24·9 kg/m2; overweight, BMI=25·0–29·9 kg/m2; obesity, BMI≥30·0 kg/m2
, obesity), Alagoas, Brazil, 2015. *Wilcoxon’s test: P<0·001. †Low weight, BMI<18·5 kg/m2; normal weight, BMI=18·5–24·9 kg/m2; overweight, BMI=25·0–29·9 kg/m2; obesity, BMI≥30·0 kg/m2
For BF, babies of obese mothers were less often breast-fed at ages 2–12 months, but from 18–24 months, this was instead true for the babies of the overweight mothers. However, none of these differences were tested for statistical significance.
According to the survival analysis, the duration of breast-feeding practices was significantly higher among the pre-gestational normal-weight mothers than among those with pre-gestational obesity: EBF (2·8 v. 2·3 months, P=0·045) and BF (15·5 v. 6·7 months, P<0·001). Mothers who had six or more prenatal consultations had higher medians for both breast-feeding practices, although the difference was not statistically significant. Mothers who had previous breast-feeding experience and the mothers who had not previously breast-fed because they were primiparous contributed to the significantly higher median durations of EBF (3·3 months) and BF (14·5 months) among women with previous breast-feeding experience compared with those without previous breast-feeding experience: EBF (1·8 months, P<0·01) and BF (11·3 months, P=0·023). Among children, the use of pacifiers was negatively associated with the duration of EBF when compared with the lack of use (2·2 v. 3·8 months, P<0·001).
Table 2 shows the results obtained from the multiple linear regression analysis of factors associated with the duration of EBF among the children who completed EBF (n 381). The factors that negatively and independently affected the duration of EBF were pre-gestational BMI≥30·0 kg/m2 (−51·9d, 95 % CI −80·4, −23·4d; P=0·002), maternal schooling≤9 years (−30·8d, 95 % CI −54·7, −6·9d; P=0·035), no prior lactation experience (−29·0d, 95 % CI −45·6, −11·5d; P=0·002) and infant pacifier use (−41·4d, 95 % CI −54·5, −28·2d; P<0·001).
Table 2 Multiple linear regression analysis of factors associated with the duration of exclusive breast-feeding (EBF) in infants, Alagoas, Brazil, 2015

* Wilcoxon’s test.
† Twenty-five cases without data.
‡ Sixteen cases without data.
§ Five cases without data.
║ Seven cases without data.
Discussion
The results of our sample point to a higher proportion of various breast-feeding practices in Alagoas than cited in other studies in the literature( Reference Moreira, Cabral and Ferreira 12 , Reference Ferreira, Vieira and Junior Cabral 16 ). For example, in the National Survey of Demography and Children’s and Women’s Health (PNDS)( 17 ), the percentage was 39·8 %, and the Prevalence of Breastfeeding in the Brazilian Capitals and Federal District (PPAM/Capitals and DF)( 18 ) survey reported a prevalence of 41 % in the Brazilian capitals and 37 % in the Northeast; while in the present study a proportion of maternal breast-feeding among children up to 6 months of 84·2 % was observed. The great discrepancy between these values may be due to the temporal difference between the studies in the literature, which occurred between the years of 2006 and 2008, and the present research which was conducted in 2015. These and other results in the literature are far below the desired level, as the great majority of children up to 6 months of age should be exclusively breast-fed.
Among children aged 12 months or older, a lower prevalence was observed in the current study than in the studies mentioned above( 17 , 18 ). In the literature, there are few studies on breast-feeding in the state of Alagoas, but there are studies on specific groups. For example, in the study carried out by Ferreira et al.( Reference Ferreira, Vieira and Junior Cabral 16 ), the percentage of children from the semi-arid region under 5 years of age who were breast-fed for more than 1 year was 43·5 %. In Maceió, the capital of Alagoas, Assunção et al.( Reference Assunção, Ferreira and Coutinho 11 ) found that the BF prevalence in children less than 2 years of age was 38·1 %.
The median BF duration observed in the current study was also unsatisfactory. Comparing the BF results of the present study with those obtained in the PPAM/Capitals and DF study( 18 ), the median duration of BF (250d, 8·2 months) was lower than that obtained in Brazil (341·6d, 11·2 months), the Northeast (346·8d, 11·4 months) and Maceió (331·5d, 10·9 months). When considering the PNDS( 17 ), the results were similar, as the median duration of BF was 425·9d (14 months). However, EBF practice in the current study demonstrated a slight improvement in median duration to 1·9 months (60d) when compared with that in the PPAM/Capitals and DF study( 18 ). This is possibly due to the strategies adopted by public policies to encourage and promote breast-feeding, which are being strengthened in basic care. For example, the Breastfeeding and Feeding Brazil Strategy can explain the change that we observed( Reference Anversa, Bastos and Nunes 19 , Reference Brandão, Venancio and Giugliani 20 ). Another possible explanation may be the absence of recent population information, as the information used in the study by Victora et al. was approximately 10 years old, which may be masking the real duration of BF in the Northeast region of Brazil( Reference Victora, Bahl and Barros 4 ).
The effects of pre-gestational obesity on the duration of breast-feeding practices in the current study are notable since mothers with this status displayed reduced EBF and BF behaviour when compared with mothers with other pre-gestational nutritional statuses. Similar findings were observed in surveys conducted by Castillo et al.( Reference Castillo, Santos and Matijasevich 5 ) in a longitudinal section of Pelotas, a city in Southern Brazil, that included 4231 infants. They observed a higher probability of cessation of beast-feeding at 3 months of age among infants of mothers who were obese during the pre-gestational period. Kair and Colaizy( Reference Kair and Colaizy 9 ) observed that overweight and obese women were more likely to discontinue breast-feeding than women who were of normal weight (overweight: OR=1·39; 95 % CI, 1·16, 1·68; obese: OR=1·26; 95 % CI, 1·03, 1·54). However, Oliveira et al.( Reference Oliveira, Lira and Filho 21 ) did not observe a significant association except in one municipality.
Among the possible explanations, the literature reports experimental studies with obese animals that suggest a delay of lactogenesis and less milk synthesis due to histological alterations of the mammary gland characterized by a reduction in the number of ramifications and diameter of the lactating ducts, the deposition of collagen in the lumen of the duct, the abnormal contraction of myoepithelial cells and the possible impairment of alveolar development. Additionally, excess maternal adiposity may promote excessive breast or nipple enlargement, making it difficult for the baby to correctly handle breast-feeding. Obesity may also contribute to higher rates of postpartum depression( Reference Thulier and Mercer 8 , Reference Kamikawa, Ichii and Yamaji 22 ).
The number of prenatal visits was not statistically significantly associated with median EBF or BF duration, but the median was relatively higher among mothers who had six or more visits, as recommended by the Ministry of Health. This factor may be due to the positive effect of the intervention of health professionals during prenatal care( Reference Oliveira, Lira and Filho 21 , Reference Vasconcelos, Lira and Lima 23 – Reference Gomes 25 ).
Primiparous mothers, as well as those with previous breast-feeding experience, had longer median lengths of different breast-feeding practices. This may be due to increased support from health and family professionals, as well as positive experiences with breast-feeding, that may contribute to greater self-efficacy and fewer difficulties, concerns and doubts about breast-feeding( Reference Hass, Howard and Christopher 26 ). Some researchers have reported that the duration of BF was associated with increased parity( Reference Hass, Howard and Christopher 26 – Reference Li, Ogden and Ballew 28 ). Hass et al.( Reference Hass, Howard and Christopher 26 ) found that previous breast-feeding experience was a predictor of BF continuity at 6 weeks postpartum. Using the third National Health and Nutrition Examination Survey (NHANES) conducted in the USA, Li et al.( Reference Li, Ogden and Ballew 28 ) concluded that multiparous women were less likely to initiate breast-feeding, but were more likely to breast-feed for a longer period.
Infant pacifier use was negatively associated with the duration of EBF. This result may be because when the infant uses a pacifier, the frequency of suckling from the breast decreases, resulting in a decrease in the production of breast milk. The use of pacifiers attracts attention because it causes difficulties in breast-feeding or even demonstrates anxiety and maternal insecurity about the feeding process, which warns us about the need to resolve such issues. Chaves et al.( Reference Chaves, Lamounier and César 24 ) followed a group of women for 12 months after childbirth and found a reduction in BF and EBF duration among those who used pacifiers. Silveira and Lamounier( Reference Silveira and Lamounier 29 ) carried out a literature review on studies that associated pacifier use with a shorter duration of breast-feeding, and a statistically significant association was found in all the studies.
In the present study, the average duration of different breast-feeding practices was assessed via survival analysis, and interpretation of the results must consider the interviewed mothers’ possible memory biases. However, to minimize maternal recall bias regarding dietary information of the children selected for the study, only children up to 2 years of age were included.
The survival analysis technique allows children still being breast-fed at the time of the interview to be considered and the proportion of children who remain breast-fed at the end of each month to be known. This technique therefore allows longitudinal ‘treatment’ of cross-sectional data. However, to perform the multivariate analysis, only children who had stopped breast-feeding were considered since they had an actual median referring to EBF duration.
In addition to the factors mentioned above, multiple linear regression analysis detected a low maternal level of education as a factor associated with a reduced duration of EBF. Mothers with a lower level of schooling may not understand the importance of EBF for children and offer their children water, tea and milk formula before the sixth month of life( Reference Oliveira, Lira and Filho 21 ).
The findings show a short duration of EBF among women with pre-gestational obesity and prenatal care may provide an opportunity to guide and encourage mothers to breast-feed their children and to achieve adequate weight gain during pregnancy.
Additionally, the present study may expand and update the situational diagnoses of the health and nutrition of maternal–infant groups in the state of Alagoas to inform government policies and programmes, specifically in relation to high pre-pregnancy BMI and the duration of breast-feeding among children up to 24 months of age.
The construction of other methodological approaches that elucidate individual and social factors to improve the actions taken in prenatal consultations is also recommended.
Acknowledgements
Acknowledgements: The authors thank the members of the Laboratory of Basic and Applied Nutrition for their help and interest in carrying out the field research. Financial support: This work was supported by the Foundation for Support to Science and Technology of the State of Pernambuco (FACEPE; A.M.S., scholarship) and the National Council of Scientific and Technological Development (CNPq; H.S.F, P.I.C.L., financing of the field research and productivity grants). FACEPE and CNPq had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: A.M.S. was responsible for the conception of the study, collected the data, interpreted the data and worked on the writing of the article; H.S.F. carried out the general review; M.L.A. collected the data and carried out the general review; P.I.C.L. worked on designing the study, interpreting the data, guiding the writing of the article and critically reviewing the content of the final version. Ethics of human subject participation: The Human Research Ethics Committee of the Federal University of Alagoas approved the study under protocol number 09093012.0.0000.5013. The families provided informed consent prior to the interviews.





