


Pregnancy encompasses a series of physiological, metabolic and nutritional adaptations in women’s body(Reference Hill and Pickinpaugh1,Reference Carlin and Alfirevic2) , since rapid fetal growth and development demand different energy nutrient intake(Reference Hill and Pickinpaugh1). It is essential meeting this demand to assure the adequate health of the mother–child binomial, mainly due to the critical window of opportunities for fetal development(Reference Watson and McDonald3,Reference Jang, Kim and Lee4) . Thus, pregnant women represent an attractive population group, whose eating habits must be well understood to help assessing future pregnancy outcomes(Reference Jang, Kim and Lee4,Reference Raghavan, Dreibelbis and Kingshipp5) .
The number of surveys gathering information about populations’ dietary and health standards has increased in recent years, mainly when it comes to pregnant women(Reference Johnson, Santos and Sparks6–Reference Vian, Zielinsky and Zilio8), since this population has been associated with the epidemiologic transition, whose expressive increase lies on the worrying incidence of chronic non-communicable diseases(Reference Costa, Del-Ponte and Assunção9,Reference Canella, Levy and Martins10) .
Thus, different methods have been used to assess food intake(Reference Cade, Thompson and Burley11,Reference Willett, Sampson and Stampfer12) – food record and 24-hour-dietary recall (24 hR) are the most used ones(Reference Kerr, Wright and Dhaliwal13,Reference Ortega, Pérez-Rodrigo and López-Sobaler14) . However, these methods can lead to underreported food intake, since it is necessary adopting multiple applications to minimise intra and interpersonal, as well as seasonal, variations(Reference Kirkpatrick and Collins15,Reference Castell, Serra-Majem and Ribas-Barba16) . Therefore, the FFQ developed and validated for the herein investigated population is a valuable tool that allows investigating the usual diet of the target group in a proper manner(Reference Willett, Sampson and Stampfer12).
Given the lack of validated methods to analyse the food intake of pregnant women, the aim of the current study was to validate and evaluate the reproducibility of a FFQ developed for pregnant women living in Northeastern Brazil.
Methods
Sample
FFQ validation study and reproducibility analysis were carried out with pregnant women treated in the public health network in Maceió City (AL) in 2019.
Maceió City is located in Northeastern Brazil; its estimated population comprises 1 018 948 inhabitants and its Municipal Human Development Index is 0·721(17).
Nowadays, the local public health network is strategically divided into eight health districts comprising the total number of sixty-seven Basic Health Units (BHU). A random drawing of two BHU per health district (sixteen units, in total) was carried out to select the BHU in the current study. After the BHU definition process was over, the number of pregnant women treated in each unit was identified based on a list provided by the Municipal Health Department. Subsequently, the healthcare contribution rate of each unit was calculated, and the resulting values were used to calculate the proportional distribution of pregnant women to be recruited.
Recommendations by Cade et al. (Reference Cade, Thompson and Burley11) and Serra-Majem et al. (Reference Serra-Majem, Andersen and Sánchez18) were used to define the sample size, which comprised 100 pregnant women.
The inclusion criteria set for individuals’ participation in the study were: 25-to-35-week pregnant women living in Maceió City, who were treated in the local public health network (the FFQ was developed to assess participants’ food intake in the last six gestational months). Pregnant women with multiple pregnancies, with chronic or specific gestational diseases, illiterate, diagnosed with cognitive issues, as well as those with neurological or locomotion issues capable of hindering the interview or the anthropometric assessment were not included in the study.
Participants were recruited through convenience method at prenatal consultation time, when information about them was initially checked in their medical records by taking into consideration previously defined exclusion and inclusion criteria. Once participants met these criteria, they were invited to participate in the research. Those who agreed to participate in it were subjected to the first interview.
Maternal data
Properly trained interviewers were in charge of collecting participants’ data; each interviewer accounted for applying all research stages to the same volunteer. Pregnant women were given a standardised questionnaire comprising socio-economic (family income, receipt of government assistance, education and marital status), lifestyle (physical activity, drinking and smoking habits), obstetric (history of abortions or miscarriages), number of previous pregnancies and prenatal consultations (use of supplements/medications, among others), food intake (FFQ and 24 hR) and anthropometric assessment information.
Weight variables were measured in Marte LC200® digital scale and height was measured with the aid of Cardiomed® portable stadiometer, at interview time, to assess anthropometric data. These variables were used to calculate participants’ BMI; anthropometric diagnosis was based on Atalah Samur and collaborators(Reference Atalah, Castillo and Castro19). In addition, pre-gestational weight (used to calculate pre-gestational BMI) and weight gain during pregnancy were investigated based on the American Institute of Medicine (IOM-USA)(Reference Rasmussen and Yaktine20).
Validation and reproducibility of the FFQ
The FFQ adopted in the current research was developed based on a database comprising 650 24 hR (two per pregnant woman) from a survey carried out in 2013 with pregnant women treated at the BHU in Maceió. The list of food items was defined based on Block et al. (Reference Block, Dresser and Hartman21), whose list of food items included food types that contributed to approximately 95 % of nutrients of interest in the current research. The final version of the herein developed FFQ presented 112 food items categorised into food groups based on NOVA classification(Reference Monteiro, Cannon and Levy22), which defines portion size (small, medium, large) and frequency by taking into consideration daily, weekly and monthly food intake. In addition, the elaborated FFQ was designed to be applied through interviews; it refers to the usual food intake in the last 6 months prior to its application to pregnant women.
Three 24 hR and two FFQ were applied at 15-d intervals between research stages in order to confirm the validity and reproducibility of the FFQ, as shown in Fig. 1.
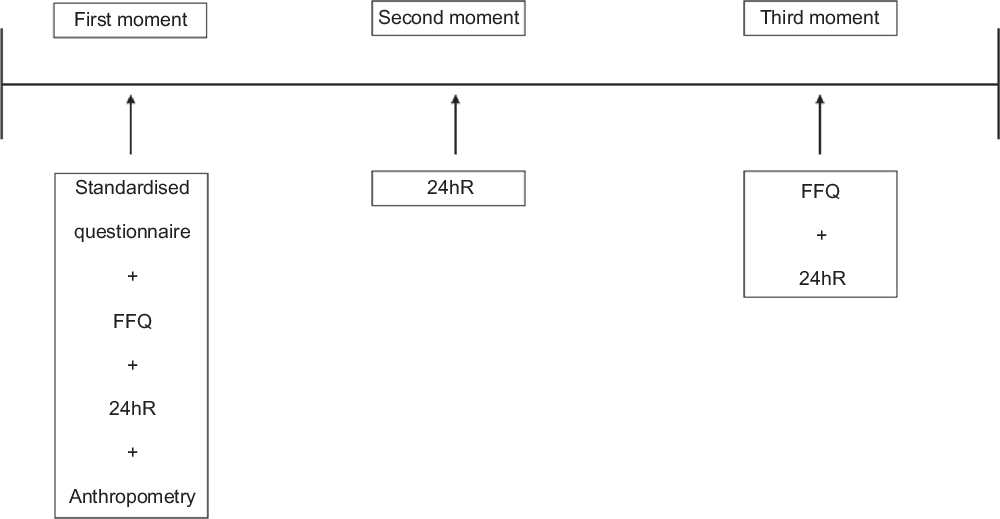
Fig. 1 Systematisation of the validation and reproducibility stages applied to the FFQ developed for pregnant women. Maceió, Alagoas State, Brazil, 2020
Data about the first and third 24 hR were collected at the BHU, based on information about participants’ food intake 24 h before the interview, which followed the order of meals. A photo album specifically developed for the current research was used to record the consumed food and beverages, the quantity in homemade measures, the preparation form, the place and time of food intake, as well as details about the brand and features of industrialised products. Data about the second 24 hR were collected through phone call 15 d after the first survey – such information corresponded to participants’ food intake in atypical days (weekend)(Reference Tran, Johnson and Soultanakis23).
Some aspects were taken into consideration to help pregnant women (pregnant adolescents as well) to better understand the instrument used to assess them, namely (a) illiterate pregnant women were not included in the survey; (b) some aspects were taken into account at FFQ elaboration time to help better understand the applied instrument; among them one finds the vertical format of the instrument (it was considered the most suitable for application in children, elderly and low-schooling populations) enabled presenting the frequency options of each food in separate, as well as including frequency categories and portion sizes in the FFQ to help reduce coding time, error transcription and the number of questionnaires to be rejected due to incomplete or blank answers(Reference Cade, Thompson and Burley11,Reference Barbosa, Rosado and Franceschini24) ; (c) the questionnaire was applied by the researcher, who previously informed volunteers about the format and content of the instrument and (d) use of food photo album to help better understand the instrument(Reference Brito, Araujo and Guimarães25).
Energy and nutrient intake estimates
The food intake frequency reported by the participants was converted into daily intake in g or ml in order to determine the nutritional content of the items included in the FFQ. Food intake frequency was multiplied by the informed portion and the product was defined as daily intake; it was divided by 7 to define weekly food intake, and by 30, for monthly intake.
Subsequently, total energy, macro and micronutrient values of the FFQ and 24 hR were determined based on the nutritional assessment and prescription system (Avanutri 4·0®). Whenever the software did not present nutritional values of regional food items, these items were inserted in it with the aid of the Brazilian Food Composition Table – TACO(26).
Statistical analysis
Data were processed in the Statistical Package for the Social Sciences software version 20.0. The Kolmogorov–Smirnov test was used to assess the normality of variables; logarithmic transformation was applied to variables that did not present Gaussian distribution.
Descriptive statistics results were expressed as means (sd), medians and frequencies. Wilcoxon test was applied to compare the energy, macro and micronutrient values of the FFQ and the mean of the 24 hR.
Pearson’s (Gaussian distribution) and Spearman’s (variables that did not present Gaussian distribution) correlation coefficients were used to compare the energy and nutrient values of the first FFQ to the mean of all three 24 hR. Correlation values ranging from 0·40 to 0·70 have indicated good agreement between the two food intake assessment methods(Reference Willett27).
Correlation coefficients were adjusted to intrapersonal and interpersonal variability (obtained through ANOVA test) to eliminate likely confounding factors. In order to do so, macro and micronutrients of all three 24 hR were adjusted to energy, based on the residual method(Reference Willett27). This process comprised the following three steps: (1) constant and regression coefficient were estimated based on a simple linear regression model, according to which, nutrients of interest were adopted as dependent variables and energy was the independent variable; (2) the constant added to the residues was calculated – this variable was used as the predictive value for the nutrient-of-interest intake necessary to meet the mean energy intake by the investigated population and (3) nutrient intake adjusted to energy intake was estimated. In addition, the correlation coefficients attenuated by intrapersonal variability were obtained based on the following formula:
 $${R_c} = {r_o}\surd [1 + ({S^2}_W/{S^2}_B)]/n,$$
$${R_c} = {r_o}\surd [1 + ({S^2}_W/{S^2}_B)]/n,$$
wherein r o is the observed correlation, S 2 W /S 2 B is the intrapersonal/interpersonal variance ratio and n is the number of repetitions of each variable per person(Reference Nusser, Carriquiry and Dodd28).
The intraclass correlation coefficients (ICC) of nutrients between the two FFQ were calculated for reproducibility analysis purposes.
P value < 0·05 was significant in all tests.
Results
One hundred pregnant women (mean age of 24·74 (sd 6·35) years) were included in the study: 25·0 % of them were adolescents and 8·0 % were ≥35 years old; mean gestational time at interview time was 29·02 (sd 3·66) weeks.
With respect to participants’ socio-economic, lifestyle and anthropometric features, 74·7 % had monthly family income ≥ 1 minimum wage (mean income of R$ 1440·71 (sd 1029·32) reais); 66·0 % reported not to work outside the home; 71·0 % had stable union; 18·0 % were smokers and 6·0 % had alcohol use disorder; 30·3 % were overweight in the pre-pregnancy period; 36·3 % got overweight during pregnancy and 71·7 % of them presented inadequate gestational weight gain (Table 1).
Table 1 Features of pregnant women treated in the public health network. Maceió City-Alagoas State, Brazil, 2019
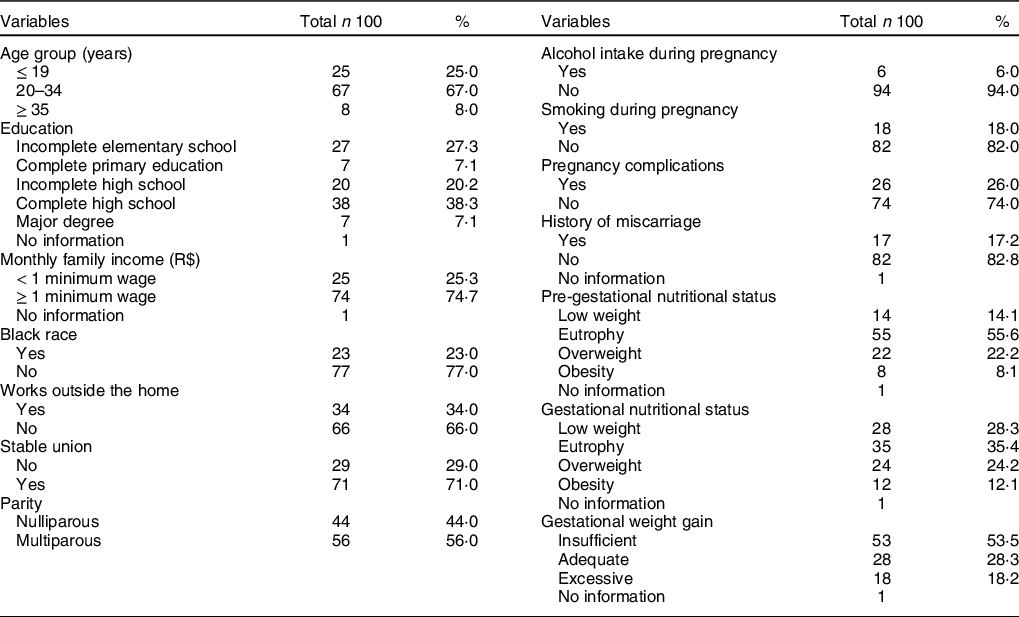
Table 2 shows the median and percentile values (25; 75) recorded for the estimated energy, macro and micronutrient intake reported in FFQ1 and FFQ2 and the 24 hR. There was a significant difference in the intake of most nutrients between FFQ1 and FFQ2, which recorded the lowest values.
Table 2 Daily intake of energy, macro and micronutrient based on the FFQ1 and FFQ2 and 24 hR of pregnant women treated in the public health network. Maceió City-Alagoas State, Brazil, 2019

Wilcoxon test; 24 hR: 24-h-dietary recall.
* Mean of three 24 h.
** P < 0·001.
Table 3 shows raw, adjusted and attenuated data referring to the FFQ validation. Fourteen out of the total number of twenty-five nutrients have shown correlation ≥ 0·40; according to total raw data, nutrients ranged from 0·92 (phosphorus) to 0·10 (protein, vitamin D, folate and Na). According to the energy-based adjustment, a significant part of the nutrients has shown correlation equal to, or lower than, the raw data - values ranged from 0·43 (energy, carbohydrate and Mg) to 0·02 (vitamin D). Table 3 also shows that correlation coefficients calculated for attenuated data were substantially higher than those calculated for raw data, except for protein, vitamin D, folate and Na, which recorded values equal to the crude coefficients.
Table 3 Correlation coefficient between FFQ1 and the mean recorded for the 24 hR of pregnant women treated in the public health network. Maceió City-Alagoas State, Brazil, 2019

* P < 0·05.
** P < 0·01.
*** P < 0·001.
† Pearson’s correlation with logarithmic variables.
‡ Spearman’s correlation.
Finally, Table 4 presents reproducibility data, which recorded high ICC for Mg (r = 0·72), Fe (r = 0·65), lipid (r = 0·56) and energy (r = 0·55), as well as lower ICC for Mn (r = 0·02), vitamin B12 (r = 0·07) and vitamin D (r = 0·14). Participants reported greater intake of all nutrients in FFQ1 than in FFQ2.
Table 4 ICC between FFQ1 and FFQ2 applied to pregnant women treated in the public health network. Maceió City-Alagoas State, Brazil, 2019
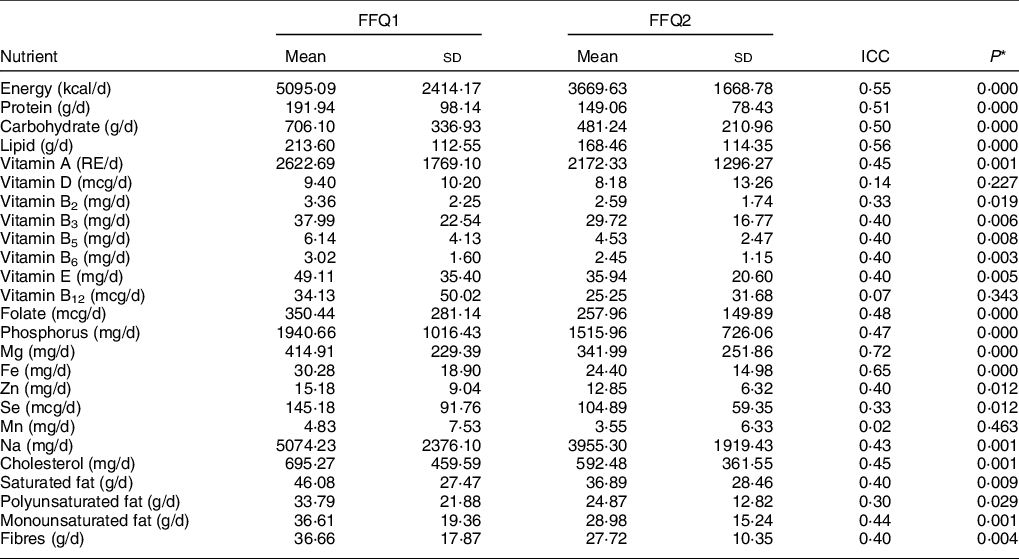
ICC, intraclass correlation coefficient.
* P < 0·05.
Discussion
The current study has presented the validity and reproducibility of a FFQ comprising 112 food items, which was specifically developed for pregnant women living in a capital city in Northeastern Brazil. To the best of our knowledge, this is the first survey aimed at testing a FFQ developed for this population by taking into account participants’ eating habits and local reality.
The herein proposed FFQ comprised food items often consumed by pregnant women living in the region (manioc, couscous, sweet potatoes); it evaluated twenty-five nutrients and showed adequate validity for this population. The FFQ was the instrument selected to be validated in the current research because it has the advantage of assessing food intake over a long period of time in a simple and economical way(Reference Coulston, Boushey and Ferruzzi29,Reference Shim, Oh and Kim30) .
Overall, the herein identified nutrients were overestimated in the FFQ in comparison to the 24 hR nutrients, and in FFQ1 in comparison to FFQ2. The Similar fact was also reported in other FFQ validation studies that have used the same survey as reference method(Reference Silva-Jaramillo, Neutzling and Drehmer31–Reference Dehghan, Cerro and Zhang33). Research focused on evaluating the validation and reproducibility of a FFQ adapted to the adult Moroccan population and a study aimed at applying a FFQ developed for Lebanese pregnant women have also identified the overestimation of the instrument in comparison to the 24 hR(Reference Papazian, Hout and Sibai34,Reference Kinany, Larsen and Khalis35) . Overestimation can be justified by the exorbitant description of intake frequency, increased portion size or lack of intake of some food items in the 24 hR. Therefore, overestimation is not an issue in epidemiological studies, since individuals are classified based on food intake levels(Reference Beaton36,Reference Barbieri, Crivellenti and Nishimura37) . Because FFQ1 presented higher mean values than FFQ2, results found in other studies were similar to ours. This outcome can be explained by pregnant women’s likely adaptation to the applied instrument, as well as by their greater involvement and attention at the time to complete the questionnaire(Reference Kinany, Larsen and Khalis35,Reference Harmouche-Karaki, Mahfouz and Obeyd38) .
The mean recorded for the unadjusted correlation coefficients between FFQ1 and 24 hR was 0·42–14 nutrients, which were considered valid for women’s food intake assessment (r ≥ 0·4)(Reference Willett, Sampson and Stampfer12). These values were higher than, or similar to, those reported in other studies conducted with pregnant women, such as the one carried out with Lebanese pregnant women, whose correlation coefficients ranged from 0·29 (Fe) to 0·76 (energy)(Reference Papazian, Hout and Sibai34), as well as the study by Ogawa et al. (Reference Ogawa, Jwa and Kobayashi39), who reported correlation coefficients ranging from 0·09 to 0·40 (nutrients) in Japanese women at early pregnancy stage.
Energy-based adjusted correlation coefficients recorded decreased values for almost all nutrients, which may indicate high food intake variation among pregnant women. The mean of coefficients increased from 0·42 to 0·45 after dilution (i.e., after the effects of intrapersonal variance were eliminated) – these values were higher than that reported (0·35) in a study conducted with Brazilian pregnant women living in Ribeirão Preto County/SP(Reference Barbieri, Nishimura and Crivellenti40).
Higher correlation coefficients were observed for phosphorus and monounsaturated fat intake, whose values ranged from 0·92 to 0·87. This finding can be associated with the fact that some food items contributing to the intake of these nutrients were consumed more often or by a larger number of pregnant women.
Results in the current study have indicated FFQ reproducibility for 19/25 (76·0 %) of the evaluated nutrients – ICC ranged from 0·07 (vitamin B12) to 0·72 (Mg). Li et al. (Reference Li, Halldorsson and Bjerregaard41) have investigated healthy pregnant women living in rural China and found similar ICC, according to which fourteen of the eighteen evaluated nutrients presented correlation coefficient ≥0·40 - values ranged from 0·27 to 0·79.
The interval between FFQ applications is extremely important to assure its reproducibility(Reference Cade, Thompson and Burley11). Thus, FFQ applied at short intervals may have their reproducibility overestimated, since participants can recall previous responses. Conversely, FFQ are expected to present lower reliability in applications carried out over long periods of time, since participants’ diet can face sudden changes(Reference Cade, Thompson and Burley11,Reference Willett, Sampson and Stampfer12) . The current study respected the 1-month interval between FFQ applications 1 and 2, as recommended(Reference Cade, Thompson and Burley11).
The following aspects prevailed among pregnant women evaluated in the current study: middle age, complete high school, monthly family income greater than, or equal to, one minimum wage and adequate nutritional status (eutrophy) in the pre-gestational and gestational periods. Changes in these variables represent risk factors for gestational complications(Reference Dou, Zhao and Lu42,Reference Bashir, Dabbous and Baagar43) . It should be noticed that gestational complications were not identified in the evaluated women, as well as that the previous limitation in the selection of pregnant women with non-communicable diseases allowed reducing factors capable of changing participants’ food intake.
Limitations observed in 24 hR comprised memory bias; collaboration by interviewees, depending on their ability, psychological conditions and cognitive level; a single recall cannot estimate the usual nutrient intake and difficulty in estimating portion size(Reference Shim, Oh and Kim30). The 24 hR is widely used in epidemiological research, since it is a low-cost method that does not affect participants’ food intake and can be applied to any age group regardless of educational or socio-economic level(Reference Foster and Bradley44,Reference Luke, Bovet and Forrester45) .
It is important highlighting some limitations observed in the current study. It was not possible using more precise methods such as the real Food Register and/or biochemical analyses in order to validate the FFQ; thus, we chose to use 24 hR because it was the most technically feasible method. The mean recorded for three 24 hR (a considerable number of days to assess participants’ usual intake) was used to minimise this limitation and to adjust nutrients based on energy in order to minimise correlated errors between the two methods. In addition, it was not possible performing random sampling.
In addition to the limitations observed for the 24 hR, FFQ has method-inherent limitations such as memory bias and response overestimation. However, techniques such as detailed description and review have been adopted to minimise these limitations.
One cannot ignore the fact that one-fourth of the current sample comprised pregnant teenagers. Some studies that brought this population together with groups of children and elderly individuals have shown some difficulty in understanding the elaborated FFQ,(Reference Barbosa, Rosado and Franceschini24) which could make these studies viable. The current research has taken some precautions to avoid this type of situation; among them, one finds: illiterate pregnant women were not included in the survey; the questionnaire was prepared in vertical form, which included frequency categories and portion sizes; the instrument was applied by the researcher; and food photo album using.
The current study differs from research already carried out in Brazil because the herein adopted instrument was specifically developed for pregnant women living in a capital city in Northeastern Brazil, which is a region that lacks studies, mainly in the food intake field.
In addition, the elaborated FFQ presented satisfactory validation for energy, carbohydrate, vitamins B2, B5, E, B12, phosphorus, Mg, Se, cholesterol, saturated, polyunsaturated and monounsaturated fats, and fibres. Similarly, it has shown satisfactory reproducibility for energy, protein, carbohydrate, lipid, vitamins A, B3, B5, B6 and E, folate, phosphorus, Mg, Fe, Zn, Na, cholesterol, saturated and monounsaturated fats, and fibres.
Therefore, the herein developed FFQ is a potentially useful tool to be used in research context to help determining the routine dietary intake of pregnant women living in Northeastern Brazil.
Acknowledgements
Financial support: Coordination for the Improvement of Higher Education Personnel (CAPES). Financial support for a master’s scholarship. Conflict of interest: None. Authorship: M.C.d.S.T., T.M.W., I.A.M., A.L.A.V., B.G.S. contributed to data collection and writing of the article; T.A.S. with the writing of the article; A.C.M.O. with the conception and design and writing of the article; all authors contributed to the critical review of the article and approval of the final manuscript. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethics Committee of the Federal University of Alagoas. Written informed consent was obtained from all subjects/patients.





