



Introduction
A large body of evidence confirms that children and adolescents who are exposed to victimization face increased risk of diverse negative outcomes by early adulthood, including psychopathology (Bowes, Reference Bowes2015; Jaffee, Reference Jaffee2017; Norman et al., Reference Norman, Byambaa, De, Butchard, Scott and Vos2012; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018), lower educational and career attainment (Brown & Taylor, Reference Brown and Taylor2008; Currie & Widom, Reference Currie and Widom2010), and risk markers for inflammatory disease (Baldwin et al., Reference Baldwin, Arseneault, Caspi, Fisher, Moffitt, Odgers and Danese2018; Copeland et al., Reference Copeland, Wolke, Lereya, Shanahan, Worthman and Costello2014; Rasmussen et al., Reference Rasmussen, Moffitt, Eugen-Olsen, Belsky, Danese, Harrington and Caspi2019). Another potentially important outcome is loneliness, a form of psychological distress associated with perceived shortcomings in one's social relationships (Peplau & Perlman, Reference Peplau, Perlman, Peplau and Perlman1982). Loneliness is particularly common among adolescents and young adults (Luhmann & Hawkley, Reference Luhmann and Hawkley2016). However, individuals vary in their susceptibility to feeling lonely, and there is evidence that this vulnerability could be shaped by adverse peer experiences earlier in life, such as being the victim of violence (Matthews et al., Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor, Kepa and Arseneault2019).
According to an evolutionary model of loneliness, humans are motivated to seek social connection as it confers a sense of safety (Cacioppo et al., Reference Cacioppo, Hawkley, Ernst, Burleson, Berntson, Nouriani and Spiegel2006). Being subjected to victimization is a sign that one's safety has been compromised, and this could in turn elicit a feeling that one's network of social connections is deficient and not fulfilling the functions desired of it. It is therefore plausible that feelings of loneliness could increase subsequent to a victimization exposure. If robust associations between victimization and loneliness can be established, this could inform future research questions about a potential mediating role of loneliness in the associations between youth victimization and later outcomes.
Differential effects of victimization on loneliness
Much of the research on childhood victimization and loneliness has focused on bullying (Pavri, Reference Pavri2015). Notably, bullying is a very specific form of victimization, the distinct features of which could have important implications (Arseneault, Reference Arseneault2018). First, bullying takes place between peers of a similar age. Given the important role of peer acceptance in shaping children's sense of belonging (Qualter et al., Reference Qualter, Vanhalt, Harris, Van Roekel, Lodder, Bangee and Verhagen2015), being bullied by peers could therefore have particularly strong implications for loneliness compared to other forms of victimization. Second, bullying is characterized by an imbalance of power in favor of the perpetrator. Thus, children who become victims of bullying are often characterized by certain pre-existing disadvantages that make it harder to defend themselves. This highlights the importance of controlling for vulnerabilities that frequently co-occur with both bullying and loneliness, such as depression and anxiety, to test whether loneliness in bullied individuals occurs only in the context of these other problems, or whether an association exists even in their absence.
In the adolescent literature, there has been an increasing focus on internet or “cyber” victimization, due to the growing ubiquity of digital technology in everyday life, particularly among younger generations. This form of victimization has its own distinct characteristics in comparison to offline forms: it takes place away from any physical location, the identity of the perpetrator may not be known, and it can continue even if the victims remove themselves from the situation (Przybylski & Bowes, Reference Przybylski and Bowes2017). As a relatively new phenomenon, conceptual and methodological approaches to cybervictimization have varied widely, and consequently, so too have estimates of its prevalence and effects on mental health (Nixon, Reference Nixon2014). Nonetheless, there is evidence that cybervictimization is associated with greater loneliness and other emotional problems in young people (Olenik-Shemesh, Heiman, & Eden, Reference Olenik-Shemesh, Heiman and Eden2012; Varghese & Pistole, Reference Varghese and Pistole2017).
Beyond bullying and cybervictimization, other forms of victimization may also play a role in the emergence of loneliness. For instance, emotional maltreatment may disrupt the formation of secure attachments, negatively shaping individuals’ perceptions of their relationships with others (Taillieu, Brownridge, Sareen, & Afifi, Reference Taillieu, Brownridge, Sareen and Afifi2016). Being physically harmed by an adult could elevate vigilance for threat, resulting in low trust, avoidant behaviors, and difficult social encounters (McCrory, Gerin, & Viding, Reference McCrory, Gerin and Viding2017). Victims of sexual assault may feel unable to disclose their experiences, due to perceived stigma or an expectation that they will not be believed (Sable, Danis, Mauzy, & Gallagher, Reference Sable, Danis, Mauzy and Gallagher2006). All such possibilities could be reflected in elevated feelings of loneliness. Moreover, exposure to multiple forms of victimization (“polyvictimization”) could have a dose-response association with loneliness, as has been observed for other mental and physical health outcomes (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards and Marks1998). This highlights the value of measurement approaches that capture diverse forms of victimization that vary in terms of the nature of the exposure (e.g. physical, emotional, sexual), the perpetrator (e.g. family members, peers, strangers), the context (e.g. home, school, online), and the severity (Fisher et al., Reference Fisher, Caspi, Moffitt, Wertz, Gray, Newbury and Arseneault2015).
Temporal priority and genetic confounding
The directionality of the associations between victimization and loneliness is not straightforward. Although loneliness could be an outcome of victimization, an alternative hypothesis is that lonely children are seen by perpetrators as easy targets: traits such as shyness and low confidence could make it harder for them to defend themselves, and thus make them more likely to be singled out (Acquah, Topalli, Wilson, Junttila, & Niemi, Reference Acquah, Topalli, Wilson, Junttila and Niemi2016; Pavri, Reference Pavri2015). Moreover, negative stereotypes attached to the concept of loneliness could lead to lonely children being ill-treated by their peers (Rotenberg & Kmill, Reference Rotenberg and Kmill1992). If this were the case, associations between childhood victimization and feelings of loneliness later in development could simply reflect the continuity of pre-existing loneliness in childhood. Alternatively, victimization and loneliness may predict one another in a bidirectional manner. In addition, the timing of the exposure during development may play a role in shaping the associations between victimization and loneliness: certain types of victimization may exert distinct effects when experienced in childhood versus adolescence (Logan-Greene, Nurius, Hooven, & Thompson, Reference Logan-Greene, Nurius, Hooven and Thompson2015; Troop-Gordon, Reference Troop-Gordon2017). These considerations necessitate longitudinal study designs, with repeated measures spanning multiple developmental stages, to disentangle the temporal priority of associations and test the possibility of “critical periods” for victimization exposure.
Another issue that bears consideration is that associations between victimization and loneliness could be confounded by genetic risk. Behavioral genetics research shows that variation in most psychological traits is partially explained by genetic differences; that is, individuals carrying certain genetic variants are more likely to have the trait than others (Plomin, DeFries, Knopik, & Neiderhiser, Reference Plomin, DeFries, Knopik and Neiderhiser2016). Moreover, the genetic influences on one trait often overlap with other traits, meaning that a correlation between two phenotypes could be driven by an underlying genetic correlation. The heritability of loneliness (that is, the proportion of variance accounted for by genetic influences) is approximately 40–50% (Goossens et al., Reference Goossens, van Roekel, Verhagen, Cacioppo, Cacioppo, Maes and Boomsma2015; Matthews et al., Reference Matthews, Danese, Wertz, Odgers, Ambler, Moffitt and Arseneault2016). Victimization, though ostensibly an environmental exposure, also does not happen at random and there may be heritable traits that increase the risk of a person becoming a victim (Ball et al., Reference Ball, Arseneault, Taylor, Maughan, Caspi and Moffitt2008; Beaver, Boutwell, Barnes, & Cooper, Reference Beaver, Boutwell, Barnes and Cooper2009; Beckley et al., Reference Beckley, Caspi, Arseneault, Barnes, Fisher, Harrington and Moffitt2018). To the extent that the same genetic influences that place individuals at risk of victimization also contribute to loneliness, the association between these phenomena may be confounded. This can be ruled out by comparing outcomes in monozygotic twin pairs who are matched for their genomes but discordant in their exposure to victimization. This method has allowed the robustness of the association between victimization and mental health to be stringently tested (Jaffee, Caspi, Moffitt, & Taylor, Reference Jaffee, Caspi, Moffitt and Taylor2004; Pingault et al., Reference Pingault, O'Reilly, Schoeler, Ploubidis, Rijsdijk and Dudbridge2018; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018).
Aim of study
In the present study, we used a developmental cohort of twins to explore the associations between victimization and loneliness between childhood and young adulthood. Multiple forms of victimization were considered, spanning different contexts, perpetrators, levels of severity, and developmental periods. As well as investigating the independent effects of different form of victimization, we tested for a cumulative effect of experiencing multiple forms of victimization. We also exploited both cross-sectional and longitudinal associations to test the directionality of effects. Furthermore, the robustness of associations was tested, first by controlling for concomitant psychopathology, and second by examining within-twin pair discordance in victimization to control for unmeasured familial sources of confounding.
Methods
Participants
Participants were members of the Environmental Risk (E-Risk) Longitudinal Twin Study, which tracks the development of a birth cohort of 2,232 British children. The sample was drawn from a larger birth register of twins born in England and Wales in 1994–1995 (Trouton, Spinath, & Plomin, Reference Trouton, Spinath and Plomin2002). Full details about the sample are reported elsewhere (Moffitt & E-Risk Study Team, Reference Moffitt2002). Briefly, the E-Risk sample was constructed in 1999–2000, when 1,116 families (93% of those eligible) with same-sex 5-year-old twins participated in home-visit assessments. This sample comprised 56% monozygotic (MZ) and 44% dizygotic (DZ) twin pairs; sex was evenly distributed within zygosity (49% male). In the study, 90% of participants were of White ethnicity.
Families were recruited to represent the UK population with newborns in the 1990s, to ensure adequate numbers of children in disadvantaged homes and to avoid an excess of twins born to well-educated women using assisted reproduction. The study sample represents the full range of socioeconomic conditions in Great Britain, as reflected in the families’ distribution on a neighborhood-level socioeconomic index (ACORN [A Classification of Residential Neighbourhoods], developed by CACI Inc. for commercial use) (Odgers, Caspi, Bates, Sampson, & Moffitt, Reference Odgers, Caspi, Bates, Sampson and Moffitt2012; Odgers et al., Reference Odgers, Caspi, Russell, Sampson, Arseneault and Moffitt2012). Specifically, E-Risk families’ ACORN distribution matches that of households nation-wide: 25.6% of E-Risk families live in “wealthy achiever” neighborhoods compared to 25.3% nationwide; 5.3% versus 11.6% live in “urban prosperity” neighborhoods; 29.6% versus 26.9% live in “comfortably off” neighborhoods; 13.4% versus 13.9% live in “moderate means” neighborhoods, and 26.1% versus 20.7% live in “hard-pressed” neighborhoods. E-Risk underrepresents “urban prosperity” neighborhoods because such houses are likely to be childless.
Follow-up home visits were conducted when the children were aged 7 (98% participation), 10 (96%), 12 (96%), and at 18 years (93%). There were 2,066 children who participated in the E-Risk assessments at age 18, and the proportions of MZ (56%) and male same-sex (47%) twins were almost identical to those found in the original sample at age 5 years. The average age of the twins at the time of the assessment was 18.4 years (SD = .36); all interviews were conducted after their 18th birthday. There were no differences between those who did and did not take part at age 18 in terms of socioeconomic status (SES) assessed when the cohort was initially defined (χ2 = .86, p = .65), age-5 IQ scores (t = .98, p = .33), or age-5 emotional or behavioral problems (t = .40, p = .69, and t = .41, p = .68, respectively).
Home visits at ages 5, 7, 10, and 12 years included assessments with participants as well as their mother (or primary caretaker). The home visit at age 18 included interviews only with the participants. The Joint South London and Maudsley and the Institute of Psychiatry Research Ethics Committee approved each phase of the study. Parents gave informed consent and twins gave assent between 5–12 years and then informed consent at age 18.
Measures
Victimization
Childhood victimization was assessed repeatedly when participants were 5, 7, 10, and 12 years old, including physical/sexual abuse, emotional abuse and neglect, physical neglect, and bullying by peers. Exposures were coded from 12-year dossiers for each child that comprised information from home-visit staff, mothers, children, family doctors, and child-protection interventions. Each exposure across childhood was coded for severity or frequency on a 3-point scale (Table 1).
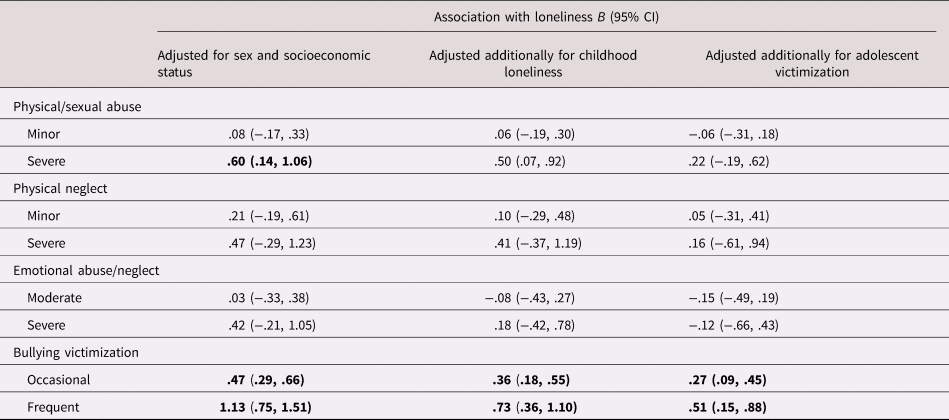
Table 1. Associations between childhood victimization and childhood loneliness (age 5–12 years)
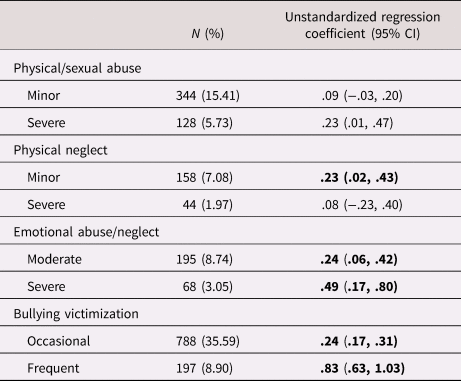
N = Number; CI = Confidence interval. All associations adjusted for sex and socioeconomic status. Associations shown in bold are significant using the Benjamini–Hochberg procedure with a false discovery rate of .05.
Adolescent victimization was assessed at age 18, when participants were interviewed about experiences between ages 12 and 18 using the Juvenile Victimization Questionnaire (Finkelhor, Hamby, Turner, & Ormrod, Reference Finkelhor, Hamby, Turner and Ormrod2011), adapted as a clinical interview. Age 12 is a salient age for our participants because it is when British children leave primary school and enter secondary school. The study assessed seven forms of victimization: maltreatment, neglect, sexual victimization, family violence, peer/sibling victimization, cybervictimization, and crime victimization. Like childhood victimization, exposure to each form of victimization was coded for severity on a 3-point scale (Table 2).
Table 2. Associations between adolescent victimization (age 12–18 years) and young adult loneliness (age 18 years)
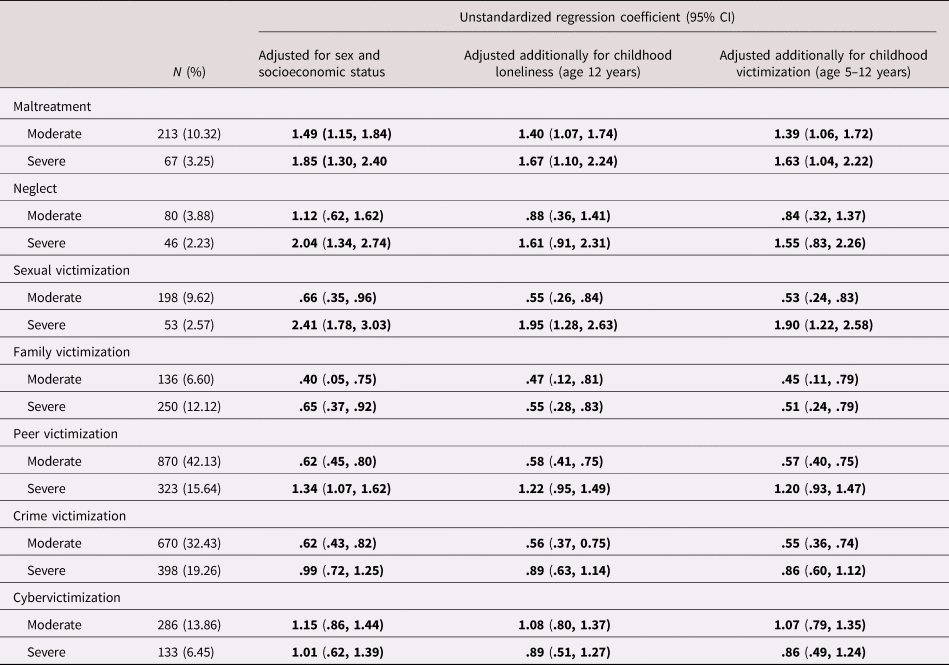
N = Number; CI = Confidence interval. All analyses are adjusted for sex and socioeconomic status. Associations shown in bold are significant using the Benjamini–Hochberg procedure with a false discovery rate of .05.
Polyvictimization refers to the experience of multiple victimizations of different types, and it is a more powerful predictor of adverse outcomes than any particular exposure (Finkelhor, Ormrod, & Turner, Reference Finkelhor, Ormrod and Turner2007). A 3-level measure of polyvictimization was derived for both childhood and adolescence, based on the number of different forms of severe victimization present: none (0), one (1), and two or more (2).
Detailed descriptions of the victimization assessments have been published previously (Danese et al., Reference Danese, Moffitt, Arseneault, Bleiberg, Dinardo, Gandelman and Caspi2017; Fisher et al., Reference Fisher, Caspi, Moffitt, Wertz, Gray, Newbury and Arseneault2015), and are provided in the Supplementary Materials.
Loneliness
A measure of loneliness in childhood was derived using three items from the Children's Depression Inventory (CDI; Kovacs, Reference Kovacs1992), completed when participants were aged 12 years. Each item was presented as a set of three statements, and participants were instructed to select the statement that described them best: (a) “I do not feel alone,” “I feel alone many times,” or “I feel alone all the time”; (b) “I have plenty of friends,” “I have some friends but I wish I had more,” or “I do not have any friends”; and (c) “Nobody really loves me,” “I am not sure if anybody loves me,” “I am sure that somebody loves me.” Although drawn from an instrument designed to assess depression, these particular items are very similar in content to items used in the Children's Loneliness Scale (CLS), which is considered the gold standard for assessing loneliness in children (Maes, Van den Noortgate, Vanhalst, Beyers, & Goossenss, Reference Maes, Van den Noortgate, Vanhalst, Beyers and Goossenss2017). Items were coded 0 to 2 and summed to produce a scale from 0–6 (M = .48; SD = .86, α = .48).
Loneliness in adulthood was assessed at age 18 years using four items from the UCLA Loneliness Scale, Version 3 (Russell, Reference Russell1996): “How often do you feel that you lack companionship?” “How often do you feel left out?” “How often do you feel isolated from others?” and “How often do you feel alone?” A very similar short form of the UCLA scale has previously been developed for use in large-scale surveys, and correlates strongly with the full 20-item version (Hughes, Waite, Hawkley, & Cacioppo, Reference Hughes, Waite, Hawkley and Cacioppo2004). The scale was administered as part of a computer-based self-complete questionnaire. The items were rated 0 (“hardly ever”), (1) (“some of the time”), or (2) (“often”). Items were summed to produce a total loneliness score from 0–8 (M = 1.57, SD = 1.94, α = .83). The correlation between loneliness measured at age 12 and at age 18 was r = .25.
Covariates
Because the items used in the age-12 loneliness measure originated from a scale used to measure depression, and because loneliness and depression are highly correlated in general (Matthews et al., Reference Matthews, Danese, Wertz, Odgers, Ambler, Moffitt and Arseneault2016), the remaining items of the CDI were summed to produce a depressive symptom scale, which was entered as a covariate with childhood loneliness to account for the shared variance between them. Symptoms of anxiety at age 12 were assessed using the Multidimensional Anxiety Scale for Children (March, Reference March1997). At age 18, symptoms of depression and anxiety were assessed via a structured clinical interview based on Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria (American Psychiatric Association, 1994). All analyses were adjusted for sex and for family socioeconomic status, measured via a standardized composite of income, education, and occupation.
Data analysis
All analyses were conducted in Stata Version 15 (StataCorp, 2017). First, in order to ascertain whether the number of victimization exposures was associated with loneliness in a dose–response manner, we tested associations between polyvictimization and loneliness. These associations were examined in childhood (age 5–12 victimization and age-12 loneliness), in adolescence (age 12–18 victimization and age-18 loneliness), and from childhood to young adulthood (age 5–12 victimization and age-18 loneliness). We also tested for a graded association between re-victimization (exposure in both childhood and adolescence) and loneliness in young adulthood.
Second, we tested childhood associations between individual forms of victimization across ages 5 to 12 and loneliness at age 12. Due to the high co-occurrence between loneliness and depression and anxiety (Matthews et al., Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor, Kepa and Arseneault2019), we further controlled for childhood symptoms of these mental health problems. Third, to test whether discordance in victimization within twin pairs was associated with differences in loneliness, we applied fixed-effects models to the data, thus controlling for familial confounds. We then repeated this analysis using MZ twin pairs only, thereby controlling completely for genetic variation between twins in a pair.
Third, we tested associations between adolescent victimization across ages 12–18 and loneliness at age 18. To investigate whether these associations were explained by pre-existing loneliness, we first tested whether childhood loneliness was associated with greater risk of adolescent victimization, and then included childhood loneliness as a covariate in the associations between adolescent victimization and young adult loneliness. Next, to determine whether these associations were explained by the continuity of victimization originating earlier in life, we tested a further model additionally controlling for prior exposure to any severe victimization in childhood. Further, we conducted sensitivity analyses, in which age-18 depression and anxiety were controlled for. We then applied fixed-effects models to the data, first in the whole sample and then in MZ twins only, to test whether the significant associations were independent of shared environmental and genetic confounds.
Fourth, we tested longitudinal associations between childhood victimization and age-18 loneliness. In order to test whether victimization predicted increases in loneliness over time, we then added age-12 loneliness as a covariate after the initial bivariate associations were estimated. Next, to test whether childhood victimization continued to predict loneliness regardless of whether victimization was still ongoing, we controlled for exposure to any victimization during adolescence. Significant associations were further subjected to controls for age-18 depression and anxiety. We also used fixed-effects models to control for the effects of unmeasured familial confounds.
Participants in this study were pairs of same-sex twins, and therefore each family contained data for two individuals, resulting in non-independent observations. To correct for this, we used tests based on the Huber–White or sandwich variance (Williams, Reference Williams2000), which adjusts the estimated standard errors to account for the dependence in the data.
Post hoc analyses
We conducted two additional sets of analyses to address questions arising from the main results. First, we entered childhood social isolation between ages 5–12 as a covariate with childhood bullying, to test whether the association between bullying and loneliness was explained by victimized children being isolated by their peers. The childhood social isolation scale was based on mothers’ and teachers’ reports of children's peer rejection and social withdrawal, using items drawn from the Children's Behaviour Checklist and Teacher Report Form (Achenbach, Reference Achenbach1991a, Reference Achenbach1991b). Full details of the measure are published elsewhere (Matthews et al., Reference Matthews, Danese, Wertz, Ambler, Kelly, Diver and Arseneault2015). This analysis was initially conducted with loneliness at age 12 as the dependent variable, and this was then repeated for loneliness at age 18. Second, we entered problematic technology use at age 18 as a covariate with adolescent cybervictimization, to test whether the association between this form of victimization and age-18 loneliness was explained by excessive time spent online. Problematic technology use was measured using an adapted version of the Compulsive Internet Use Scale (Meerkerk, Van Den Eijnden, Vermulst, & Garretsen, Reference Meerkerk, Van Den Eijnden, Vermulst and Garretsen2009).
A breakdown of the research questions and variables used in each analysis is provided in Supplementary Table S1.
Results
Cumulative and enduring effects of polyvictimization
Individuals who were exposed to one form of severe victimization were lonelier on average than those not exposed, and individuals exposed to multiple forms of severe victimization were more lonely compared to those exposed to just one form, or none at all (Figure 1). This pattern was observed in childhood (B = .54; 95% CI = .31, .77), in adolescence (B = 1.25; 95% CI = .98, 1.53), and from childhood to adolescence (B = .73, 95% CI = .31, 1.15). Furthermore, individuals who were exposed to severe victimization in both childhood and adolescence were lonelier at age 18 years than individuals who were victimized in just one of these time periods, or never (B = 1.14; 95% CI = .83, 1.45).
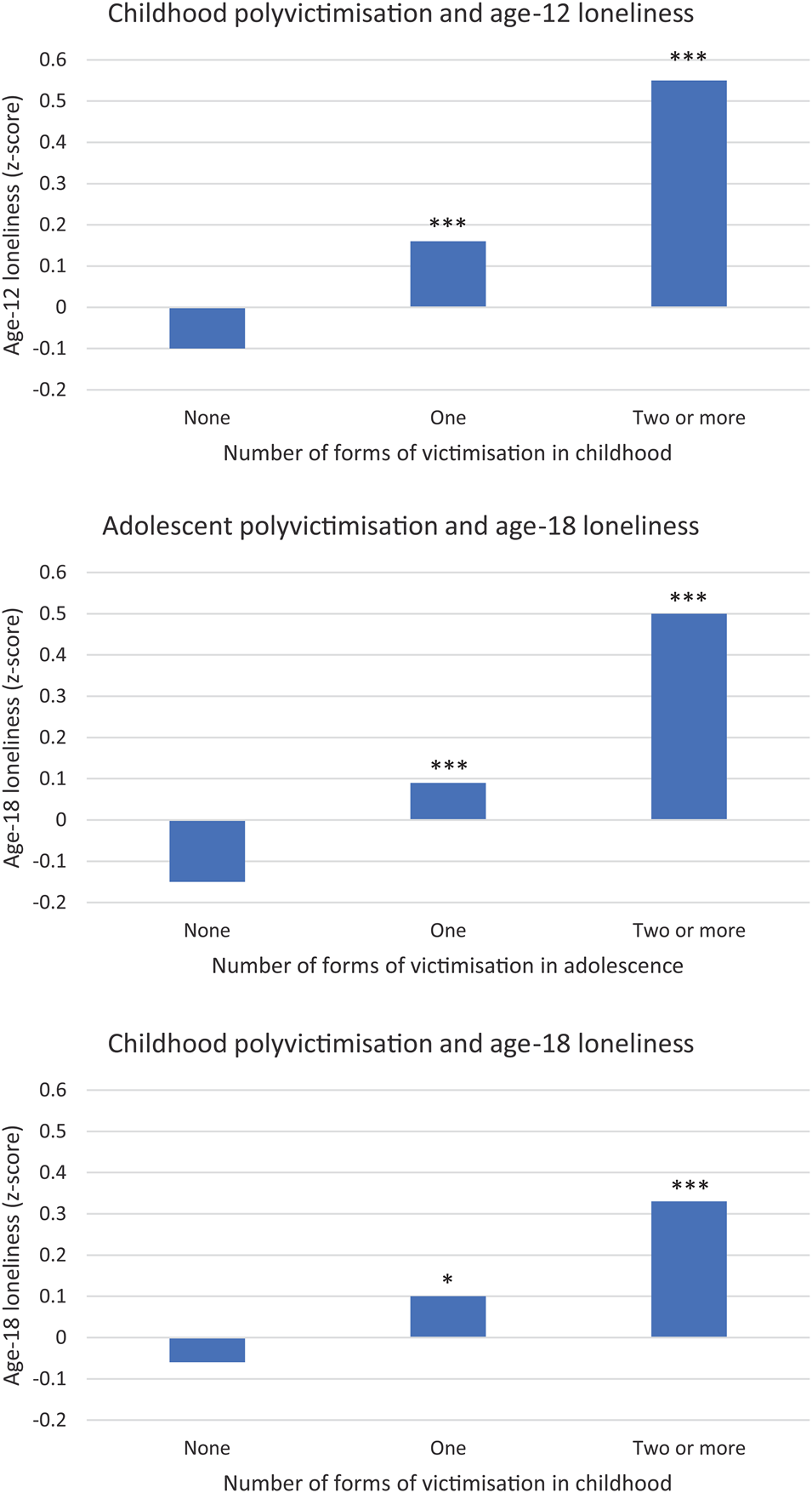
Figure 1. Mean (z scored) levels of loneliness according to the number of forms of victimization experienced. *p < .05 ***p < .001
Associations between victimization and loneliness in childhood
In bivariate regression models, multiple forms of victimization between 5–12 years were associated with loneliness at age 12 (Table 1). However, when concurrent depression and anxiety at age 12 years were controlled for, only bullying remained independently associated with loneliness (occasional bullying: B = .11; 95% CI = .05, .17; frequent bullying: B = .24; 95% CI = .09, .39). When social isolation between 5–12 years was controlled for in a post hoc analysis, childhood bullying remained associated with loneliness at age 12 (occasional: B = .18, 95% CI = .11, .26; frequent B = .67; 95% CI = .46, .87).
A fixed effects model using the whole sample (MZ and DZ twins together) revealed that bullying victimization was associated with within-family differences in loneliness, indicating an association independent of shared environmental influences (occasional bullying: B = .25; 95% CI = .12, .38; frequent bullying: B = .76; 95% CI = .47, 1.05). When the sample was restricted to MZ twins only, thereby holding genetic influences constant also, the association remained significant (occasional: B = .19; 95% CI = .01, .37; frequent: B = .71; 95% CI = .30, 1.12). Thus, among genetically-identical twin pairs discordant for bullying victimization, the twins who were bullied were lonelier on average than their non-bullied co-twins. Within-family analyses could not be conducted for physical neglect or emotional abuse/neglect due to low discordance for these exposures among MZ twins (Supplementary Table S2).
Associations between adolescent victimization and loneliness in young adulthood
All forms of adolescent victimization were associated with greater feelings of loneliness at age 18 years (Table 2). The strongest associations were for severe maltreatment, sexual victimization, and neglect. Adolescent victimization was also predicted by childhood loneliness (Table 3). Nonetheless, all associations between adolescent victimization and age-18 loneliness remained significant after controlling for childhood loneliness, and for prior victimization in childhood (Table 2). These associations were also robust to controls for the concurrent presence of any other form of severe victimization, and for depression and anxiety symptoms, with the exception of family victimization and moderate sexual victimization which became nonsignificant (Table 4).
Table 3. Associations between childhood loneliness (age 12 years) and adolescent victimization (age 12–18 years)
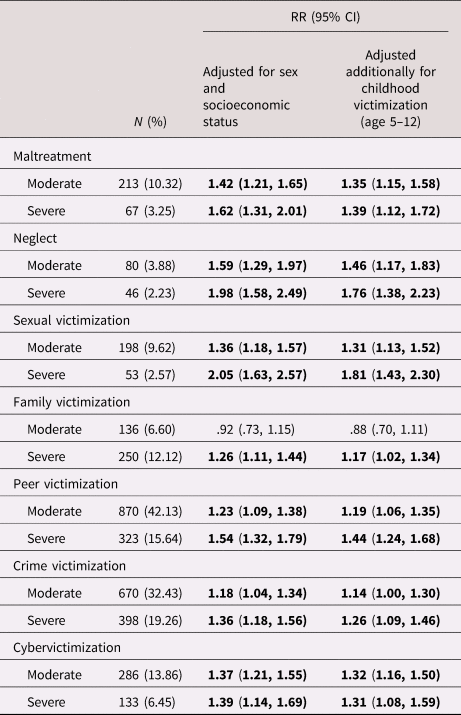
N = Number; CI = Confidence interval. RR = Relative risk ratio. All associations adjusted for sex and socioeconomic status. Associations shown in bold are significant using the Benjamini–Hochberg procedure with a false discovery rate of .05.
Table 4. Associations between adolescent victimization (age 12–18 years) and young adult loneliness (age 18 years), adjusting for confounds
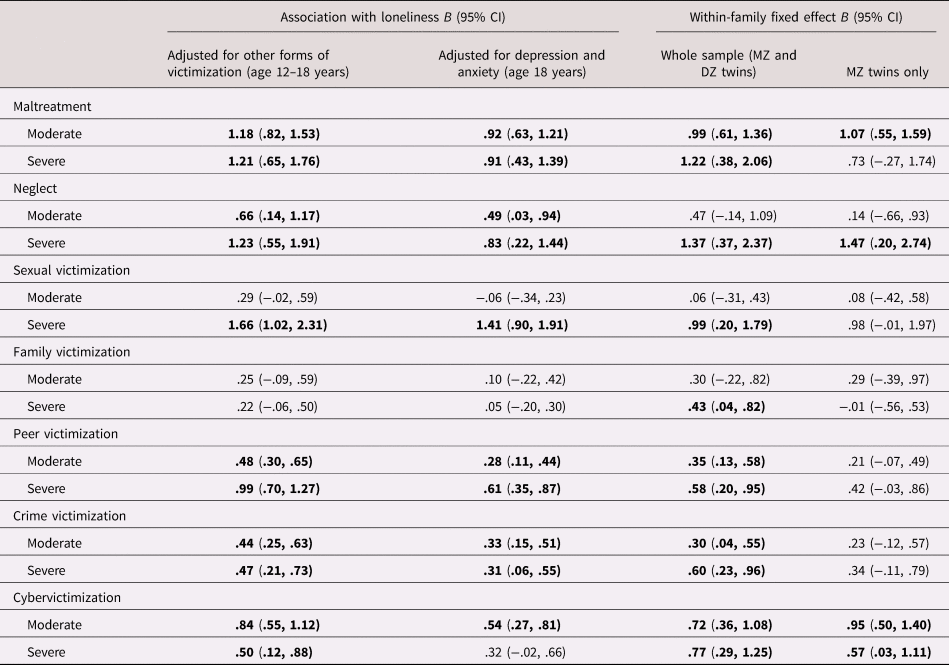
B = Unstandardized regression coefficient; CI = Confidence interval; MZ = monozygotic; DZ = dizygotic. All analyses are adjusted for sex and socioeconomic status. Associations shown in bold are significant using the Benjamini–Hochberg procedure with a false discovery rate of .05.
In the whole sample, the within-family fixed effect was significant for all forms of victimization, indicating that victimization was associated with differences in loneliness independently of shared environmental influences (Table 4). However, when the sample was restricted to MZ twins, only maltreatment, neglect and cybervictimization remained significantly associated with loneliness. This indicates that associations between the other forms of adolescent victimization and loneliness are largely explained by familial influences, both genetic and environmental.
As a post hoc analysis, the association between cybervictimization and loneliness was tested while controlling for problematic technology use, to test whether the association was explained by excessive time spent online. The inclusion of this covariate did not substantively attenuate the association (moderate: B = .93; 95% CI = .65, 1.21; severe: B = .85; 95% CI = .46, 1.23).
Longitudinal associations between childhood victimization and age-18 loneliness
Of the four forms of childhood victimization examined, severe physical/sexual abuse and occasional and frequent bullying up to age 12 years predicted feelings of loneliness at age 18 (Table 5). The strongest effect was for frequent bullying victimization. These associations were not explained by pre-existing loneliness in childhood. After controlling for ongoing victimization during adolescence, only bullying remained significantly associated with loneliness. This association was robust to controls for depression and anxiety at age 18 (occasional bullying: B = .28; 95% CI = .11, .46; frequent bullying: B = .82; 95% CI = .49, 1.14), and for childhood social isolation (occasional: B = .41, 95% CI = .21, .60; frequent: B = .90; 95% CI = .50, 1.31).
Table 5. Associations between childhood victimization (age 5–12 years) and young adult loneliness (age 18 years)
B = Unstandardized regression coefficient; N = Number; CI = Confidence interval. All analyses are adjusted for sex and socioeconomic status. Associations shown in bold are significant using the Benjamini–Hochberg procedure with a false discovery rate of .05.
In fixed effect models, frequent childhood bullying victimization predicted within-twin pair differences in age-18 loneliness in the whole sample (B = .56; 95% CI = .02, 1.10), indicating an association independent of family-wide environmental influences. However, this effect became nonsignificant when the sample was restricted to MZ twins (B = −.36; 95% CI = −1.05, .33), indicating genetic mediation of the remaining association between childhood bullying victimization and age-18 loneliness.
Discussion
This study builds on the existing literature by using a longitudinal twin study design to advance hypotheses about the developmental associations between victimization and loneliness in young people. Diverse forms of victimization in childhood and adolescence were shown to co-occur with elevated feelings of loneliness, and the graded effects observed for polyvictimization suggest a cumulative association, with higher levels of loneliness being reported in the presence of multiple forms of victimization. Moreover, lonely children were at increased risk of experiencing new instances of victimization during adolescence, over and above prior victimization exposures. However, to the extent that victimized children and adolescents felt lonely as adults, this was partly explained by the presence of co-occurring mental health problems, and by genetic influences that simultaneously contribute to risk for victimization and for loneliness.
Of the four forms of childhood victimization investigated in this study, bullying was the most common, and emerged as the strongest correlate of loneliness at age 12. It was the only form of victimization to be associated with loneliness irrespective of concurrent psychopathology, and was also independent of familial confounding. In late childhood and early adolescence, feelings of loneliness are related strongly to an unfulfilled need to be accepted by peers (Qualter et al., Reference Qualter, Vanhalt, Harris, Van Roekel, Lodder, Bangee and Verhagen2015). Bullying by peers constitutes a clear frustration of this need. Indeed, social exclusion is itself a common relational bullying tactic (Wolke, Woods, Bloomfield, & Karstadt, Reference Wolke, Woods, Bloomfield and Karstadt2000). This may partly explain why bullying was more strongly associated with loneliness compared to other forms of victimization. However, social isolation did not fully explain this association, suggesting that bullying could have implications for loneliness over and above relegating children to the periphery of the peer group.
Loneliness is generally conceptualized as arising from a perceived incongruence between an individual's desired and actual social relationships (Peplau & Perlman, Reference Peplau, Perlman, Peplau and Perlman1982). For bullied children in school or other group settings, being acutely aware of the disparity between their own troubled peer relationships and the relatively positive and normative relationships enjoyed by their contemporaries in the same environment could elicit an acute sense of injustice and a perception of oneself as an outsider. Feeling that one has no one to turn to for support could further compound feelings of isolation and helplessness, as victims often believe that reporting the bullying (for example, to a teacher) is not a viable option (Berguno, Leroux, McAinsh, & Shaikh, Reference Berguno, Leroux, McAinsh and Shaikh2004). Other potential mechanisms through which bullying could increase vulnerability to loneliness include diminished self-esteem, social anxiety, and elevated sensitivity to social rejection (Iffland, Sansen, Catani, & Neuner, Reference Iffland, Sansen, Catani and Neuner2014; Pavri, Reference Pavri2015; Zimmer-Gembeck, Trevaskis, Nesdale, & Downey, Reference Zimmer-Gembeck, Trevaskis, Nesdale and Downey2014).
Bullying was also the only form of childhood victimization that foreshadowed greater feelings of loneliness in adulthood, even when victimization was no longer ongoing. However, the within-family analyses did not support a causal pathway from childhood bullying to adult loneliness, instead pointing to common familial influences underlying the two, including genetic differences. Thus, although bullying is associated with loneliness in childhood via environmental pathways, the more long-term association between childhood bullying and young adult loneliness is largely mediated by genetic mechanisms. This finding mirrors other research on discordant twins, showing that while bullying predicts mental health problems longitudinally, the environmental component of this association, though present at baseline, diminishes over time, with genetic influences largely explaining outcomes after 5 years (Singham et al., Reference Singham, Viding, Schoeler, Arseneault, Ronald, Cecil and Pingault2016). One possibility is that children initially feel lonely as a result of being bullied and genetic influences shape the recovery trajectory, whereby only those children with a genetic vulnerability continue to feel lonely over time.
Children exposed to physical abuse and emotional abuse/neglect were lonelier at age 12 only if they also exhibited symptoms of depression and anxiety. As loneliness frequently co-occurs with these mental health problems, this constitutes a subgroup of substantial size. Nonetheless, it indicates that children exposed to this form of victimization do not report loneliness in the absence of emotional problems. Previous research in this cohort has also shown that neither parental antisocial behavior nor witnessing domestic violence in early childhood were associated with feelings of loneliness in adulthood (Matthews et al., Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor, Kepa and Arseneault2019). Thus, certain experiences in the childhood home environment which have powerful implications for emotional and behavioral development appear to be less applicable to this particular outcome. Instead, victimization within the family home seems to be more relevant for loneliness if experienced later in development: maltreatment and neglect during adolescence emerged as significant correlates of young adult loneliness, independently of covariates, whereas physical abuse during childhood only predicted loneliness if victimization was ongoing during adolescence. Childhood maltreatment may nonetheless interact with loneliness to affect other outcomes: for example, previous findings in this cohort show that the association between loneliness and sleep impairments is exacerbated among individuals with a history of physical maltreatment (Matthews et al., Reference Matthews, Danese, Gregory, Caspi, Moffitt and Arseneault2017).
Cybervictimization co-occurs with offline victimization more often than not, with the latter accounting for a larger proportion of variance in mental health problems such as depression and anxiety (Przybylski & Bowes, Reference Przybylski and Bowes2017). Despite this, both peer and cybervictimization in adolescence were independently associated with young adult loneliness. However, of the two, only cybervictimization survived controls for familial confounds. It is unclear what distinct features of cybervictimization may differentiate it from “traditional” peer victimization in this way. It was hypothesized that cybervictimization could be a proxy for compulsive or problematic internet use, which has been shown to be associated with loneliness (Matthews et al., Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor, Kepa and Arseneault2019; Nowland, Necka, & Cacioppo, Reference Nowland, Necka and Cacioppo2018) and could increase the probability of encountering hostile communications online. However, problematic technology use did not explain the association in this sample, indicating that the experience of this type of victimization merits further exploration. Meanwhile, the finding that an environmental effect for peer victimization was only detected in childhood and not in adolescence suggests again that the effects of victimization on loneliness may vary according to the developmental stage in which it is experienced.
That some of the significant associations between victimization and loneliness were explained by genetic mechanisms raises the question of which heritable traits could underlie these associations. Depression and anxiety, which were included as covariates in this study as they are known correlates of both victimization and loneliness, may partly account for the heritable component of these phenotypes (Arseneault, Bowes, & Shakoor, Reference Arseneault, Bowes and Shakoor2010; Matthews et al., Reference Matthews, Danese, Wertz, Odgers, Ambler, Moffitt and Arseneault2016). However, most associations survived controls for these confounds. Attachment styles or social cognitive skills may be plausible candidates that merit investigation. Furthermore, analysis of genome-wide data and polygenic risk scores may offer promise in future research of disentangling the genetic overlap between victimization and loneliness.
Limitations
Our findings should be considered in light of some limitations. It should be noted that although data on bullying were collected prospectively, the upper limit of the reporting period (age 12 years) coincided with the assessment of childhood loneliness. The association between these measures is therefore based partly on cross-sectional data and does not convey information about its direction. The longitudinal associations from childhood bullying to adult loneliness, and from childhood loneliness to adolescent peer victimization, are suggestive of a bidirectional association. However, bullying and peer victimization are not synonymous terms; bullying being a specific form of peer victimization that is repeated and involves a power imbalance in favor of the perpetrator (Arseneault, Reference Arseneault2018). Testing for a reciprocal association between bullying and loneliness would require repeated measures of both constructs using consistent measures.
It was not possible to examine physical abuse and sexual abuse separately in childhood, due to small group sizes for sexual abuse (minor: N = 17; severe: N = 16). The issue of power also applies to discordant twin analyses, as the level of discordance within twin pairs, particularly for childhood victimization, is low (Jaffee, Reference Jaffee2017). For example, there were no MZ pairs in this sample who were discordant for severe childhood physical neglect (Supplementary Table S2). In the case of adolescent victimization, there was greater discordance for most forms of victimization (Supplementary Table S3). Nonetheless, the halving of sample size when restricting analyses only to MZ twins has further implications for the precision of model estimates (Boardman & Fletcher, Reference Boardman and Fletcher2015).
The internal consistency of the childhood loneliness measure was modest. One potential explanation for this is that loneliness is a multidimensional construct (Hawkley, Browne, & Cacioppo, Reference Hawkley, Browne and Cacioppo2005), and each of the items maps onto a specific manifestation of loneliness: lack of friends, not being loved, and the internal state of feeling “alone.” The three would not always co-occur within the same individual, as they apply to different domains of life (e.g. school and peer group vs. home and family). Nonetheless, each one fits conceptually to the definition of loneliness as a perception that one's relationships with others are deficient in some way.
By definition, all participants in this sample had a sibling of the same age and sex (and, in more than half of cases, the same genome). The extent to which this could be protective against loneliness is not clear. Conversely, there may be unique aspects of being a twin that could contribute to loneliness, such as being treated as a pair rather than as individuals with separate identities, or being left out by peers due to an assumption that twins can rely on each other for company. The experience of loneliness may therefore be different in some respects for twins compared to singletons or non-twin sibling pairs. However, the number of individuals in this sample who reported feelings of loneliness “some of the time” or “often” at age 18 years are in line with those found in other studies of adolescents and young adults in the UK general population (Office for National Statistics, 2018).
Implications
While these data do not support a causal effect of childhood bullying on loneliness that endures into the adult years, this does not mean that victims should be considered “out of the woods” if the bullying ceases. To the contrary, if being a victim of bullying partially reflects a genetic vulnerability to loneliness, an implication of this is that victims remain at risk of becoming lonely later in life even if they are no longer being victimized. Early adulthood is a peak age for loneliness (Luhmann & Hawkley, Reference Luhmann and Hawkley2016), and individuals with a history of bullying victimization in childhood may require particular support during the transition from adolescence to adult life. Moreover, bullying should remain a concern for long-term outcomes more generally, as it has been shown to predict mental health and psychosocial problems well into mid-life (Takizawa, Maughan, & Arseneault, Reference Takizawa, Maughan and Arseneault2014). The findings of the present study do not detract from the importance of interventions to reduce bullying and support victims in order to prevent adverse outcomes later in life.
Additionally, the findings highlight that abuse and neglect, though extensively studied as childhood risk factors, could have particular implications for loneliness when they are experienced in adolescence rather than in childhood. Even though adolescents increasingly spend more time outside of the family home, thereby exposing them to a more diverse range of environmental risks, victimization within the family home appears to be particularly important for loneliness at this stage of life. Conversely, while peer victimization has strong implications for mental health in adolescence (Troop-Gordon, Reference Troop-Gordon2017), it appears to be most relevant to loneliness when experienced in childhood. This highlights that the experience of loneliness, and its antecedents, are dynamic across development (Qualter et al., Reference Qualter, Vanhalt, Harris, Van Roekel, Lodder, Bangee and Verhagen2015), and that strategies to support victimized and lonely individuals should reflect this.
Supplementary Material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579420001005.
Acknowledgments
The E-Risk Study is funded by the Medical Research Council (UKMRC grant G1002190). Additional support was provided by National Institute of Child Health and Human Development (grant HD077482) and by the Jacobs Foundation. Timothy Matthews is a British Academy Postdoctoral Fellow. Helen L. Fisher is supported by an MQ Fellows Award (MQ14F40). Louise Arseneault is the Mental Health Leadership Fellow for the UK Economic and Social Research Council. The authors are grateful to the Study members and their families for their participation. Our thanks to CACI, Inc., and to members of the E-Risk team for their dedication, hard work, and insights.
Conflicts of Interest
None.









 Open access
Open access