


The world is not on track to end malnutrition and poverty by 2030, as set out in the Sustainable Development Goals in 2016(1). Having made considerable progress in reducing the global prevalence of hunger, between 2005 where it stood at 12·3 %, to 2014 where it plateaued just under 8 % until 2018, we are now experiencing a steep increase with a prediction that the prevalence could now be as high as 10·5 %(1). Consequently, with eight years remaining, the world is moving in the wrong direction, with an estimated 702–828 million people in the world facing hunger. More than half of those undernourished live in Asia, with one-third in Africa(1).
Alongside undernutrition, there is also concern about a global increase in overnutrition, the so-called double burden of malnutrition, often occurring in the same communities or even families and associated with poverty, lack of access to education, and food insecurity. Multiple factors are contributing to the recent increase in prevalence of malnutrition, including climate extremes, conflict, the COVID-19 pandemic, and their contribution to the economic shock currently experienced globally. Independently, and in combination, these factors have negatively impacted the global agri-food systems, driving up inequalities and challenging the quantity and quality of food that people can access, resulting in an increased reliance on low-cost high calorie staples, with low micronutrient density.
Micronutrient deficiency, also referred to as ‘hidden hunger’, is estimated to effect two billion people, or one in four worldwide(Reference von Grebmer, Saltzman and Birol2). Deficiencies in vitamin A, folate, zinc, iodine and iron are of particular concern in women and children(Reference Black, Allen and Bhutta3). A recent study that combined micronutrient status data from 22 nationally representative population-based surveys from 20 countries, indicated that the global prevalence of micronutrient deficiency is likely to be much higher than previously thought, with deficiency of at least one micronutrient estimated to affect 56 % in preschool children and 69 % among non-pregnant women of reproductive age (WRA)(Reference Stevens, Beal and Mbuya4). South Asia, East Asia and Sub-Saharan Africa and the Pacific were the worst affected areas. However, the study also highlighted the high prevalence of micronutrient deficiencies in high income countries, for example the UK and USA where 43 % and 32 % of WRA respectively have at least one ‘core’, micronutrient deficiency (iron, zinc or folate).
Supplementation is effective for targeted interventions, but not practical on a population scale due to the high recurring costs and logistical distribution challenges. The three primary scalable food-based strategies to increase micronutrient intake are: dietary diversification, food fortification and food biofortification(Reference Lowe5). While dietary diversification, meaning making diverse diets available and affordable for all, would be the ideal long-term goal, this feels very far out of reach against the backdrop of challenges and current trends in global food insecurity and malnutrition described above. It would require radical transformation of the agri-food system to achieve a reduction in inequalities on a global scale(6), driven by international political commitment, and sustained by commercial drivers. In the short-medium term, food fortification and biofortification offer solutions to hidden hunger that can be scaled to population levels.
The intention of this review is not to provide a comprehensive review of food fortification and biofortification programmes; this has been done extensively for a number of key micronutrients(Reference Hall and King7–Reference Kaur, Agarwal and Sabharwal10). The aim is to provide a brief overview of fortification and biofortification strategies to address micronutrient deficiencies, then to explore the strengths and limitations of these two strategies using the example of Pakistan as a specific context where fortification and biofortification initiatives were launched independently, but in parallel in 2016. The food fortification programme (FFP), supported by UK Aid, was designed to address the high prevalence of vitamin A, iron and zinc deficiency, particularly in WRA and children(11). An evaluation at the 5-year end point of the FFP was undertaken by an independent international consortium(12). The biofortification initiative began with the release of the first biofortified wheat variety in Pakistan, Zincol-2016, supported through the HarvestPlus programme in collaboration with the Pakistan National Agriculture Research Centre. The BiZiFED research programme, supported by UKRI Global Challenges Research Fund(13,14) , was the first study in Pakistan to explore the performance of Zincol-2016 under a variety of ‘real-world’ soil and agronomic conditions. Outcome measures explored the health impact of Zincol-2016 in a low resource community where the prevalence of zinc deficiency was high, and the enablers and barriers to scale up from the perspective of the producers and consumers.
Food fortification
Fortification involves the addition of a micronutrient or micronutrients to food during food processing, or at the point of use, such as micronutrient powders that can be applied at home directly to food prior to consumption(Reference Olson, Gavin-Smith and Ferraboschi15). It can be mandatory or voluntary and should be regulated to avoid excessive exposure to potentially toxic levels of minerals of vitamins through multiple vehicles. It can be employed to target nutrient deficiencies on a population scale, so-called ‘mass’ or ‘universal fortification’, or used to target specific vulnerable population groups, such as children or pregnant women(16). The key to success for any fortification programme is the choice of food vehicle, which should be consumed year-round without seasonal variation. The food vehicle must facilitate scale (i.e. high proportion of the population consuming that food in fortifiable form) and equitable access (i.e. that all communities, particularly disadvantaged groups, have access to the fortifiable form)(12). Another important factor in successful scale-up is the ability to monitor the fortification process and to control the quality of the fortified product to ensure that it meets the target micronutrient level and prevent excessive intake. This requires technical infrastructure and effective monitoring and enforcement policies. This is made viable when the fortification takes place in a limited number of centralized food processing facilities, serving the majority of the supply for the population. The pathway to the scale-up of food fortification is illustrated in Fig. 1. Many of the steps are also common to the scale-up of biofortification.

Fig. 1 Pathway for scale-up of food fortification and biofortification. Abbreviation: NGO, Non-government Organization(46).
One of the global success stories has been salt iodization which began in Switzerland in 1922, a country where iodine deficiency was prevalent, resulting in high rates of iodine deficiency disorders (e.g. endemic goitre and cretinism)(Reference Bürgi, Supersaxo and Selz17). A century later, 88 % of the global population uses iodized salt. Salt is an ideal food fortification vehicle in the case of iodine because it is consumed by populations in stable amounts throughout the year and is relatively inexpensive to fortify, thus, allowing a global reach, and reducing barriers to access even by the poorest communities. Currently, 124 countries have legislation of mandatory salt iodization, and 21 have legislation allowing voluntary iodization(18). This has dramatically reduced the global prevalence of iodine deficiency related disorders which include goitre, cretinism, intellectual impairment, and adverse obstetric outcomes(Reference Pearce and Zimmermann19).
Similarly, fortification of flour with iron, often in combination with zinc and B vitamins (particularly folic acid and B12), has significantly improved iron status and reduced anaemia in many countries(Reference Kaur, Agarwal and Sabharwal10,Reference Gera, Sachdev and Boy20) . A study designed to assess how the prevalence of anaemia in non-pregnant women was impacted in countries that had introduced mass fortification of wheat flour or wheat and maize flour, with countries that had never fortified, reported that after adjusting for human development index of the country, and malaria, each year of fortification was associated with a 2·4 % reduction in the odds of anaemia prevalence. Among countries that never fortified, no reduction in the odds of anaemia prevalence over time was observed(Reference Barkley, Wheeler and Pachon21).
Although inadequate zinc intake is estimated to affect 17·3 % of the global population(Reference Wessells and Brown22), the prevalence of zinc deficiency is rarely monitored in population surveys due to the lack of a sensitive and specific biomarker(Reference Hall and King7,Reference King23) . This also means that monitoring the impact of a zinc fortification programme on health outcomes relating to zinc deficiency is challenging. The clinical consequences of zinc deficiency include stunted growth in children, suboptimal immune function and increased risk of complications in pregnancy and childbirth(Reference King23). The most frequently used biomarker for assessing zinc status on a population scale is serum or plasma zinc concentration, although interpretation of the data may be confounded by the prevalence of concurrent inflammation(Reference McDonald, Suchdev and Krebs24). A Cochrane review of the adverse or beneficial effects of zinc fortification of staples foods reported that zinc fortified foods increased serum or plasma zinc concentration, compared to foods without added zinc, by a mean difference of 12·12 µmol/l. However, when food fortified with zinc plus other micronutrients was compared with food fortified with micronutrients but not zinc, there was no overall difference in serum or plasma zinc concentration, possibly due to nutrient interactions(Reference Shah, Sachdev and Gera25) but clearly illustrating the complexity of interpreting serum/plasma zinc concentration particularly when provided within a food matrix(Reference Hall26).
The most common food staples chosen for universal iron and zinc fortification programmes are cereals (wheat, maize, rice) used for flour or breakfast cereal products. Condiments, seasonings, flavoured beverages, and powdered or liquid milk have also been explored for more targeted approaches in population subgroups(Reference Adamo, Atashpaz and Germain27). For zinc and iron, the food matrix and meal composition can significantly impact the amount of mineral absorbed and retained (bioavailability) from the fortified food. Phytic acid, present in plant based foods, including cereals and grains, is one of the most potent inhibitors of zinc absorption, so must be considered when setting the optimal target fortification level(Reference Hall and King7).
Vitamin A is one of the four most prevalently deficient micronutrients worldwide, with a particularly high prevalence in sub-Saharan Africa and Southeast Asia. Vitamin A deficiency (VAD) results in night blindness due to the role of retinol in dark adaptation. In its most severe form, VAD may lead to a thickening and ulceration of the cornea, referred to as keratomalacia ultimately resulting in blindness. Children and pregnant women are the most susceptible to VAD, which in addition to the ocular effects, also increases susceptibility to common childhood infections and morbidity in children and increases risk of complications during pregnancy women(Reference Tanumihardjo, Russell and Stephensen28). VAD remains the leading cause of preventable blindness in children in low and middle income countries (LMICs)(Reference Xu, Shan and Lin29). As a fat-soluble vitamin, edible vegetable oils and fats (margarine) are common food vehicles for fortification. However dry forms coated with starch, gum or gelatine and an adhesive can be used in dry foods (sugar). A Cochrane review of the impact of fortification of staple foods on VAD identified a wide variety of food vehicles, including refined sugar, edible vegetable oils and fats, rice, wheat flour, maize flours and corn meals, condiments and seasonings, and powdered or liquid milk(Reference Hombali, Solon and Venkatesh9). Due to a concerted international commitment to eliminating VAD, through a combination of food fortification, supplementation and biofortification strategies, the global incidence of VAD has decreased by 44 % from 1990 to 2019(Reference Zhao, Liu and Zhang30). However, the burden of VAD remains high in regions with a low socio demographic index. Mandatory national vitamin A fortification programmes have been implemented in several countries including Guatemala, Venezuela, Zambia, Morocco, Philippines and Thailand(Reference Dary and Mora8,Reference Hombali, Solon and Venkatesh9) .
Food fortification programmes in Pakistan
In Pakistan, multiple micronutrient deficiencies are prevalent against a backdrop of widespread malnutrition and food insecurity. Nutrient deficiencies affect both urban and rural communities, and all regions and income groups, thus a population-based approach is warranted to address the scale of the challenge(12,31,32) .
Mandatory fortification of vegetable oil and ghee with vitamin A was introduced in 1965. But in 2011, the Pakistan National Nutrition Survey (NNS) reported that 46 % of pregnant women had VAD(31). Inadequate fortification that failed to meet the national standards was likely to be one of the contributing factors to the persistently high deficiency rates(12). A survey conducted in 2017 found that only 19 % of brands were adequately fortifying, and 69 % of other brands, not up to national standards(33). The NNS 2011(31) also reported that the prevalence of iron deficiency anaemia and zinc deficiency in non-pregnant women was 19·9 % and 41·6 % respectively. Vitamin D deficiency was also highly prevalent, affecting 66·8 % of non-pregnant women(31).
In 2016, a 5-year FFP was launched with the specific aim to reduce iron deficiency anaemia by 33 % and vitamin A deficiency by 25 % in women and children(34). The programme also included zinc, folate and vitamin D to address undernutrition particularly among the poorest women, girls and children under 5 years of age(12,34) . The ambitious 5-year programme was expected to reach 150 million people with fortified staples, one of the largest fortification programmes in the world.
Oil and ghee were chosen as the vehicle for vitamins A and D as these are inexpensive and widely used in meal preparation, thus having the potential for scale and equity. For iron, folate and zinc, wheat flour produced at large commercial roller mills was chosen as the vehicle. Wheat flour is used for making bread (roti, chapati, naan, paratha) which is consumed with every meal year-round, thus the most widely consumed staple and the ideal vehicle for fortification. The overarching approach employed was to increase the supply of fortified food products, increase demand and create an enabling environment for food fortification(12). This was achieved by providing technical assistance to government (local and provincial) and industry partners, and by engaging in advocacy targeted at policy makers and the public. The specific objectives are described in Text box 1.

Box. 1. Objectives of the food fortification programme(34)
The final evaluation at the end of the 5-year FFP highlighted the successes and limitations of the FFP within the Pakistan context(12). In terms of the oil/ghee fortification, mandatory fortification with vitamin A and D was already in place prior to the launch of the FFP. Many mills were already fortifying oil/ghee (albeit not always to an acceptable standard that meets the target vitamin concentrations), and consumer acceptance was strong, thus raising public awareness of the benefits of fortified oil/ghee was not a priority. Efforts were therefore focussed on improving fortification standards through improved monitoring and enforcement. One of the key challenges faced was the widespread availability of ‘loose’ (unpackaged), unrefined (not fortified) oil/ghee on the market at a reduced price to consumers. This was found to represent 28 % of the available oil/ghee, and most likely to be the oil purchased by low-income households. It was acknowledged that stricter enforcement of regulations around the production of illicit oil/ghee would have an economic impact the poorest. Nevertheless, the programme was successful in improving the fortification standards, and increasing the number of registered, participating mills, such that they reached adequate levels of vitamins A and D, and on track to achieve the target of for annual production of 2·5 million metric tonnes of fortified oil/ghee by 2021. Interviews at the end of the programme indicated that this improvement was due in part to the subsidy for the premix and testing kits that were provided to the mills during the FFP programme. It remains to be seen whether the momentum can be sustained as mills graduate from subsidization.
In contrast to oil and ghee, wheat flour fortification with iron, folate and zinc was undertaken on a voluntary basis. Therefore, millers and retailers required a strong public demand for the fortified product to make a business case for adopting the fortification strategy and increasing the supply. However, although this logic holds true where there is capacity for producers to create a price niche for high quality products in an open market, this does not meet one of the essential criteria for population-based fortification strategies, namely equity, since the poorest would not have access to these premium products. In addition, the government-controlled wheat market and flour price in Pakistan does not provide a strong commercial business case for voluntary fortification since the producer is unable to pass on the additional cost to consumer. Therefore, raising awareness for wheat flour fortification had little potential to change consumer or industry behaviour. One way to resolve this would be for the government to offset the cost of the premix and fortification process, however this ongoing cost would undermine the original goal of sustainability in the production of fortified wheat flour. Additionally, legislation for mandatory fortification of flour could be introduced. Within the Pakistan context, this is complex and time consuming due to the devolution of decision-making around health, food and agriculture to provincial governments, however some initial progress has been made towards achieving legislation in Sindh province which is home to 50 Million people, or 23 % of the Pakistani population.
Another challenge to the flour fortification programme was the decision to target the large commercial roller mills. This significantly undermined the scalability of flour fortification programme since only a proportion of wheat flour consumed in Pakistan is processed in these mills. It is estimated that industrial mills account for between 40 and 60 % of household wheat flour procurement in Pakistan(Reference Ansari, Mehmood and Gazdar35). The remaining proportion of household flour is derived from wheat grain that is retained for self-consumption by farmers or received as in-kind payment by farm labourers, and is milled in small local ‘chakkis’, of which there are many thousand in both urban and rural locations across the country(Reference Ansari, Mehmood and Gazdar35). In addition, the end of programme evaluation report highlighted that the focus on the technical aspects of producing fortified flour meant that there was a lack of complimentary activity and engagement with policy makers and stakeholders early-on in the programme. This meant that the essential ‘enabling environment’ to support the scale-up of the programme was not effectively created (Fig. 1). Although this was corrected post-mid-term, notably through engagement with the influential Pakistan Flour Mills Association, this was not sufficient to mitigate the impact of the lack of earlier political engagement on achieving the programme goals(12).
In 2020, the FFP suffered major setbacks linked to the COVID pandemic and an ongoing wheat shortage affecting prices. Despite these challenges, the FFP was successful in improving access to premix and the installation of micro feeders so that more mills are in a position to fortify going forward, should the incentive be there for them to do so. At the end of the programme, the target to provide 1·5 million metric tons of fortified wheat flour annually was not reached, and the proportion of the wheat flour that was fortified represented less than half of the wheat flour produced by the participating mills(12).
Biofortification
Biofortification is the enhancement of the nutrient content of a staple crop through plant breeding and/or agronomic techniques(Reference Saltzman, Birol and Bouis36). Plant breeding methods may involve the transfer of genes between species to introduce new, beneficial characteristics or traits such as enhanced nutrient content, or the reduction in an antinutrient concentration that limits the bioavailability of nutrients in a plant, such as phytate. This transgenic breeding technique is also referred to as genetic modification (GM). An early example of the use of this technique for nutrition purposes is ‘Golden Rice’ which is biofortified in vitamin A. The original work on Golden Rice was undertaken in the 1990s by Beyer and Potrykusby(Reference Ye, Al-Babili and Kloti37). They found that by introducing two genes to the rice DNA, a plant phytoene synthase and a bacterial phytoene desaturase, the pathway for the synthesis of β-carotene is switched on and consequently accumulates in the grain(Reference Burkhardt, Beyer and Wunn38). This early work resulted in rice that contained 1·6 ug/g carotenoids which is not sufficient to meet daily provitamin A requirements of the target population. Further refinement of the GM process resulted in a second generation of Golden Rice, capable of achieving carotenoid concentrations of 37 ug/g in the endosperm(Reference Al-Babili and Beyer39). Recent work has demonstrated that this second generation has potential to provide 89–113 % of the vitamin A requirement of children in Bangladesh(Reference Swamy, Samia and Boncodin40). However, concerns around the safety of GM crops have limited the global uptake. Currently, the Philippines is the only country that has approved the planting of Golden Rice(Reference Wu, Wesseler and Zilberman41).
Conventional breeding methods that have been used for thousands of years can also be used to select for desirable traits in food crops, including nutrient content alongside yield potential and disease resistance. In recent years there has been a rapid expansion in the number of micronutrient biofortified staple crop varieties that have been released to address micronutrient deficiencies around the world(Reference Lowe5). For example iron rich beans have been produced in Rwanda that have 72 % higher iron content than standard varieties, and have demonstrated improvement in indices of iron status in women after consuming for 4·5 months under controlled study conditions(Reference Haas, Luna and Lung’aho42).
Agronomic techniques, including the application of nutrient fertilizers to the soil or directly to foliage, can also be used to enhance the nutrient content of a staple crop, either as a standalone method or in combination with traditionally bred biofortified varieties to realize the nutrient accumulation potential of the crop without the limitation of low soil nutrient content(Reference Cakmak and Kutman43). Agronomic methods alone can result in highly significant increases in micronutrient content of a crop, particularly when the nutrient supply from the environment is limiting. For example in Malawi where due to local geology, soil selenium levels are very low, application of selenium fertilizer resulted in an increase of 150 % in the selenium content of maize, which translated into a significant increase in serum selenium concentration in WRA and school aged children(Reference Joy, Kalimbira and Sturgess44). Similarly, the enrichment of rice with zinc through application of zinc through the soil and/or foliage resulted in a net increase in zinc content of 52·2 % above control in the cooked product(Reference Saha, Chakraborty and Padhan45).
Once a biofortified crop variety has been developed, the steps to anchoring the variety in the food system and creating a self-sustaining supply are illustrated in Fig. 1. The key steps include (1) Research and development through breeding programmes for desired traits. It is also important to develop a robust system for tracing supply chains so that they can be certified as biofortified for consumer awareness and choice. Objective evidence from efficacy and effectively trials is valuable to support the scale-up campaigns and underpin policy development and implementation. (2) Scaling, meaning to create a demand for biofortified seed varieties amongst farmers and consumers, for example through media campaigns. This has more chance of success if it can be linked to local and national policies thus providing an enabling environment for the dissemination of information promoting the benefits of growing and consuming biofortified crops. Endorsement by influential and trusted community and religious leaders can also help to drive demand. (3) Mainstreaming, to anchor the biofortified stable within the food production system such that it becomes an accepted and consistent contribution to the staple supply chain. This can be achieved by building momentum through the research and development pipeline, to allow ongoing release of new biofortified varieties. The development of public-private partnerships to assist with the delivery of the supply chain, and engagement with food industry to incorporate biofortified staples into their products also helps to achieve the goal of mainstreaming(46). Scaling biofortified beans in Rwanda where up to 12 per-cent of national bean production derived from biofortified varieties, illustrates the successful implementation of supply chain multisectoral approaches(Reference Birol and Bouis47).
Biofortification in Pakistan
In 2016, the first zinc biofortified wheat variety for Pakistan, Zincol-2016, was released. The BiZiFED programme was launched in 2017 to evaluate the potential for zinc biofortified wheat address zinc deficiency in Pakistan on a population scale. The programme was comprised of two elements; an efficacy trial(Reference Lowe, Khan and Broadley48) conducted between 2017 and 2019, and an effectiveness trial(Reference Lowe, Zaman and Moran49) conducted between 2019 and 2021. The overarching research questions for two these trials are summarized in text box 2.

BiZiFED was the first research programme to study the impact of consuming zinc biofortified wheat on health outcomes in women, adolescent girls and children in Pakistan. It also sought to evaluate the performance of the biofortified crop under different soil conditions and agronomic management practices and explore the potential barriers and enablers for scale-up in terms of farmer and consumer acceptability.
For the efficacy study, biofortified wheat (Zincol-2016) and a standard wheat variety (Galaxy) that served as the control for the double blind, randomized, controlled cross-over trial, were grown on a single farm under carefully supervised conditions. Experimental field trials indicated that the zinc content of the Zincol-2016 grain was optimized when zinc fertilizer was applied to the soil during sowing, and also to the foliage when the seedhead started to form (i.e. booting stage)(Reference Zia, Ahmed and Bailey50). Analysis of the grain immediately prior to harvest revealed that the zinc concentration of the Zincol-2016 grain was more than double that of the Galaxy control, 49·3 ± 5·6 mg/kg compared with 22·3 ± 2·9 mg/kg respectively. Based on an average flour consumption of 224 g per day, this resulted in an estimated daily zinc intake for the study participants of 11 mg from wholemeal, or 5·5 mg from white, Zincol-2016 flour compared with 5 mg from wholemeal and 2·5 mg from white Galaxy flour(Reference Lowe, Zaman and Khan51). Encouragingly, similar grain zinc concentrations for Zincol-2016 were achieved when the biofortified wheat was grown by local farmers under ‘real-world conditions’ with some technical support from local collaborators, 45·3 ± 10·7 mg/kg(Reference Gupta, Zaman and Fatima52), although there was a high level of variability from 24·3 to 76·3 mg/kg.
The study failed to demonstrate a measurable impact of consuming the biofortified wheat for 6 months on anthropometric outcome measures in adolescent girls or children under 5 years old. However, there was some indication of an improvement in morbidity in both groups due to upper respiratory tract infections towards the end of the intervention period(Reference Gupta, Shahzad and Zaman53,Reference Gupta, Zaman and Fatima54) . As mentioned previously, current biomarkers lack the sensitivity to pick up small changes in dietary zinc intake, thus no change in plasma zinc concentration post-intervention was detected, however analysis of hair zinc concentration using a novel x-ray fluorescence technique did identify a significant increase in hair zinc levels in the adolescent girls consuming zinc biofortified flour for 6 months(Reference Frederickson, Fleming and Asael55).
Consumer acceptability was explored in focus group discussions with community members and elders living in the BiZiFED study location, which was a low resource community. Thematic analysis of the transcripts revealed an appreciation of the potential health benefits of biofortified flour, and despite concerns about a potentially higher price compared with standard flour, a willingness to pay a little extra for the health benefit was expressed(Reference Mahboob, Ohly and Joy56,Reference Mahboob, Ceballos-Rasgado and Moran57) . Furthermore, a survey of 418 farmers growing zincol-2016 in Punjab province was conducted 1 year after their participation in the BiZiFED trial(Reference Ceballos-Rasgado, Moran and Ander58). The survey was designed to explore the farmers experiences of growing Zincol-2016, and whether they chose to grow it again once the trial had ended. It revealed that 47 % of the farmers did retain some grain from the 2021 harvest to plant the following season, citing its yield, disease resistance, high quality of flour and nutritional benefit as the main drivers(Reference Ceballos-Rasgado, Moran and Ander58). Exploration of the barriers and enablers to scale up in focus group discussion with farmers in the northern province of Khyber Pakhtunkhwa supported the findings of the survey, with the flour quality and health benefits being key enablers. Barriers included additional production costs (e.g. zinc fertilizer) and external threats to the supply chain, such as the consequences of crop disease and severe climate events and major health crises as experienced in the recent COVID-19 pandemic.
Conclusions
Food fortification and biofortification both have potential to positively address micronutrient deficiencies on a population scale and are complementary strategies alongside dietary diversification and supplementation. They share several advantages over supplementation since neither require individual behaviour change, and both have the potential provide benefit to all members of society irrespective of socioeconomic status. The pathways to scale-up and mainstreaming of fortified foods and biofortified crops share many common elements (Fig. 1), however, context specific cultural, political, economic and behavioural factors can significantly impact the success or failure of a fortification or biofortification initiative.
This review explores the challenges faced by fortification and biofortification, initiated independently around the same time in Pakistan. The endline review of the FFP highlighted the contextual challenges relating to the fortification of wheat flour, in particular, the choice of food vehicle which should ensure that the key principles of equity and scale are preserved so that the fortified product reaches all and is affordable for all. This requires in-depth understanding of the consumption patterns, processing mechanisms and market forces. While this was mostly successful for oil/ghee fortification with vitamins A and D which benefited from the mandatory fortification legislation that was already in place, it was less so for wheat flour which was fortified on a voluntary basis. In the absence of enforced legislation, voluntary fortification relies on economic/market drivers for it to become self-sustaining. These conditions are not present in the Pakistan context where wheat price is controlled, therefore there is an ongoing need for government subsidies to mills to incentivize flour fortification, alongside investment in infrastructure for monitoring and quality control. Similarly, farmers involved in growing zinc biofortified wheat expressed the need for government subsidies to offset the cost of the fertilizers required to optimize the zinc content of the wheat grain.
The potential scalability of flour fortification is also compromised in the Pakistan context because only around half of the flour consumed is processed in registered roller mills, with the opportunity to add the premix. The rest is processed in the many local chakkis. In 2020, the World Food Program (WFP) in Pakistan undertook a pilot study designed to support ten chakkis to fortify the flour with micronutrients. The pilot involved training on fortification, compliance and monitoring alongside the provision of microfeeders, test kits for measuring micronutrient levels and the creation of quality assurance systems. The programme also provided support for registration with government bodies and public awareness campaigns The chakkis provided an opportunity for households to purchase the fortified flour or to have the micronutrient premix added to their own grain which they brought to the chakki for milling, for a small additional cost. WFP reported that the participating chakkis experienced a growth in their business as a result of participating in the pilot, with an increase in sales of fortified flour to existing customers, and new customers attracted by the offer of the fortified product(Reference Gie59). Within 1 year of participation in the pilot, the ten chakkis were fortifying 85 % of their flour and the pilot has now been expanded to include 50 chakkis, reaching over 2 million beneficiaries(Reference Gie59).
The early evaluation of biofortification of wheat presented in this review was on a relatively small scale, but still presents some valuable lessons. Demonstrating effectiveness of a biofortification intervention in a real-world (free-living) scenario is difficult to establish due to the range of soil conditions and agronomic methods that introduce variability in the level of target nutrient present in the staple crop, coupled with the numerous dietary factors and food preparation practices that may enhance or limit the absorption of the target nutrient. There is a need long-term studies to monitor impact on health outcomes over time. This, however, this is resource intensive and in the case of zinc requires further exploration of sensitive and reliable biomarkers of status.
An enabling environment, linked to policy and programmes is vital for the scale-up of both fortification and biofortification, and both require partnerships for delivery and participation in the food value chain. The endline report of the FFP highlighted the failure to place sufficient emphasis early in the programme on building alliances with government regulatory bodies and miller’s associations, which hindered the achievement of the flour fortification target.
Since the release of Zincol-2016, the first zinc biofortified wheat variety in Pakistan, the development pipeline has delivered Akhbar and Nawab-21 on to the market in 2017 and 2021 respectively, and Tarnab Rehbar and Tarnab Gandum-1 in 2023. The most recent report from HarvestPlus released in 2022 indicated that the market share of zinc biofortified wheat was projected to reach 20 % of the certified seed sector in 2022, with over 1·4 million households growing zinc biofortified wheat varieties(46).
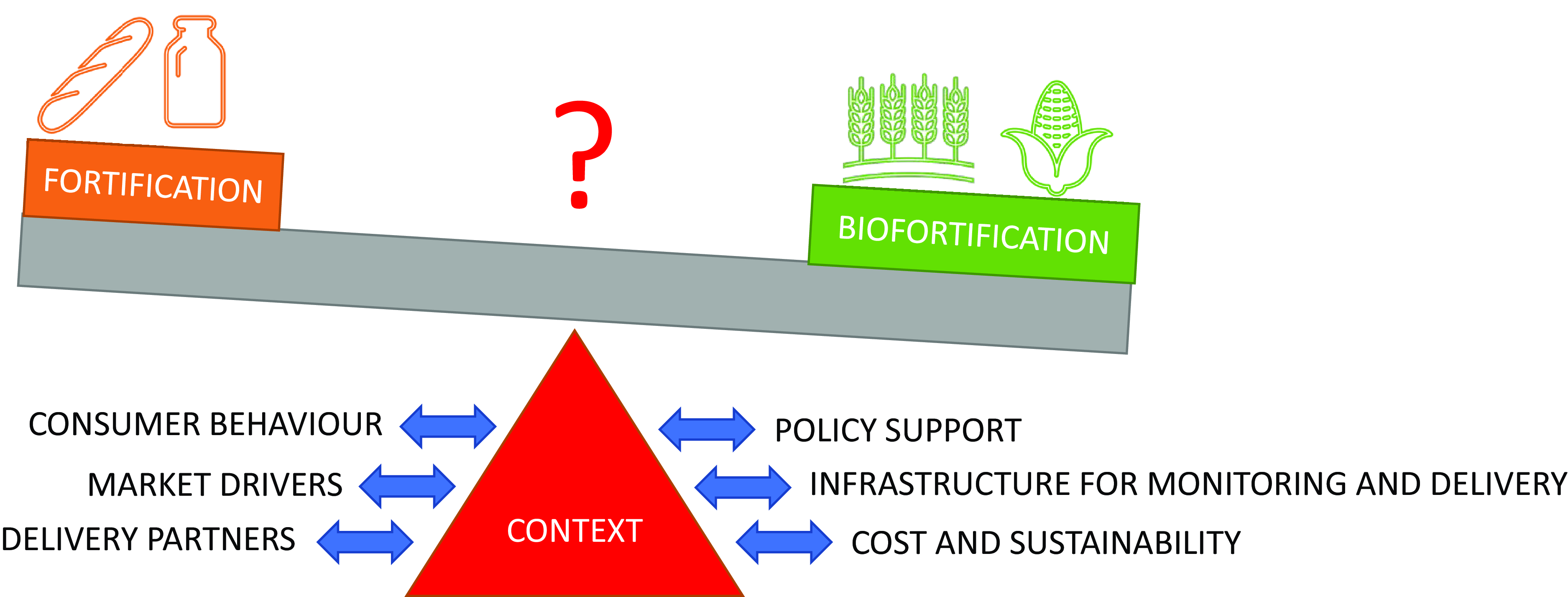
In summary, it is clear that integration of both fortification and biofortification into the mainstream food production system is more likely than employing either method in isolation to have a lasting impact on the debilitating consequences of hidden hunger and reverse the current trend of an increasing prevalence of malnutrition. As illustrated by the case study in Pakistan, the cultural and political context, including the supporting infrastructure and market forces significantly impacts the implementation and ultimate success of both strategies. An in-depth analysis and understanding of the context is required to weigh up the balance of where resources should be invested for maximum impact.
Acknowledgements
I gratefully acknowledge the support of my colleagues and partners involved in the BiZiFED research programme, particularly Dr Victoria Moran and Dr Swarnim Gupta and Prof Erick Boy for their helpful comments during the drafting of this manuscript.
Financial support
The work was supported by UKRI/BBSRC through the Global Challenges Research Fund (grant number BB/P02338X1 and BB/S013989/1).
Author contribution
N.L. is responsible for conceptualizing and writing this review article.
Conflict of interests
There are no conflicts of interest.




 Open access
Open access