Lifestyle-related non-communicable diseases (NCD) account for almost half of all deaths and disability in low-/middle-income countries(Reference Gakidou, Afshin and Abajobir1). It is projected that NCD cases will overtake infectious diseases by 2030 in sub-Saharan Africa (SSA)(Reference Haddad, Hawkes and Udomkesmalee2–Reference Mathers and Loncar4). Even with the worrying trend, NCD are not given due attention as a public health issue in SSA(5,Reference Geneau, Stuckler and Stachenko6) . The key determinants of NCD are overweight and obesity. Prevalence of overweight and obesity is increasing at a high rate in urban SSA particularly among women of reproductive age (WRA). The prevalence is higher among women at a rate that is almost twice as high as in men(Reference Hawkes and Fanzo7). For example, while 18·9 % of urban Ugandan men are overweight/obese, levels among urban women stand at 44 %(8). In Tanzania, an estimated 42 % of urban women are either overweight or obese(9), while in South Africa, the prevalence is at 70 %(Reference Cois and Day10). Maternal overweight and obesity pose health risks to mothers as well as their offspring(Reference Hanson, Barker and Dodd11,Reference Godfrey, Reynolds and Prescott12) . The key modifiable risk factors for overweight and obesity are unhealthy dietary patterns and physical inactivity(Reference Alwan13,Reference Cecchini, Sassi and Lauer14) . Studies depict an increase in physical inactivity in urban Africa, especially among women(Reference Guthold, Stevens and Riley15). Projections show that the 2018–2030 WHO global action plan on physical activity (PA) target (a 15 % relative reduction in insufficient PA) cannot be met(16). Dietary patterns observed among populations of urban low-/middle-income countries show poor alignment with current recommendations(Reference Becquey, Savy and Danel17–Reference Cockx, Colen and De Weerdt21).
At the base of unhealthy dietary and PA behaviours are socio-cultural and environmental determinants which are not only intertwined conceptually but also vary with context(Reference Eldredge, Markham and Ruiter22). In SSA, these determinants are largely shaped by women(Reference Phillips, Comeau and Pisa23–Reference Van ‘T Riet, Den Hartog and Mwangi26). Hence, understanding factors influencing and informing dietary and PA decisions in women is vital. A comprehensive and systematically synthesised overview of determinants of dietary and PA behaviours of WRA is lacking in urban SSA. In this study, a systematic review was conducted to synthesis and to collate determinants of dietary and PA behaviour among WRA in urban SSA according to the socio-ecological framework.
Methodology
Systematic searches of literature were conducted according to a predefined protocol published on PROSPERO (ID: CRD42018108532)(Reference Peter, Christophe and Ogwok27). We followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) as a guideline to conduct and report this systematic review(Reference Moher, Liberati and Tetzlaff28).
Search strategy
Electronic databases of MEDLINE, Embase, Scopus and Web of Science were searched. Additional eligible studies were identified from the bibliographies of included articles (snowballing). The initial search string (Table 1) was developed in Embase using the Population, Intervention, Comparison and Outcome model, combining population (WRA (18–49 years) living in urban SSA), intervention (factors influencing dietary and PA behaviours as risk factors for nutrition-related NCD), comparison (not applicable) and outcome (determinants of dietary and PA behaviours) terms (Table 2). The search string was refined for use in different databases. Searches were conducted from August to September 2018. All identified studies were imported to endnote.
Table 1. Search string developed in Embase
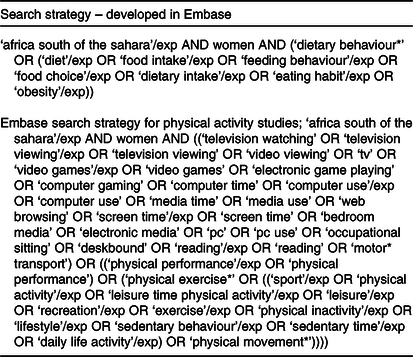
Table 2. PICO criteria used to define research question
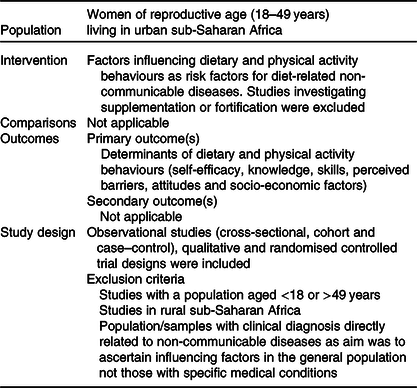
PICO, Population, Intervention, Comparison, Outcome.
Eligibility criteria
The review was restricted to studies published in English from 2000 to September 2018. This timeframe was chosen because the world is changing at a fast rate and determinants before the turn of the century may no longer be relevant. Observational studies (cross-sectional, cohort and case–control), qualitative and randomised controlled trial designs were included. Studies with a population aged <18 or >49 years and those in rural SSA were excluded. Studies conducted in population/samples with clinical diagnosis directly related to nutrition-related NCD were as well excluded.
Study selection
Two reviewers working independently screened the identified studies according to the inclusion criteria to select relevant ones. Prior to this, duplicates were removed. First, one reviewer (P. Y.) screened the titles. Abstracts of selected studies were then reviewed independently by P. Y. and C. M. The full text was read in cases of insufficient information in the title and abstract. The full text of the selected studies was then retrieved and read to determine whether they met the inclusion criteria by one reviewer (P. Y.). Excluded full-text studies were listed with reasons for their exclusion. See PRISMA diagram in Fig. 1.
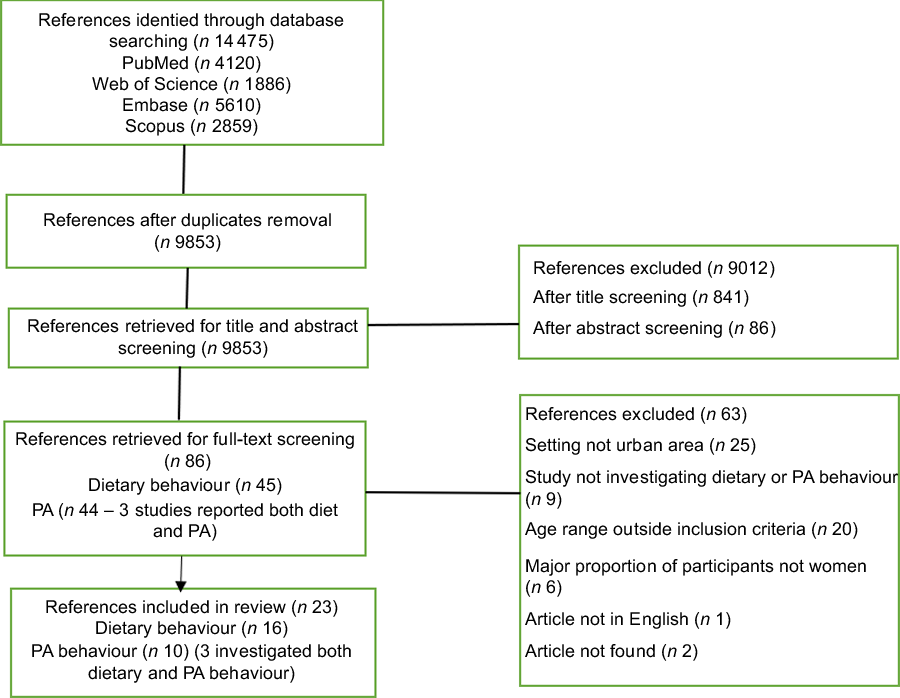
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart showing the study selection process. PA, physical activity.
Data extraction
Data extraction, such as study design, study setting (countries and city), sample size (number of participants), study information (title, author(s), journal and year of publication) and characteristics of participants (type of community, age, sex and social-economic status), was done by a single reviewer. Data extraction for determinants of PA and dietary behaviour (components of specific dietary and PA behaviours studied, how they were measured and outcomes) was initially accomplished by one reviewer (P. Y.). Extracted data were then scrutinised by a second reviewer (C. M.). Data extraction sheets were pilot-tested on five papers before applying them to all included studies. Extracted data are presented in online Supplementary Tables S1 and S2. Identified studies could not allow quantifying the magnitude of identified determinants(Reference Bauman, Sallis and Dzewaltowski29). Thus, data synthesis was narrative. To structure the narrative synthesis, thematic analysis approach was used(Reference Thomas and Harden30). Thematic analysis involved identifying key concepts from studies and organising them into one overall data scheme. The identified key concepts were categorised into themes by constant comparative analysis. Comparative analysis involved taking concepts from one study and recognising the same concepts in other studies. Qualitative research depicts the scope and variation in views, and the uncommon views in a few studies might represent important features(Reference Fade31). Therefore, findings mentioned by a few studies were considered relevant in this review. Themes were structured according to the socio-ecological model. The results from all identified studies were summarised irrespective of methodological quality.
Quality assessment
Standardised quality assessment tools were used to assess the quality of the studies. The ‘standard for reporting for reporting qualitative research tool’ was used to assess qualitative studies(Reference O’Brien, Harris and Beckman32), while the National Heart, Lung, and Blood Institute quality assessment tool for observational cohort and cross-sectional studies was used for cross-sectional studies(Reference Bethesda33). To arrive at quality judgement, we critically appraised how methodological fatal flaws contributed to overall risk of bias.
Results
Description of included studies
The systematic search yielded 9853 studies after duplicate removal. From these studies, ninety-three articles (forty-seven for dietary behaviour and forty-six for PA) were screened for full-text review. From the articles, twenty-three studies (thirteen investigated dietary behaviour only, seven PA, while three investigated both behaviours) were included in quality assessment and analysis (Fig. 1). The characteristics of studies included in analysis are presented in online Supplementary Tables S1 and S2. Searches identified only qualitative studies and descriptive cross-sectional studies. A total of eleven studies used a descriptive cross-sectional design, nine used qualitative, while three used a mixed design. In terms of study setting, the majority were from South Africa and West Africa. Of the sixteen studies on dietary behaviour, six were from South Africa(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34–Reference Stern, Puoane and Tsolekile37) , four from Ghana(Reference Dake, Thompson and Ng19,Reference Boatemaa, Badasu and De-Graft Aikins38–Reference Aryeetey, Oltmans and Owusu40) and two from Burkina Faso(Reference Becquey, Savy and Danel17,Reference Savy, Martin-Prével and Danel41) . Four studies were from Kenya(Reference Van ‘T Riet, Den Hartog and Mwangi26), Tanzania(Reference Cockx, Colen and De Weerdt21), Senegal(Reference Holdsworth, Delpeuch and Landais25) and Cameroon(Reference Kiawi, Edwards and Shu20). Studies on PA were from South Africa(Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42–Reference Walter and du Rosa46) , Nigeria(Reference Adeniyi, Ogwumike and Bamikefa47,Reference Afolabi, Addo and Sonibare48) and Cameroon(Reference Kiawi, Edwards and Shu20).
Quality appraisal
Overall, four of eleven qualitative studies were rated as good quality, four were of poor quality, while three were of moderate quality (online Supplementary Table S3). Strength was well-elaborated data analysis and data collection methods. The main weaknesses were lack of specification of qualitative approach and research paradigm used as well as data management techniques. Majority of studies did not use a theoretical framework as well. Seven of twelve descriptive cross-sectional studies were of moderate/poor methodological quality (online Supplementary Table S4). The main limitations were insufficient description of the study population and sample size. These methodological gaps signify a potential bias, and it is important to interpret study findings while considering the potential bias.
Data synthesis
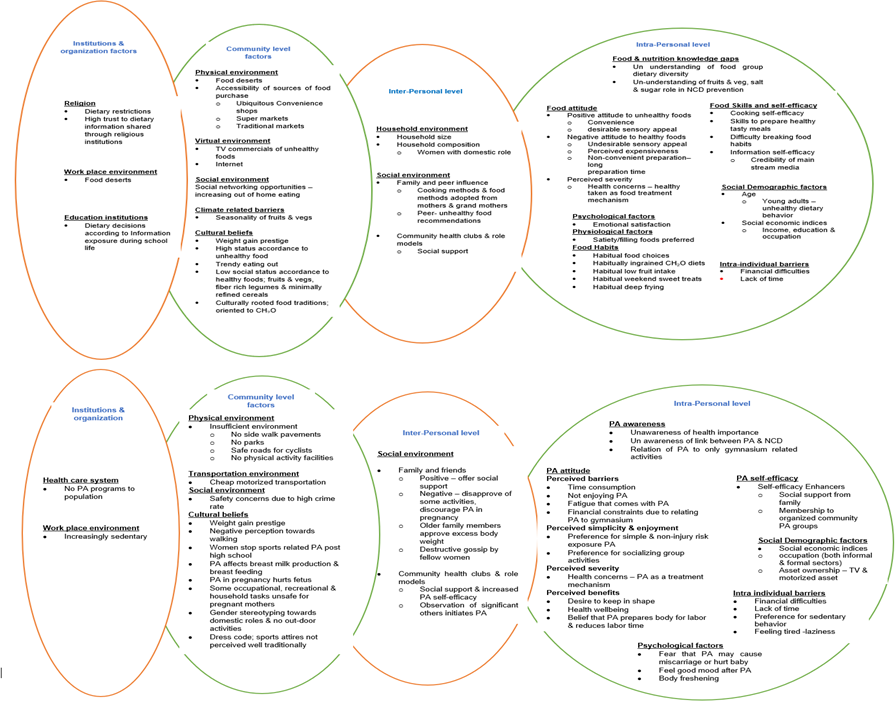
The determinants identified for both behaviours included factors that cut across all the five levels of the socio-ecological framework(Reference Glanz and Bishop49) (Figs 2 and 3). Dietary behaviours studied included: food purchasing(Reference Aryeetey, Oltmans and Owusu40), food choice(Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Stern, Puoane and Tsolekile37,Reference Hiamey, Amuquandoh and Boison39) , healthy eating(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Holdsworth, Delpeuch and Landais25,Reference Boatemaa, Badasu and De-Graft Aikins38) , food environment characteristics(Reference Dake, Thompson and Ng19), nutrition knowledge(Reference Van Den Berg, Okeyo and Dannhauser35,Reference Charlton, Brewitt and Bourne36) and dietary diversity and pattern(Reference Becquey, Savy and Danel17,Reference Cockx, Colen and De Weerdt21,Reference Savy, Martin-Prével and Danel41) . Components of PA studied included: PA pattern(Reference Gradidge, Crowther and Chirwa44,Reference Hattingh, Le Roux and Nel45,Reference Afolabi, Addo and Sonibare48) , PA beliefs(Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37) , PA knowledge and socio-cultural barriers(Reference Kiawi, Edwards and Shu20,Reference Walter and du Rosa46) and experiences of PA during pregnancy and postpartum(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Adeniyi, Ogwumike and Bamikefa47) . Qualitative studies uncovered more of knowledge, attitude and socio-cultural mediators, while cross-sectional studies reported on majorly socio-economic determinants.
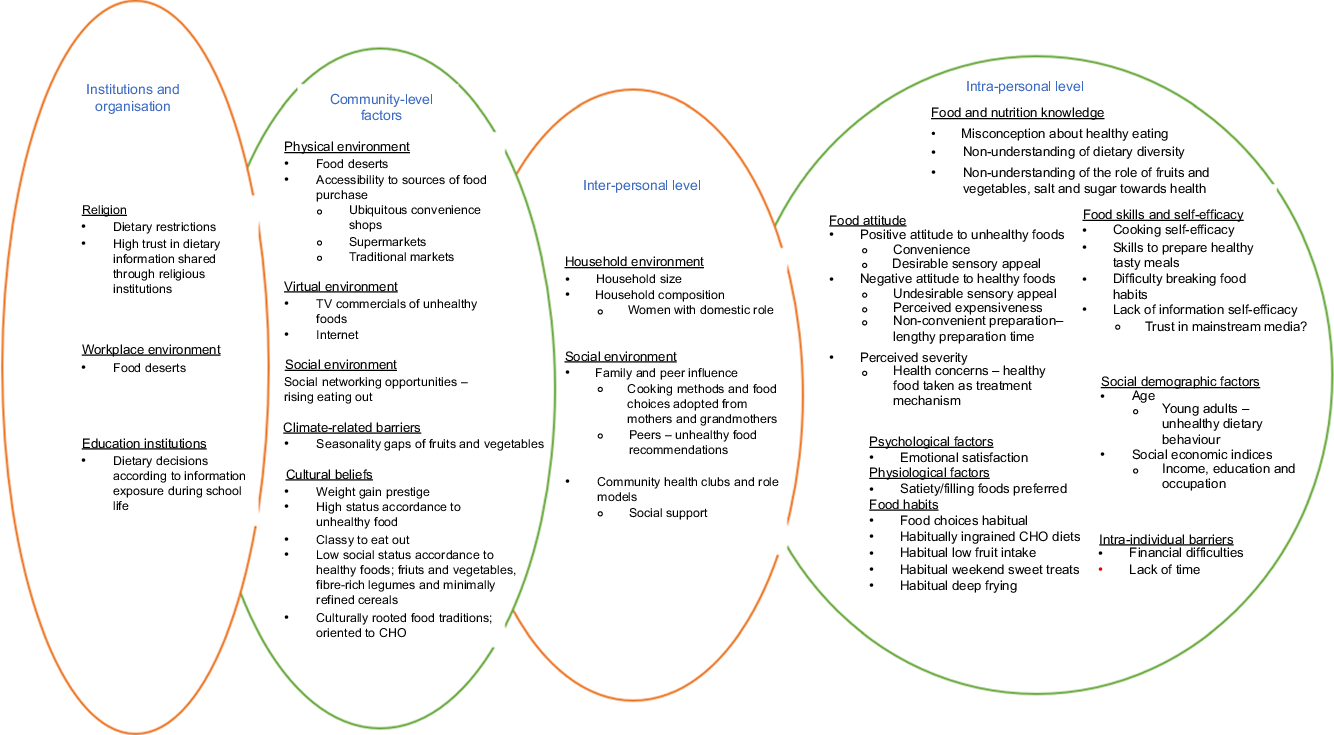
Fig. 2. Determinants of dietary behaviour arranged according to socio-ecological framework. TV, television; CHO, carbohydrate.
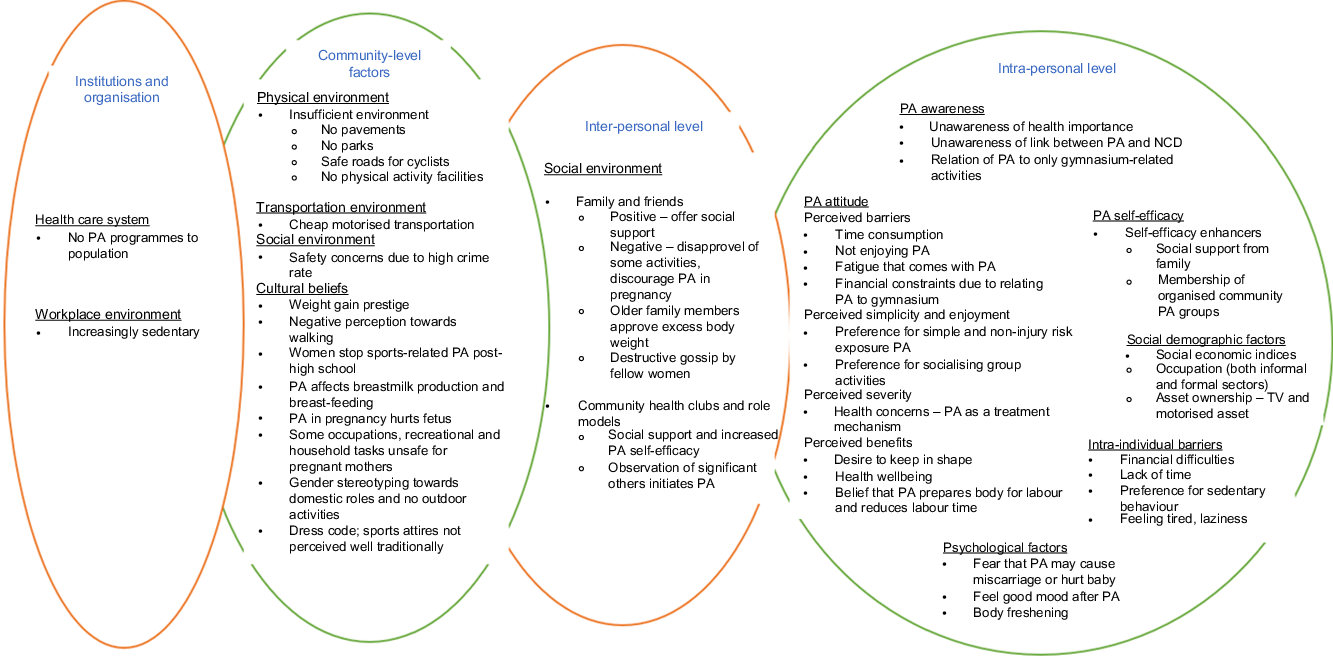
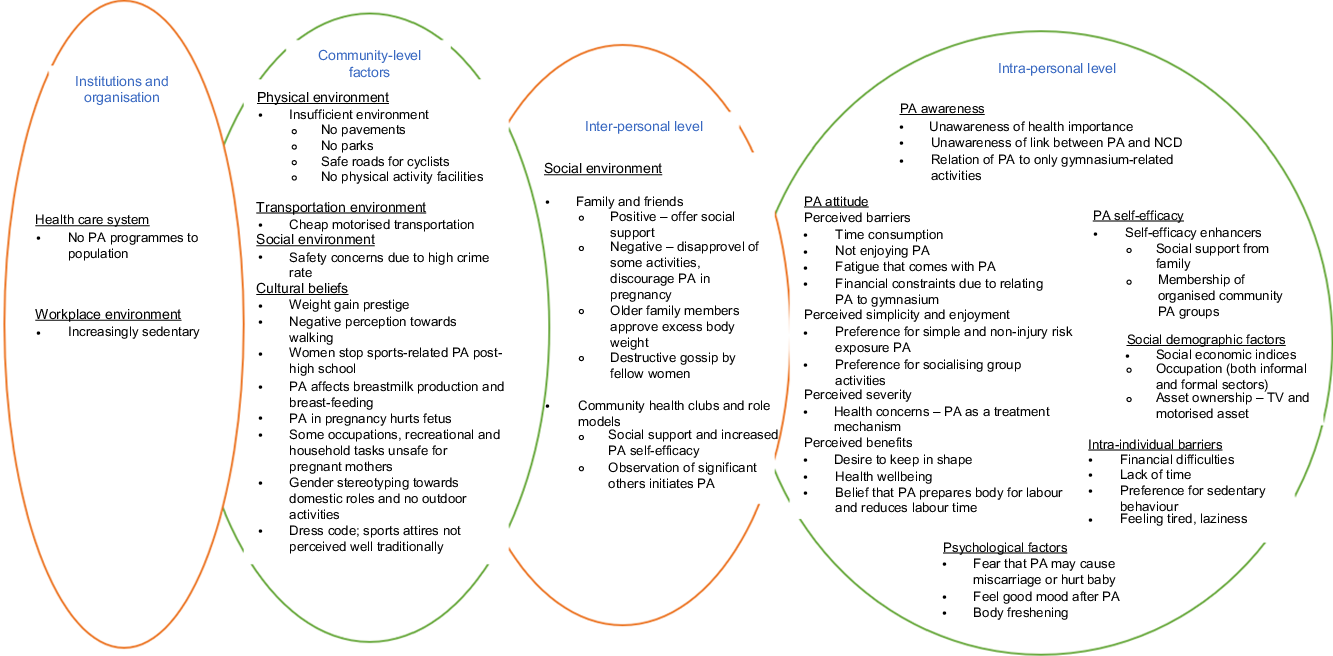
Fig. 3. Determinants of physical activity (PA) behaviour arranged according to socio-ecological framework. TV, television; NCD, non-communicable diseases.
Determinants of dietary behaviour
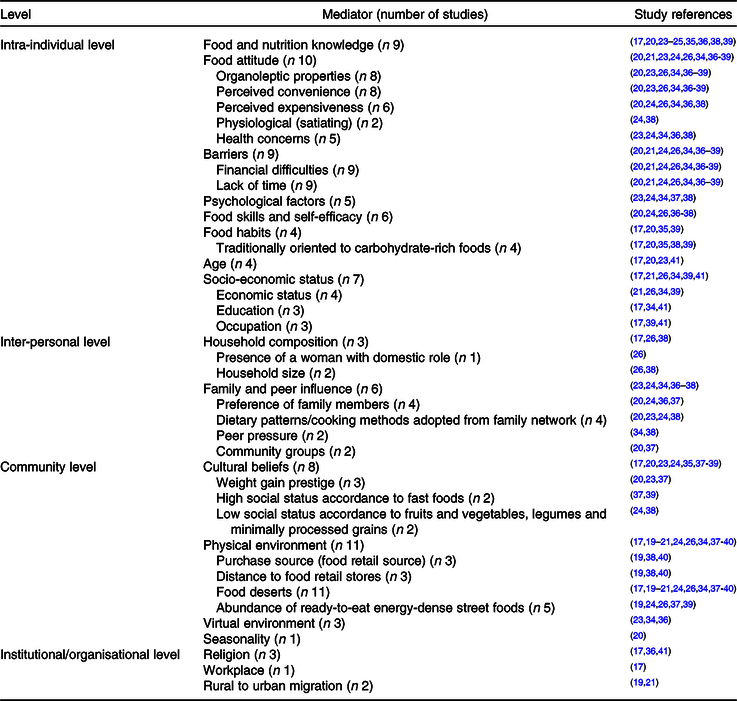
Table 3 gives an overview of determinants of dietary behaviours among WRA in urban SSA.
Table 3. Determinants of dietary behaviour arranged according to the socio-ecological framework
Factors at intra-personal level
Food and nutrition knowledge
Nine studies reported food and nutrition knowledge to have an influence on dietary behaviours(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23–Reference Holdsworth, Delpeuch and Landais25,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38,Reference Hiamey, Amuquandoh and Boison39) . Several misconceptions about healthy eating were reported in qualitative terms. Healthy eating was interpreted in terms of moderate intake of fat with unclear understanding of the benefits of fruits and vegetables and diet diversification. Dietary diversity was understood from the perspective of consuming different foods rather than from concept of food group diversity(Reference Boatemaa, Badasu and De-Graft Aikins38). Knowledge of the role of healthy food to NCD prevention was scanty(Reference Holdsworth, Delpeuch and Landais25,Reference Charlton, Brewitt and Bourne36) . There was a link between fat and NCD, but salt and sugar linkage along with preventive role of fruits and vegetables was not understood. The role of food and nutrition knowledge on dietary behaviours was inconclusive(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Hiamey, Amuquandoh and Boison39) . A study among young adults in South Africa reported that despite having a good understanding of healthy eating, it was not a priority when making dietary decisions(Reference Phillips, Comeau and Pisa23). In contrast, a study among Ghanaian street food consumers found that among the reasons people choose street foods was to compose a healthy diet from the available diversity of foods(Reference Hiamey, Amuquandoh and Boison39).
Food attitude
Ten studies reported attitude to be a determinant of dietary behaviours(Reference Kiawi, Edwards and Shu20,Reference Cockx, Colen and De Weerdt21,Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36–Reference Hiamey, Amuquandoh and Boison39) . All studies reported a positive attitude towards energy-dense diets that are rich in sugar, salt or fat (unhealthy). Unhealthy foods were perceived to have a better taste and to require minimal or no time for preparation(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36–Reference Hiamey, Amuquandoh and Boison39) . Healthy foods, including whole grains, fruits and vegetables, were not preferred by consumers. The high cost of food, long time involved in food preparation and undesirable sensory attributes (tasteless, dry and insipid) explained the negative attitude towards healthy foods(Reference Kiawi, Edwards and Shu20,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38) . Perceived health concerns also influenced dietary behaviours(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38) . Health concerns (adverse health risks to an individual or loved ones) were discussed as elicitors of a positive attitude towards healthy foods(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38) . However, this was discussed to influence older adults. Young adults perceived that health concerns only manifest in old age.
Psychological and physiological factors
Five studies found emotional satisfaction to be a determinant for consumption of foods rich in fat, salt and sugar(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Stern, Puoane and Tsolekile37,Reference Boatemaa, Badasu and De-Graft Aikins38) . Fruits and vegetables were also perceived to be non-satiating(Reference Everett-Murphy, De Villiers and Ketterer24,Reference Boatemaa, Badasu and De-Graft Aikins38) .
Time and financial barriers
Financial difficulties and lack of time were noted as major barriers influencing dietary behaviours(Reference Kiawi, Edwards and Shu20,Reference Cockx, Colen and De Weerdt21,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36–Reference Hiamey, Amuquandoh and Boison39) . Financial difficulties were mentioned as determinants of low fruit and vegetable intake(Reference Kiawi, Edwards and Shu20,Reference Cockx, Colen and De Weerdt21,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38) . Studies on consumption of street foods in Kenya, Ghana and South Africa found that ability to get food on credit and savings on fuel when food preparation is avoided partly explains the increased consumption of these foods(Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Stern, Puoane and Tsolekile37,Reference Hiamey, Amuquandoh and Boison39) . In South Africa and Cameroon, participants perceived that a balanced diet was hard to sustain due to budget constraints.
Food skills and self-efficacy
Dietary behaviours were discussed to be influenced by food preparation skills and self-efficacy(Reference Kiawi, Edwards and Shu20,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Charlton, Brewitt and Bourne36–Reference Boatemaa, Badasu and De-Graft Aikins38) . Participants in a qualitative study in Ghana reported that the ability to improvise with available resources to prepare healthy tasty meals informs their dietary decisions(Reference Boatemaa, Badasu and De-Graft Aikins38). Everett-Murphy et al. (Reference Everett-Murphy, De Villiers and Ketterer24) in South Africa found that many individuals lack the skills and confidence to prepare healthy tasty meals. Participants reported a difficulty in breaking unhealthy entrenched dietary habits(Reference Everett-Murphy, De Villiers and Ketterer24). The difficulty was mediated by rejection of healthy foods by family especially when perceived to be un-tasty.
Food habits (habit strength)
Five studies reported food habits to have an influence on dietary behaviours(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Hiamey, Amuquandoh and Boison39) . High consumption of carbohydrate-rich foods and low consumption of fruits and vegetables are habitually ingrained(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Hiamey, Amuquandoh and Boison39) . In South Africa, sweet treats are social rituals on weekends, while deep frying is an entrenched habit nurtured from childhood(Reference Everett-Murphy, De Villiers and Ketterer24).
Age
Four studies reported age to have an influence on dietary behaviours(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Savy, Martin-Prével and Danel41) . In Cameroon, young adults (18–40 years) regarded fruits and vegetables to be for the older adults (≥40 years)(Reference Kiawi, Edwards and Shu20). Younger Burkinabe adults compared with older adults have a snacking behaviour with mainly energy-dense foods that are nutrient poor(Reference Becquey, Savy and Danel17,Reference Savy, Martin-Prével and Danel41) .
Socio-economic status
Seven studies reported on influence of socio-economic status indices: income/economic, education and occupation on dietary behaviours(Reference Becquey, Savy and Danel17,Reference Cockx, Colen and De Weerdt21,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Hiamey, Amuquandoh and Boison39–Reference Savy, Martin-Prével and Danel41) . Findings are mixed on the direction of influence. A low-income status was found to be a predictor for high consumption of unhealthy street foods in Ghana, Kenya and South Africa(Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Hiamey, Amuquandoh and Boison39) . In contrast, a high-income status in Tanzania was a predictor for consumption of unhealthy foods(Reference Cockx, Colen and De Weerdt21). Three studies found higher education level to be associated with higher dietary diversity and increased likelihood to choose healthy food offers(Reference Becquey, Savy and Danel17,Reference Van Zyl, Steyn and Marais34,Reference Savy, Martin-Prével and Danel41) . Women working in the informal sector (street and market vendors) were reported to depend on majorly street foods(Reference Hiamey, Amuquandoh and Boison39). In urban Burkina Faso, working in the formal sector (professional/corporate jobs) was associated with higher snacking habits(Reference Becquey, Savy and Danel17).
Factors at inter-personal level
Household composition
Household size and composition, according to three studies, had an influence on dietary behaviours(Reference Becquey, Savy and Danel17,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Boatemaa, Badasu and De-Graft Aikins38) . The presence of a housewife was associated with decreased dependence on out of home eating(Reference Van ‘T Riet, Den Hartog and Mwangi26). A large household size was associated with increased prioritisation of satiety-giving carbohydrate-rich foods over other food groups(Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Boatemaa, Badasu and De-Graft Aikins38) .
Family and peer influence
Six studies found dietary decisions to be mediated by the family and friends(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36–Reference Boatemaa, Badasu and De-Graft Aikins38) . Dietary patterns are adopted from largely family networks(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Boatemaa, Badasu and De-Graft Aikins38) . At the same time, the preferences of family members are a vital consideration in dietary choices(Reference Everett-Murphy, De Villiers and Ketterer24,Reference Charlton, Brewitt and Bourne36) . Two qualitative studies in South Africa and Ghana found that due to peer pressure, young adults (≤ 35 years) eat more energy-dense street/fast foods(Reference Van Zyl, Steyn and Marais34,Reference Boatemaa, Badasu and De-Graft Aikins38) . Community groups were also reported as determinants of dietary behaviours.
Factors at community level
Cultural beliefs
Several cultural beliefs influenced dietary behaviours(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Stern, Puoane and Tsolekile37–Reference Hiamey, Amuquandoh and Boison39) . Three studies reported perception of body image to have an influence on food intake(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37) . Overweight is associated with beauty, dignity, health, wealth and good treatment by husband, while weight loss is a source of stigma and a sign of HIV/AIDS(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37) . A positive weight gain perception is a motivation for unhealthy dietary behaviours. Other reported cultural beliefs included low social status accorded to fruits and vegetables, legumes and minimally refined cereals, and high social status accorded to unhealthy fast foods and eating out(Reference Everett-Murphy, De Villiers and Ketterer24,Reference Stern, Puoane and Tsolekile37–Reference Hiamey, Amuquandoh and Boison39) .
Physical environment
Eleven studies reported food choices to be influenced by ubiquitous cheap high energy-dense nutrient-poor foods and food deserts(Reference Becquey, Savy and Danel17,Reference Dake, Thompson and Ng19–Reference Cockx, Colen and De Weerdt21,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Stern, Puoane and Tsolekile37–Reference Aryeetey, Oltmans and Owusu40) . An abundance of ready-to-eat street food offers was reported(Reference Dake, Thompson and Ng19,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Stern, Puoane and Tsolekile37,Reference Hiamey, Amuquandoh and Boison39) . These street offers are limited in fruits and vegetables but provide mostly refined carbohydrate-rich foods. Food purchases are from mainly three retail sources: traditional markets including farmers’ weekly market days, supermarkets and convenience retail stores that offer mainly processed food(Reference Dake, Thompson and Ng19,Reference Aryeetey, Oltmans and Owusu40) . Studies reported that majority of the population still prefer traditional markets because they offer low-priced fresh food. It was also found that proximity to food retail stores determines purchasing behaviour(Reference Aryeetey, Oltmans and Owusu40). Participants in these studies reported a high dependence on convenience stores due to their ubiquity in the communities(Reference Dake, Thompson and Ng19,Reference Boatemaa, Badasu and De-Graft Aikins38,Reference Aryeetey, Oltmans and Owusu40) . Some participants reported weekly food purchasing behaviour to counter accessibility difficulties to traditional markets(Reference Aryeetey, Oltmans and Owusu40).
Virtual/information environment
Three studies reported virtual environment (media) to influence food decisions(Reference Phillips, Comeau and Pisa23,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36) . A strong trust in credibility of nutrition information shared from mainstream media (television and radio) was reported(Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36) .
Factors at institutional level
Religion and food deserts within workplaces influenced dietary choices(Reference Becquey, Savy and Danel17,Reference Charlton, Brewitt and Bourne36,Reference Savy, Martin-Prével and Danel41) . Dietary advice shared through religious institutions was reported to highly influence dietary decisions.
Fig. 2 gives a schematic overview of determinants of dietary behaviour among WRA in urban SSA arranged according to the socio-ecological framework.
Determinants of physical activity behaviour
Table 4 gives an overview of determinants of PA behaviour among WRA in urban SSA.
Table 4. Determinants of physical activity (PA) behaviour arranged according to the socio-ecological framework
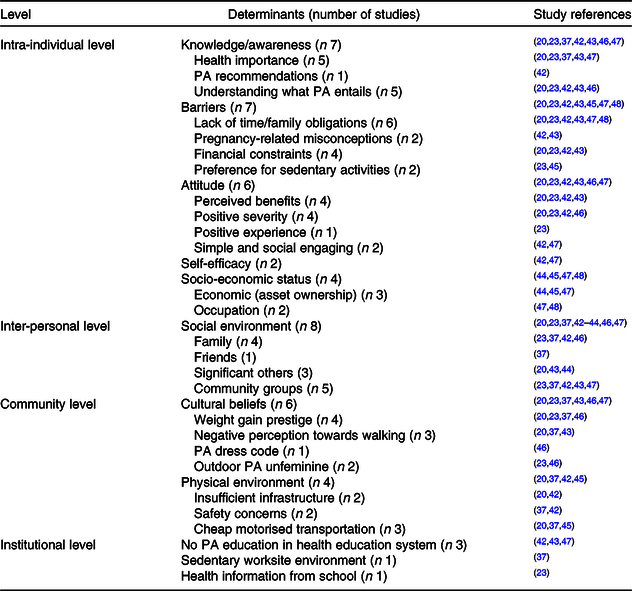
Determinants at intra-personal level
Awareness
Seven studies reported key determinants of PA as being knowledge/awareness of PA recommendations, its health benefits and how one might engage in PA(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Walter and du Rosa46,Reference Adeniyi, Ogwumike and Bamikefa47) . Researchers found a high proportion of participants unaware of the health benefits of PA(Reference Kiawi, Edwards and Shu20,Reference Stern, Puoane and Tsolekile37,Reference Adeniyi, Ogwumike and Bamikefa47) . Health benefits of PA were related to mainly body cleansing(Reference Kiawi, Edwards and Shu20,Reference Watson, Norris and Draper43) . Knowledge on the role of PA in NCD prevention was lacking. Adeniyi et al. (Reference Adeniyi, Ogwumike and Bamikefa47) found that an estimated 61 % of Nigerian women were not aware of PA benefits towards enhancing postpartum health. Studying PA in pregnancy, Muzigaba et al. (Reference Muzigaba, Kolbe-Alexander and Wong42) reported that women were not aware of PA recommendations.
Intra-individual barriers
Barriers included lack of time, feeling tired (laziness), preference for sedentary activities (television viewing) and financial constraints (money to buy bike, to pay at gyms)(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Hattingh, Le Roux and Nel45,Reference Adeniyi, Ogwumike and Bamikefa47,Reference Afolabi, Addo and Sonibare48) . Long working hours and need to prioritise social obligations (family needs) were reported to be a major basis for insufficient time(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Adeniyi, Ogwumike and Bamikefa47) . Physiological changes (increased stomach size) during pregnancy and psychological fear that increased PA may hurt the baby or cause miscarriage were reported to be barriers to PA(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43) .
Physical activity attitude
Perceived severity, benefits and positive experience were reported to have an influence on PA attitude(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Walter and du Rosa46,Reference Adeniyi, Ogwumike and Bamikefa47) . Perceived PA benefits included positive pregnancy outcomes, body freshening, keeping in shape and feel-good mood(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43) . Likewise, health concerns (adverse health risks to an individual or loved one) were discussed to increase likelihood to engage in PA(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Walter and du Rosa46) . Positive experience, for example, blood pressure normalisation resulting from a past PA programme, was reported as a motivator to continue with PA(Reference Phillips, Comeau and Pisa23). The PA perceived to be simple, and socially engaging was described to contribute to a positive attitude(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Adeniyi, Ogwumike and Bamikefa47) .
Physical activity self-efficacy
Two studies reported self-efficacy to be a determinant of PA behaviour(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Adeniyi, Ogwumike and Bamikefa47) . Several factors were described to determine PA self-efficacy. Social support, having a PA buddy or belonging to a group, increased PA self-efficacy(Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Adeniyi, Ogwumike and Bamikefa47) .
Socio-economic status
Four descriptive cross-sectional studies found socio-economic indices, asset ownership and occupation to be associated with PA behaviours(Reference Gradidge, Crowther and Chirwa44,Reference Hattingh, Le Roux and Nel45,Reference Adeniyi, Ogwumike and Bamikefa47,Reference Afolabi, Addo and Sonibare48) . A study among Nigerian women working in informal markets reported that of the total 16 h spent on daily activities, 11·5 h are spent on predominantly sedentary market vending activities(Reference Afolabi, Addo and Sonibare48).
Determinants at inter-personal level
Social environment
Eight studies found family, friends and community groups to have an influence on PA(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42–Reference Gradidge, Crowther and Chirwa44,Reference Walter and du Rosa46,Reference Adeniyi, Ogwumike and Bamikefa47) . Direction of social environment influence was inconclusive. Family members were reported to discourage their relatives from PA they do not approve(Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Walter and du Rosa46) . Membership in a community health club/group positively influenced PA(Reference Stern, Puoane and Tsolekile37,Reference Watson, Norris and Draper43) , while lack of access to sports teams/community groups had a negative influence(Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Adeniyi, Ogwumike and Bamikefa47) . Community groups were reported to offer practical solutions to overcome PA barriers, emotional support and an opportunity to participate in group PA.
Determinants at community level
Cultural beliefs
Six studies reported cultural misconceptions to be determinants of PA(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Watson, Norris and Draper43,Reference Walter and du Rosa46,Reference Adeniyi, Ogwumike and Bamikefa47) . PA is viewed as unfeminine and in conflict with the perceived weight gain prestige(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Walter and du Rosa46) . Walking is considered a sign of poverty and idleness(Reference Kiawi, Edwards and Shu20,Reference Stern, Puoane and Tsolekile37,Reference Watson, Norris and Draper43) . Two studies reported a gender stereotype that women by tradition should not engage in outdoor-related PA(Reference Phillips, Comeau and Pisa23,Reference Walter and du Rosa46) . Dress code also had an influence on PA, and exercise attires (tight and short) are perceived negatively(Reference Walter and du Rosa46).
Physical environment
Insufficient infrastructure (playgrounds, parks, pavements for pedestrians and safe roads for cyclists) and safety concerns (violence against women) were the major impediments to outdoor PA(Reference Kiawi, Edwards and Shu20,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Hattingh, Le Roux and Nel45) . Three studies reported cheap motorised transportation (motor bikes) to influence PA(Reference Kiawi, Edwards and Shu20,Reference Stern, Puoane and Tsolekile37,Reference Hattingh, Le Roux and Nel45) .
Fig. 3 gives a schematic overview of determinants of PA among WRA in urban SSA arranged according to the socio-ecological framework.
Discussion
The review identified twenty-three studies from settings of majorly South and West Africa. In the search, we did not find any randomised controlled trial, quasi-experiment or observational study (e.g. cohort and case–control). A similar finding was reported by Gissing et al.(Reference Gissing, Pradeilles and Osei-Kwasi50) in their mapping review of drivers of dietary behaviour in urban Africa. Across studies, the heterogeneity in methodologies does not allow quantification of determinants’ effects on dietary and PA behaviour. Within the socio-ecological framework, included studies reported factors on mainly the intra/inter-personal and community level. Few studies reported factors on the community, institutional and public policy level.
Dietary behaviour
Notable determinants of dietary behaviour at the intra-individual level were food knowledge, attitude, skills, self-efficacy and psychological factors. In total, nine of sixteen identified studies reported healthy eating to be interpreted in terms of mainly fat intake moderation with unclear understanding of the role of sugar, salt, fruits and vegetables and diet diversification(Reference Becquey, Savy and Danel17,Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23–Reference Holdsworth, Delpeuch and Landais25,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Charlton, Brewitt and Bourne36,Reference Boatemaa, Badasu and De-Graft Aikins38,Reference Hiamey, Amuquandoh and Boison39) . The majority of countries in SSA lack contextualised food-based dietary guidelines, while those in place are poorly communicated(Reference Lachat, Otchere and Roberfroid51,Reference Parker, Steyn and Levitt52) . This partly explains the misconceptions about healthy eating. Research from Northern settings shows that food and nutrition knowledge may inform decisions about food intake and differentiating between healthy and unhealthy foods(Reference Vidgen and Gallegos53–Reference Scripa55). Thus, the misconceptions about healthy eating in urban SSA could unknowingly be translating into unhealthy dietary behaviour.
Emotional and satiety satisfaction are important determinants of food choices. Sensory attributes instigate emotional needs(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Stern, Puoane and Tsolekile37,Reference Boatemaa, Badasu and De-Graft Aikins38) . Due to financial difficulties, hunger satisfaction is a major consideration during food decisions in urban SSA. These findings reinforce recommendations by Perry et al.(Reference Perry, Samra and Edmonstone56) and Vidgen & Gallegos(Reference Vidgen and Gallegos53) that healthy food decisions need not only consider nutrition but also gastronomic needs and available resources (time and money). This signifies a need for knowledge, skills and self-efficacy to plan, manage and deliver healthy but feasible food decisions. In particular, skill to plan healthy food choices on time and budget is paramount to address the financial and time insufficiency barriers. Like in Northern settings(Reference Pettinger, Holdsworth and Gerber57), in urban SSA, female labour market opportunities have increased and do not only limit available time for household domestic roles but also cooking skills(Reference Cockx, Colen and De Weerdt21).
Beyond intra-personal levels, family, peer and community groups influence are notable determinants at the inter-personal level(Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Zyl, Steyn and Marais34,Reference Charlton, Brewitt and Bourne36–Reference Boatemaa, Badasu and De-Graft Aikins38) . At the community level, cultural beliefs, physical and virtual environments are important determinants(Reference Becquey, Savy and Danel17,Reference Dake, Thompson and Ng19–Reference Cockx, Colen and De Weerdt21,Reference Phillips, Comeau and Pisa23,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van Den Berg, Okeyo and Dannhauser35,Reference Stern, Puoane and Tsolekile37–Reference Aryeetey, Oltmans and Owusu40) . In line with findings from high-income countries, unhealthy food choices are linked to endorsement from peers, while the family network influences largely cooking methods and dietary patterns(Reference Sleddens, Kroeze and Kohl58–Reference Deliens, Clarys and De Bourdeaudhuij61). A high regard for community health groups was found. Community health groups offer emotional and valuable support necessary to overcome barriers to unhealthy dietary behaviour(Reference Stern, Puoane and Tsolekile37). Several healthy eating recommendations now recognise the importance of social support in shaping dietary behaviour(Reference Vidgen and Gallegos53,Reference Perry, Samra and Edmonstone56) .
Culture informs food beliefs, while communities align these beliefs with healthy dietary recommendations(Reference Perry, Samra and Edmonstone56,Reference Larson and Story60) . The prevailing food beliefs within urban SSA promote dietary behaviours that deviate from healthy recommendations. Next to food beliefs, cultural norms perpetuate gender constructs that variably influence dietary behaviour. These norms include culturally constructed gender roles and overweight prestige. Overweight among women is perceived as a sign of good treatment by the husband. Because of prestige ensuing from weight gain, husbands are inclined to endorse behaviours that promote overweight(Reference Gissing, Pradeilles and Osei-Kwasi50). In line with findings from other low- and middle-income settings, food shopping and cooking are customarily a woman’s role(Reference Boatemaa, Badasu and De-Graft Aikins38,Reference Caperon, Arjyal and Puja62) . These culturally defined gender roles have implications in dietary behaviours for both men and women. First, it restricts men’s food preparation skills, making them dependent on women. Meanwhile, female labour markets across urban SSA are on the rise which ultimately affects their involvement in household roles like food preparation. Our findings demonstrate increased out of home eating among members in households without housewives(Reference Cockx, Colen and De Weerdt21,Reference Van ‘T Riet, Den Hartog and Mwangi26) . Studies from other settings report unhealthy dietary practices among men compared with women(Reference Caperon, Arjyal and Puja62,Reference Spencer, Rehman and Kirk63) . It is therefore important to understand gender roles for effective behaviour change within the households.
Eleven studies reported food choices in this setting to be influenced by food deserts and ubiquitous availability of cheap high energy-dense nutrient-poor foods(Reference Becquey, Savy and Danel17,Reference Dake, Thompson and Ng19–Reference Cockx, Colen and De Weerdt21,Reference Everett-Murphy, De Villiers and Ketterer24,Reference Van ‘T Riet, Den Hartog and Mwangi26,Reference Van Zyl, Steyn and Marais34,Reference Stern, Puoane and Tsolekile37–Reference Aryeetey, Oltmans and Owusu40) . Over the last decade, supermarkets, street foods and fast food chains with less healthy offers have increased within urban Africa(Reference Dake, Thompson and Ng19,Reference Hiamey, Amuquandoh and Boison39,Reference Aryeetey, Oltmans and Owusu40) . Between 1992 and 2014, per capita energy availability grew by over 10 % in middle- and low-income countries(Reference Steyn and McHiza64). Topical studies in urban SSA have found an association between supermarket purchases and unhealthy weight gain(Reference Demmler, Klasen and Nzuma65–Reference Kimenju, Rischke and Klasen67). The present review has found a high regard of information shared through religious institutions. Use of religious institutions as vehicles of health promotion has shown potential among Black American communities(Reference Newton, Carter and Johnson68).
Physical activity behaviour
Awareness, attitude and self-efficacy were identified as important determinants of PA at the intra-personal level. The awareness of the benefits and different types of PA is still low in SSA. Accordingly, awareness is an important determinant of PA in the SSA setting compared with developed countries. The majority of SSA countries lack action-based PA guidelines. Studies also report inadequate capacity of health personnel(Reference Watson, Norris and Draper43,Reference Lachat, Otchere and Roberfroid51) . For example, in South Africa, only 19 % of health workers provide PA-related information during antenatal visits(Reference Watson, Oddie and Constantinou69).
The review found lack of time to be a major barrier to PA(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Adeniyi, Ogwumike and Bamikefa47,Reference Afolabi, Addo and Sonibare48) . Culturally in the SSA setting, women oversee domestic affairs of the home(Reference Walter and du Rosa46). This coupled with the improving female labour market opportunities, and longer commuting hours (traffic jams and distinct separation of home and work location) greatly diminishes available time for structural-related PA.
Several cultural misconceptions relating to PA were found. The current review found a preference for PA perceived to be simple, like walking. Presently, over 75 % of PA in urban SSA is contributed by travel-related walking(Reference Guthold, Stevens and Riley15). However, participation in walking is threatened by cultural misconceptions which depict walking as a sign of poverty and idleness. With increasing evolution of cheap motorised transportation within urban SSA(16,Reference Kiawi, Edwards and Shu20,Reference Stern, Puoane and Tsolekile37,Reference Hattingh, Le Roux and Nel45) , negative perceptions towards walking may decrease PA. PA is viewed as unfeminine since it affects glossy attractiveness of women due to excess body fat and their traditional domestic roles(Reference Kiawi, Edwards and Shu20,Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Walter and du Rosa46) . Traditionally, women are socialised into gender stereotypical roles by their mothers. Automation and technological advancements are gradually replacing previously active domestic chores(16,Reference Gradidge, Crowther and Chirwa44,Reference Walter and du Rosa46) . Time spent on passive forms of recreation (e.g. television and social media) is increasing(Reference Gradidge, Crowther and Chirwa44). The growing trend in sedentary life requires innovative approach to address gender stereotypes for women being restricted to indoor activities. Initiating a culture of PA opportunities in post high-school period (e.g. adult amateur netball community clubs) could be valuable(Reference Phillips, Comeau and Pisa23). The adjustment of the physical education curriculum could as well prepare communities to accept women’s participation in exercise-related PA(Reference Guthold, Stevens and Riley15,Reference Spencer, Rehman and Kirk63) .
The social environment, particularly community health groups, and PA role models positively influence PA(Reference Phillips, Comeau and Pisa23,Reference Stern, Puoane and Tsolekile37,Reference Muzigaba, Kolbe-Alexander and Wong42,Reference Watson, Norris and Draper43,Reference Adeniyi, Ogwumike and Bamikefa47) . Membership in a community health group may help increase awareness of importance of PA(Reference Walter and du Rosa46). These groups may as well offer practical solutions to PA barriers and misconceptions through experience sharing. According to sport and social sciences, people socialise into PA(Reference Moore, White and Campbell70,Reference Coakley71) . Central agents of socialisation are the community groups. Potential of group activities to increase PA among adults has been reported by Seghers et al. (Reference Seghers, Van Hoecke and Schotte72) in Belgium. Socialisation through community groups could address cultural gender stereotypes around PA in urban SSA.
The physical environment was an important PA determinant in this setting. Built environmental variables like public and private recreational facilities, paved pavements and neighbourhood aesthetics enhance recreational and travel-related PA(Reference Owen, Humpel and Leslie73–Reference Saelens and Handy75). Safety concerns related to increasing crime rates in developing countries have been shown to negatively influence PA in developing settings(Reference Parra, Gomez and Sarmiento76,Reference Gomes, Reis and Parra77) . Feeling unsafe may diminish confidence in the ability to be physically active or willingness to go outdoors(Reference Bennett, McNeill and Wolin78). SSA is rapidly undergoing urbanisation. This urbanisation is largely un-organised and has brought along with it several undesirable effects, chief among them being youth unemployment, a catalyst for crime rates.
Limitations
The review identified mainly studies from South and West Africa. SSA is a very diverse community, and thus, generalisation of the current findings to East and Central African parts of SSA may be challenging. Restriction of the review to English publications could also have limited the scope leaving out publications in French, yet countries of West and Central SSA are predominantly French speaking. Additionally, this review identified majorly cross-sectional studies making causality deduction difficult. Furthermore, a bigger proportion of the qualitative studies identified did not include theoretical framework in their design. Across studies, there was considerable heterogeneity in study designs, assessed indicators, measurement and behaviour components assessed, making comparability of indicators difficult.
Conclusion
This review has proposed socio-ecological frameworks for potential determinants of dietary and PA behaviour among WRA in urban SSA. It highlights salient potential determinants: importance of traditional weekly farmers’ markets, food deserts within work environments, cultural misconceptions (gender stereotypes), virtual environment (media), sedentary home/work environments and cheap motorised transport (motorcycles). However, evidence is from mainly cross-sectional studies and on intra- and inter-personal levels. Research into determinants of dietary and PA behaviour in the context of urban SSA is minimal, particularly on the community, institutional and public policy level. Studies with rigorous qualitative and quantitative designs are required to validate and develop the proposed frameworks further, especially within East Africa. The cross-sectional nature of available evidence makes policy recommendation challenging. Nevertheless, available insights suggest a need for comprehensive skill-based interventions focusing on socio-cultural misconceptions and financial limitations.
Acknowledgements
We acknowledge Constance Herrebout who identified studies from Scopus database and Merel Leyman, Anke Vandycke, Sigrid Devloo and Diane Berardis for their input in quality assessment.
The work was funded by the Belgian Directorate General for Development Cooperation and Humanitarian Aid (DGD), an initiative implemented by VLIR-UOS (Vlaamse Interuniversitaire Raad - Universitaire Ontwikkelingssamenwerking (Flemish Interuniversities Council - University Development Co-operation)).
C. M. and P. Y. were responsible for the design of the study and development of search string. P. Y. carried out the search and performed the initial screening. C. M. and P. Y. independently reviewed abstracts of selected studies. P. Y. extracted the data, and C. M. helped with interpretation of the data. P. Y. drafted the initial manuscript. All authors contributed to interpretation of the results and critical review of the manuscript and approved the final manuscript.
The authors have no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114520001828