



Introduction
In times of national crisis, individual differences in explanatory beliefs may affect the degree of adherence to necessary collective responses. Accurate beliefs foster helpful behaviours; erroneous beliefs foster unhelpful behaviours. In the current coronavirus pandemic, we focus on the potential influence of false conspiracy theories (Sunstein & Vermeule, Reference Sunstein and Vermeule2009) on the English population's response. Conspiracy theories typically have four common characteristics (Freeman & Bentall, Reference Freeman and Bentall2017): the world or an event is held to be not as it seems; there is believed to be a cover-up by powerful others; the theory is accepted only by a minority; and the theory is unsupported by evidence. There are likely to be varying degrees of such mistrust, from excessive scepticism to detailed ideas concerning perpetrators, motivations, and modi operandi. This mistrust can be conceptualised as a conspiracy mentality (Brotherton, French, & Pickering, Reference Brotherton, French and Pickering2013; Goertzel, Reference Goertzel1994; Imhoff & Bruder, Reference Imhoff and Bruder2014): a way of seeing the world that is marked by antipathy to official or mainstream accounts or to those in higher status positions. This conspiracy mind-set can be seen in evidence that holding one conspiracy belief raises the likelihood of unrelated conspiracy beliefs (Swami, Chamorro-Premuzic, & Furnham, Reference Swami, Chamorro-Premuzic and Furnham2010) and that individuals can simultaneously endorse mutually incompatible conspiracy beliefs (Wood, Douglas, & Sutton, Reference Wood, Douglas and Sutton2012). Conspiracy beliefs are unlikely to be benign. For instance, parental belief in anti-vaccine conspiracy theories is associated with lower intent to vaccinate a child (Jolley & Douglas, Reference Jolley and Douglas2014), while such theories are cited by parents who do not vaccinate their children (Attwell, Leask, Meyer, Rokkas, & Ward, Reference Attwell, Leask, Meyer, Rokkas and Ward2017; Luthy, Beckstrand, Callister, & Cahoon, Reference Luthy, Beckstrand, Callister and Cahoon2012). In our view multiple features of the current pandemic make conspiracy beliefs likely to develop and propagate. Such erroneous beliefs will weaken collective actions necessary to minimise harm to the population.
Our perspective on conspiracy beliefs is rooted in the psychology of mistrust. Conspiracy theories are attempts to explain world events that are threatening or inconsistent with personal expectations. The acceptance of conspiracy explanations is much more likely when an individual tends to mistrust. A mistrusting mind-set – a defensive response of wariness – will occur when there is perceived vulnerability and a sense of assailment. Perceptions of vulnerability and attack can be linked to low self-esteem, poorer psychological well-being, powerlessness, and anger. Mistrust of authority or higher status groups is more likely when there is a perception of (real or subjective) social marginalisation. When emotion is heightened by perceived danger, individuals are likely to accept the explanations, however unlikely, that conform to preconceptions. The more cognitively taxing process of carefully weighing up the evidence for and against different explanations is unlikely to be adopted. Conspiracy beliefs are likely to bring short-term benefits, such as a reduction in uncertainty and increase in control; access (often online) to like-minded people; and a sense of having privileged information. It has been argued that the benefits can be categorised as epistemic (e.g. understanding), existential (e.g. control), and social (e.g. positive self-image) (Douglas et al., Reference Douglas, Uscinski, Sutton, Cichocka, Nefes, Ang and Deravi2019). Conspiracy beliefs and paranoia are associated (Goreis & Voracek, Reference Goreis and Voracek2019) but the shared nature of conspiracy beliefs is most likely less unhealthy in comparison to paranoia, in which the individual alone is the target. Empirical evidence has linked conspiracy beliefs to perceptions of threat from societal change (Federico, Williams, & Vitriol, Reference Federico, Williams and Vitriol2018), uncertainty (van Prooijen & Jostmann, Reference van Prooijen and Jostmann2013), powerlessness (Abalakina-Paap, Stephan, Craig, & Gregory, Reference Abalakina-Paap, Stephan, Craig and Gregory1999), lack of socio-political control (Bruder, Haffke, Neave, Nouripanah, & Imhoff, Reference Bruder, Haffke, Neave, Nouripanah and Imhoff2013), perceptions of lower social status (Freeman & Bentall, Reference Freeman and Bentall2017), less analytic thinking (Swami, Voracek, Stieger, Tran, & Furnham, Reference Swami, Voracek, Stieger, Tran and Furnham2014), lower levels of education and income (Douglas, Sutton, Callan, Dawtry, & Harvey, Reference Douglas, Sutton, Callan, Dawtry and Harvey2016; Freeman & Bentall, Reference Freeman and Bentall2017), and being a member of a disadvantaged social group (Davis, Wetherell, & Henry, Reference Davis, Wetherell and Henry2018). Political extremes (left or right) are most associated with the endorsement of conspiracy beliefs (Krouwel, Kutiyski, van Prooijen, Martinsson, & Markstedt, Reference Krouwel, Kutiyski, van Prooijen, Martinsson and Markstedt2017; van Prooijen, Krouwel, & Pollet, Reference van Prooijen, Krouwel and Pollet2015).
The coronavirus pandemic and associated countermeasures have created conditions in which conspiracy beliefs are likely to develop. Such conditions include the sense of vulnerability triggered by the sustained threat to physical health, psychological well-being, and financial security. Uncertainty about the future is widespread. Expectations about everyday life have changed rapidly and dramatically, with top-down imposition of explanations and required responses, enforceable by law. Normal routines and plans have been thwarted. The effects of the countermeasures are likely to have been greatest in those in lower socio-economic circumstances. There is much talk of medical tests and vaccinations, while many individuals have greater time to themselves, in isolation, and with the Internet to hand. We hypothesise that: a significant minority of the population hold excessively sceptical views, including clear false conspiracy beliefs, of official explanations of the coronavirus pandemic; these ideas connect with pre-existing conspiracy theories, especially about vaccinations; and conspiracy ideas are associated with less compliance with government guidance such as social distancing and less willingness to take up future tests and vaccinations. We would expect conspiracy beliefs to be more likely to be held by those who are more marginalised, reflected by lower levels of psychological well-being, education, and income. We also took the opportunity to survey individuals’ appraisals of positive outcomes in the response to the pandemic.
Methods
Participants
An online survey with a quota sampled participant group was conducted by Lucid (https://luc.id/) from 4th May 2020 to the 11th May 2020. The quotas used were based upon UK Office for National Statistics (ONS) population estimate data. The quotas were for gender (males = 49.35%, females = 50.65%), age (<18 = 21.30%, 18–24 = 9.4%, 25–34 = 13.4%, 35–44 = 14.00%, 45–54 = 13.7%, 55–64 = 11.70%, 65–99 = 16.50%), region (South East = 16.33%, North West = 13.04%, East = 11.09%, West Midlands = 10.55%, South West = 9.94%, East Midlands = 8.58%, North East = 4.76%, London = 15.92%, Yorkshire and the Humber = 9.79%), and income (<£ 15 000 = 17.06%, 15 000–19 999 = 9.11%, 20 000–29 999 = 18.63%, 30 000–39 999 = 15.32%, 40 000–49 999 = 11.81%, 50 000–59 999 = 7.51%, 60 000–69 999 = 5.58%, 70 000–99 999 = 8.58%, 100 000–149 000 = 4.15%, 150 000 + = 2.25%). Lucid's platform serves as a centralised source for survey responses, working with over 250 survey suppliers, all of whom adhere to the ESOMAR Guidelines (https://www.esomar.org/what-we-do/code-guidelines). Lucid operates a marketplace in which they advertise the survey to suppliers, who provide individual participants, with sampling by Lucid from this pool. The advantage of using multiple survey sources is substantially less reliant on any particular demographic or segment of the population. Respondents will have been sourced from: ads and promotions across digital networks, search, word of mouth and membership referrals, social networks, online and mobile games, affiliate marketing, banner ads, offerwalls, TV and radio ads, and offline recruitment with mail campaigns. Participants have opted in to being a panel member for the supplier as well as providing informed consent to this particular survey. Individuals are not included if they have responded to all questions in the same way or have a completion time that is less than one-third of the median.
The Oxford Coronavirus Explanations, Attitudes, and Narratives Survey (OCEANS) was approved by the University of Oxford Central University Research Ethics Committee (R 69510/RE001) and all participants provided informed consent. Participants were given the following rationale for OCEANS: ‘Coronavirus has been a shock and lives have changed dramatically. At times of crisis, people may think of lots of different explanations for what is occurring. We are interested in how common different views may be and how they influence responses to the crisis. It may inform the extent to which people follow current lockdown guidance and take-up future treatments… A wide-range of views are asked – some have a lot of evidence supporting them, others have no evidence supporting them. You may agree or disagree with explanations provided’.
Assessments
We collected demographic data, information on how the pandemic had affected each participant, and where they obtained information about the virus. On seven-point scales, participants rated religiosity (0 = not all religious, 6 = strongly religious) and political viewpoint (0 = strongly left wing, 6 = strongly right wing). They were also asked how they viewed the importance of voting in general elections.
Conspiracy mentality questionnaire (CMQ) (Bruder et al., Reference Bruder, Haffke, Neave, Nouripanah and Imhoff2013)
This five-item scale assesses a non-content specific tendency to see secretive forces behind events (e.g. ‘there are secret organizations that greatly influence political decisions’). Each item is rated on an 11-point scale from 0% (certainly not) to 100% (certain) scale. Higher scores indicate a greater degree of conspiracy mentality. Cronbach's α in the current study was 0.88.
Coronavirus conspiracy explanations
We asked participants to rate the extent to which they agreed with 48 conspiracy statements. Each item is rated on a five-point scale: do not agree (1), agree a little (2), agree moderately (3), agree a lot (4), agree completely (5). A higher score indicates greater endorsement of a statement. The list of statements comprised: scepticism about the government's response (n = 3) (e.g. ‘I'm sceptical about the official explanation about the cause of the virus’), general conspiracy views on the cause of the virus (n = 3) (e.g. ‘The virus is a hoax’), general conspiracy views about the spread of the virus (n = 7) (e.g. ‘The spread of the virus is a deliberate attempt to reduce the size of the global population’), general conspiracy views about the reasons for lockdown (n = 5) (e.g. ‘The real reason for the lockdown is to impose mass surveillance’), and then specific conspiracy beliefs (n = 30) (e.g. ‘The elite have created the virus in order to establish a one-world government’). The statements were generated from searching the internet in the preceding weeks of the lockdown, looking at both mainstream and alternative sites, which produced an initial list of 99 conspiracy statements. The selection of items tried to balance out possibly opposing political and religious views on causes and motivations. We also assessed agreement with four official explanations (e.g. ‘The virus is most likely to have originated from bats’).
Following of UK government coronavirus guidance
Participants were asked to rate how often they followed six key aspects of government guidance on a five-point scale (not at all, occasionally, some of the time, most of the time, all of the time). Higher scores indicate greater levels of following the guidance. Participants were also asked to rate on the same scale two general items assessing how much they follow the guidance now and how much they will in the future.
Future medical tests and treatment
Participants were asked to rate on a five-point scale (definitely, probably, possibly, probably not, definitely not) how likely it was that they would accept diagnostic tests and vaccination for coronavirus, and whether they would wear a facemask outside if advised. Higher scores indicate lower potential engagement.
Sharing coronavirus information
Participants were asked two questions concerning the degree to which they shared with other information or opinions about the coronavirus. Each was rated on a five-point scale (not at all, occasionally, some of the time, most of the time, all of the time). Higher scores indicate greater sharing.
Vaccine conspiracy beliefs scale (Shapiro, Holding, Perez, Amsel, & Rosberger, Reference Shapiro, Holding, Perez, Amsel and Rosberger2016)
This seven-item questionnaire asks participants how much they agree on a seven-point scale (strongly disagree, disagree, somewhat disagree, neutral, somewhat agree, agree, strongly agree) with vaccine conspiracy statements (e.g. ‘Vaccine safety data is often fabricated’). Higher scores indicate greater endorsement of vaccine conspiracy statements. Cronbach's α in the current study was 0.95.
Climate change conspiracy belief (Bolsen & Druckman, Reference Bolsen and Druckman2018)
Participants were asked to rate on a seven-point scale (strongly disagree, disagree, somewhat disagree, neither agree nor disagree, somewhat agree, agree) how much they agreed with the statement ‘The idea that climate change is primarily due to human activities is a hoax or a conspiracy’. Higher scores indicate greater belief in the conspiracy.
Trust barometer (Edelman, 2020)
Items were constructed, based on the barometer, to assess levels of trust in a number of institutions and professions. Each item is rated on a five-point scale (1 never trust, 2 rarely trust, 3 sometimes trust, 4 often trust, 5 always trust).
Revised Green et al. paranoid thoughts scale – part B (R-GPTS) (Freeman et al., Reference Freeman, Loe, Kingdon, Startup, Molodynski, Rosebrock and Bird2019)
This 10-item questionnaire assesses persecutory ideation over the past fortnight. Each item (e.g. ‘Certain individuals have had it in for me’.) is rated on a 0 (not at all) to 4 (totally) scale. Higher scores indicate higher levels of paranoia. Cronbach's α in the current study was 0.97.
Warwick−Edinburgh mental well-being scale (WEMWBS) (Tennant et al., Reference Tennant, Hiller, Fishwick, Platt, Joseph, Weich and Stewart-Brown2007)
The WEMWBS is a 14-item scale assessing psychological well-being over the past fortnight. Each item (e.g. ‘I've been feeling optimistic about the future’) is rated on a 1 (none of the time) to 5 (all of the time) scale. Higher scores indicate a greater level of well-being. Cronbach's α in the current study was 0.93.
Positive experiences of the pandemic
At the end of the survey participants were asked to rate on a five-point scale (do not agree, agree a little, agree moderately, agree a lot, agree completely) 17 potential positive aspects of the pandemic (e.g. ‘The coronavirus pandemic has brought communities closer together’). Higher scores indicate greater endorsement of positive aspects of the crisis.
Analysis
The first main reporting was descriptive, providing the prevalence of endorsement of items. 95% confidence intervals (CI) for prevalence percentages were estimated using bootstrapping with 1000 samples. Data reduction, using principal components analyses, was carried out separately for the 18 general coronavirus conspiracy theory items and the 30 specific coronavirus conspiracy items. The primary principal component factors (without rotation) that explained 61.3% and 69.4% of the variance respectively, were used to test associations with the other variables. No attempt was made to fit formal measurement models (e.g. via confirmatory factor analysis), since this is unnecessary for the data simplification process (see Freeman et al., Reference Freeman, Dunn, Murray, Evans, Lister, Antley and Morrison2015). Associations were then tested using Pearson's correlations, t tests, ANOVAs, and chi-square tests. There were no missing data. All statistical testing was two-tailed. The analyses were carried out using SPSS Version 25.0.0.1 (IBM, 2017).
Results
A summary of demographic information about the participant group is provided in Table 1. The group is consistent with the quota sampling targets for age, gender, income, and region.
Table 1. Demographic information

In Table 2, a summary is provided of the frequency of endorsement of each general and specific coronavirus conspiracy belief. The mean total specific coronavirus conspiracy score was 46.1, s.d. = 26.0 (minimum = 30, maximum = 150, 25th percentile = 30, 50th percentile = 32, 75th percentile = 48, 90th percentile = 91), the mean total generic coronavirus conspiracy score was 34.1 (s.d. = 17.0) (minimum = 18, maximum = 90, 25th percentile = 20, 50th percentile = 27, 75th percentile = 45, 90th percentile = 60), and the mean total score for the four official explanations was 12.9, s.d. = 3.4 (minimum = 4, maximum = 20, 25th percentile = 10, 50th percentile = 13, 75th percentile = 15). Endorsement scores for all specific conspiracy items significantly positively correlated with one another, and similarly all generic conspiracy items significantly positively correlated with one another. The correlation between the specific and generic coronavirus conspiracy principal component scores was high, r = 0.84, p < 0.001. Specific conspiracy beliefs, r = −0.101, p < 0.001, and generic conspiracy beliefs, r = −0.21, p < 0.001, were both negatively associated with the total endorsement score for the official explanations.
Table 2. Endorsement of general and specific coronavirus conspiracy beliefs and official explanations

There were no significant differences in levels of specific, t(df = 2451.5) = 1.89, p = 0.056, or general, t(df = 2466.3) = 0.69, p = 0.491, coronavirus conspiracy beliefs by gender. Younger participants held higher levels of both specific, r = −0.42, p < 0.001, and general, r = −0.35, p < 0.001, coronavirus conspiracy beliefs. There were lower levels of both specific, df = 407.0, t = −9.44, p < 0.001, and general, df = 426.8, t = −8.21, p < 0.001, coronavirus conspiracy concerns in those of white ethnicity (n = 2160) compared to individuals of other ethnicities (n = 341). There were no significant associations of specific, r = 0.02, p = 0.25, or general, −0.02, p = 0.418, coronavirus conspiracy concerns with household income. General conspiracy, r = −0.06, p = 0.002, but not specific, r = −0.01, p = 0.526, coronavirus conspiracy concerns, were associated with lower levels of education. Specific and general coronavirus conspiracy beliefs were significantly higher in those who thought it not worth voting in a general election (n = 195) compared with individuals who thought you should only vote if you care who wins (n = 512), with the latter scoring significantly higher for coronavirus conspiracy beliefs than individuals who consider it everyone's duty to vote (n = 1794). Individuals (n = 1825) who obtained most of their information about coronavirus from the BBC had lower levels of specific, df = 934.8, t = 11.91, p < 0.001, and general, df = 1058.2, t = 12.09, p < 0.001 coronavirus beliefs compared with those who did not (n = 676). Whereas individuals (n = 453) who obtained most of their information about coronavirus from friends had higher levels of specific, df = 602.6, t = −5.77, p < 0.001, and general, df = 618.61, t = −6.24, p < 0.001 coronavirus beliefs compared with those who did not (n = 2048). Similarly, individuals (n = 808) who obtained most of their information about coronavirus from social media had higher levels of specific, df = 1263.6, t = −12.27, p < 0.001, and general, df = 1345.61, t = −12.73, p < 0.001 coronavirus beliefs compared with those who did not (n = 1693). Individuals (n = 382) who obtained most of their information about coronavirus from YouTube had higher levels of specific, df = 470.73, t = −10.39, p < 0.001, and general, df = 494.11, t = −11.06, p < 0.001 coronavirus beliefs compared with those who did not (n = 2119).
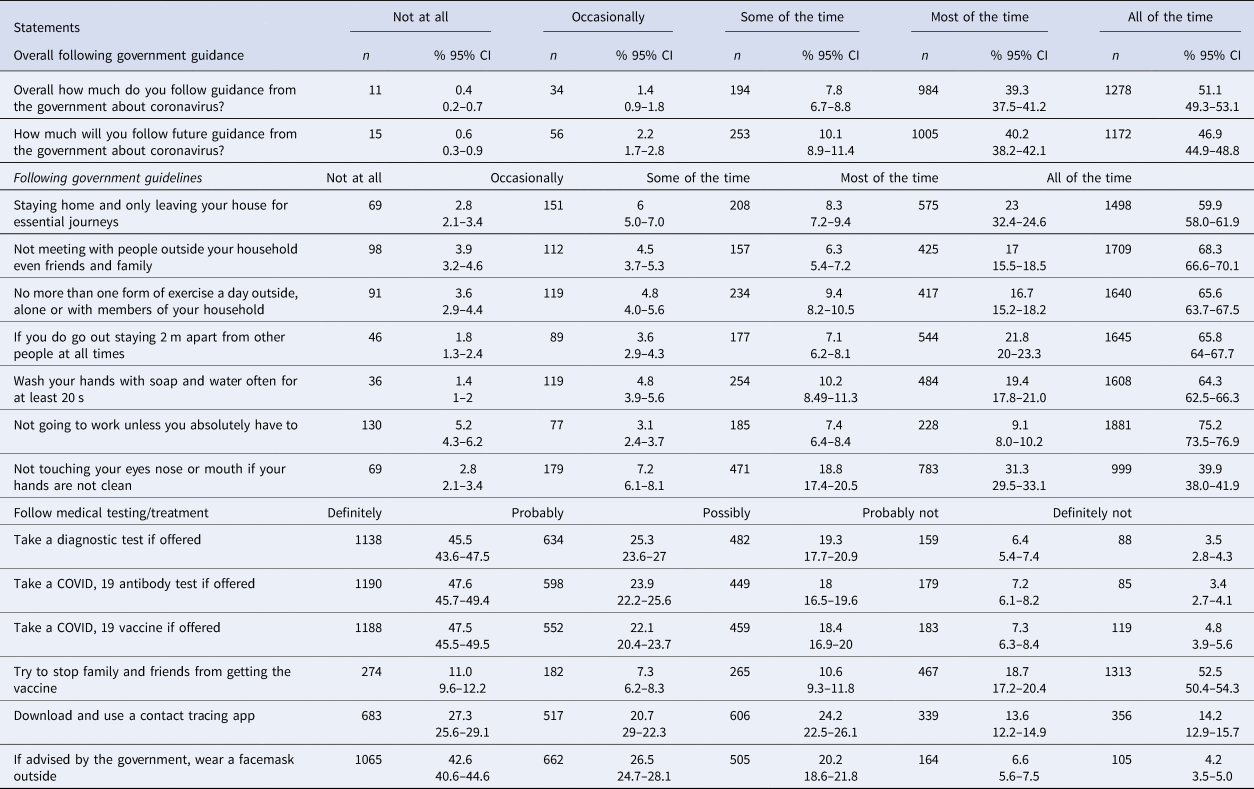
The degree to which participants adhere to government coronavirus guidance and willingness to accept future diagnostics and vaccination is summarised in Table 3. Generally, rates of adhering to the guidelines were high, though approximately 20% adhered to a lower extent.
Table 3. Following of government coronavirus guidance and willingness to accept future diagnostics and vaccination
Endorsement of specific or generic coronavirus conspiracy beliefs is significantly associated with less self-reported adherence to each government recommendation (Table 4). Conspiracy beliefs were also associated with less likelihood to accept future diagnostic tests or a vaccination. As illustrations of these associations, respondents who endorsed to any degree that ‘Coronavirus is a bioweapon developed by China to destroy the West’ were much more likely to also not adhere (defined as less than most of the time) to the guidance to stay at home, odds ratio (OR) 4.57, 95% CI 3.62–5.79, and endorsing to any degree that ‘Jews have created the virus to collapse the economy for financial gain’ was highly associated with not adhering to the guidance to stay at home, OR 14.34, 95% CI 11.26–18.25. Respondents were more likely to report that they would not accept a COVID-19 vaccine (possibly not, definitely not) if they endorsed the bioweapon belief, OR 2.11, 95% CI 1.65–2.70, or the belief about Jewish people, OR 2.70, 95% CI 2.08–3.50.
Table 4. Associations of coronavirus conspiracy beliefs with following government guidelines

Coronavirus conspiracy concerns were associated with all other forms of mistrust, notably paranoia, general vaccination conspiracy beliefs and climate change conspiracy belief (Table 5).
Table 5. Associations of coronavirus conspiracy concerns and general mistrust

Holding specific or general coronavirus conspiracy beliefs was associated with higher levels of religiosity, slightly more right wing political orientation, and being more likely to share information and opinions about coronavirus (Table 6). Although there is a small association of coronavirus conspiracy beliefs with degree of right wing views, there was also evidence for a quadratic relationship, with those who rated themselves as at the extreme ends of either left or right holding higher levels of conspiracy thinking. A hierarchical regression showed that both the linear political item, B = −0.28, standard error = 0.05, t = −5.92, p < 0.001, and a quadratic term (the political item squared), B = 0.064, standard error = 0.01, t = 8.63, p < 0.001 were significant predictors of specific coronavirus conspiracy scores. A similar finding was found for holding general coronavirus conspiracy beliefs. There was little indication of an association of coronavirus conspiracy beliefs with psychological well-being.
Table 6. Associations of coronavirus conspiracy concerns and general mistrust

The endorsement of positive experiences from the pandemic is summarised in Table 7. These show that at a personal and local level there have been positive aspects appraised by most people. Higher levels of specific coronavirus conspiracy beliefs, r = 0.20, p < 0.001, and general coronavirus conspiracy beliefs, r = 0.21, p < 0.001, were associated with higher levels of endorsement of the positive statements.
Table 7. Positive experiences of the coronavirus pandemic

Discussion
The results are illuminating but dispiriting: a substantial minority of the population endorses unequivocally false ideas about the pandemic. Only half the population showed little evidence of conspiracy thinking. The idea that the current crisis may be especially fertile ground for conspiracy beliefs may well be correct. The coronavirus conspiracy ideas ascribe malevolent intent to individuals, groups, and organisations based on what are likely to be long-standing prejudices. For instance, almost half of participants endorsed to some degree the idea that ‘Coronavirus is a bioweapon developed by China to destroy the West’ and around one-fifth endorsed to some degree that ‘Jews have created the virus to collapse the economy for financial gain’. The conspiracy beliefs were connected to a number of markers of excessive mistrust: paranoia, endorsement of other conspiracy beliefs, mistrust in institutions and experts, and a conspiracy mentality. Conspiracy beliefs are likely to be both indexes and drivers of societal corrosion. They matter in this context because they may well have reduced compliance with government social distancing guidelines, thereby contributing to the spread of the disease. One consequence of this national crisis may be to reveal fully the harmful effects of mistrust and misinformation.
A public health information crisis may be observable. Misinformation and misguided – often malign – views look to be highly prevalent. Fringe beliefs may now be mainstream. A previously defining element that the beliefs are typically only held by a minority may require revision. The numerous different conspiracy statements, often contradictory in detail, were all significantly associated. The detailed content of the statements may matter less than the respondents’ tendency to believe that institutions, officials, and experts may be deliberately misleading. This is consistent with previous research that shows mutually incompatible conspiracy beliefs can be endorsed (Wood et al., Reference Wood, Douglas and Sutton2012) and with the noticeably high associations in this study of coronavirus conspiracy beliefs with paranoia (i.e. the idea that others intend harm to the individual) and conspiracy beliefs concerning vaccination and climate change. Healthy scepticism may have tipped over into a breakdown of trust. There may also be a simple attraction of discussing, holding, and sharing conspiracy theories, especially in youth. Interestingly, those holding conspiracy beliefs could also see greater personal benefits arising from the crisis. There were indications that the coronavirus conspiracy beliefs are more likely to be held by those who perceive themselves as marginalised, but these relationships do not appear as strong as in previous studies (e.g. Freeman & Bentall, Reference Freeman and Bentall2017). This weakening may reflect a cross-over of distrust of mainstream accounts into the mainstream itself. Replications of the survey are required to confirm whether the high prevalence of conspiracy beliefs is accurate. Comparative studies across countries could be extremely informative in establishing the social causes.
There are significant limitations to the survey. Foremost, we used a non-probability online quota sampling method. This will have introduced bias into who was approached to take part. Probability sampling, in which members of the population have an equal chance of participating, produces better estimates. All that we know in this survey is that as a whole the respondents were broadly representative of the adult general population on a number of basic demographic features but not that individual respondents were representative of the general population. The views of those who are not online were not assessed, the level of non-responses to the survey invitation is unknown, and, specifically, it is unknown whether the degree to which conspiracy beliefs are endorsed influenced the decision to take part. The prevalence estimates in this survey need to be treated with caution. It is also unknown whether important coronavirus conspiracy beliefs were overlooked in the item pool or the degree to which self-report of attitudes to coronavirus guidelines is accurate. The cross-sectional nature of the design precludes causal inference. Arguably, the coronavirus concerns could be post hoc rationalisations of not following socially accepted lockdown behaviours. However, we believe it is more likely that conspiracy beliefs drive behaviour or at the very least remove barriers to carrying out unhelpful behaviours. In our view the urgent question now is how can the prevalence and impact of conspiracy beliefs and general mistrust be reduced both in the short and long term?
Acknowledgements
DF is supported by an NIHR Research Professorship (NIHR-RP-2014-05-003). The study was supported by the NHS National Institute of Health Research (NIHR) invention for innovation (i4i) programme (Project II-C7-0117-20001) and the NIHR Oxford Health Biomedical Research Centre (BRC-1215-20005). The views expressed are those of the authors and not necessarily those of the National Health Service, NIHR, or the Department of Health.
Author contributions
DF was the chief investigator and wrote the paper. All authors contributed to the study design. DF and SL carried out the analyses. All authors commented on the paper.
Conflict of interest
Daniel Freeman has written popular science, self-help, and academic books about paranoia with several publishers for which royalties are received. DF reports grants on the topic of paranoia from National Institute for Health Research, Medical Research Council, and Wellcome Trust. Other authors report no competing interests.








 Open access
Open access