



Introduction
Every year up to two million people across the world receive a first diagnosis of schizophrenia (Jongsma et al., Reference Jongsma, Gayer-Anderson, Lasalvia, Quattrone, Mulè and Szöke2018), which remains associated with poor long-term clinical and social outcomes (Morgan et al., Reference Morgan, Lappin, Heslin, Donoghue, Lomas, Reininghaus and Dazzan2014), including higher mortality rates than the general population (Hjorthøj, Stürup, McGrath, & Nordentoft, Reference Hjorthøj, Stürup, McGrath and Nordentoft2017).
In line with this, insight has been consistently linked with outcome in psychosis – greater insight, better outcomes (Lincoln, Lüllmann, & Rief, Reference Lincoln, Lüllmann and Rief2007; Lysaker, Pattison, Leonhardt, Phelps, & Vohs, Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018). Impaired clinical insight (insight thereafter) can be considered as a cardinal feature of psychotic disorders (Carpenter, Strauss, & Bartko, Reference Carpenter, Strauss and Bartko1973), especially schizophrenia (Amador et al., Reference Amador, Flaum, Andreasen, Strauss, Yale, Clark and Gorman1994). The multidimensional model of insight proposed by David (Reference David1990), which included: (i) awareness of having a mental illness, (ii) the ability to recall previous psychotic experiences as abnormal and (iii) treatment compliance, has received much support from research over the last three decades (Amador & David, Reference Amador and David2004; David, Reference David2019; Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018). However, the evidence of that previous treatments targeting insight are effective in schizophrenia spectrum disorders (SSD) is limited, which may have been due to not addressing what appears to underlie poor insight in SSD, namely metacognitive deficits (Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018a; Nair, Palmer, Aleman, & David, Reference Nair, Palmer, Aleman and David2014).
Thus, in 2004 Henry and Ghaemi conducted a systematic review of 13 previous randomized and non-randomized studies (Henry & Ghaemi, Reference Henry and Ghaemi2004) on different types of intervention, such as psychoeducation (PSE), psychoanalytically oriented therapies, cognitive-behavioural therapy (CBT), video recorded self-observation and antipsychotics, for changing insight. These standard treatments targeting the classic symptoms of schizophrenia failed to improve insight, which was a secondary outcome measure in most of the included studies. In 2013 the results from 19 randomized controlled trials (RCTs) on insight, none of which tested metacognitive interventions, were meta-analysed (Pijnenborg, van Donkersgoed, David, & Aleman, Reference Pijnenborg, van Donkersgoed, David and Aleman2013). Although the overall effect size, d = 0.34, was medium and significant, which suggested that insight could be improved following integrative treatments, further subanalyses for specific interventions, namely CBT, PSE and adherence therapy, yielded smaller non-significant effects. Hence, no evidence-based intervention could be recommended for enhancing insight in SSD.
However, as alluded to above, the metacognitive basis of insight, which is supported by recent meta-analytic literature (Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018; Nair et al., Reference Nair, Palmer, Aleman and David2014), may shed some light on this, that is, metacognitively oriented interventions may improve insight. Metacognition may be defined as ‘knowledge and cognition about cognitive phenomena’ (Flavell, Reference Flavell1979, p. 906) or ‘the ability to think of one's and others’ thinking' (Wells & Purdon, Reference Wells and Purdon1999). Patients with SSD have been demonstrated to have poorer metacognitive performance than the general population (Beck, Baruch, Balter, Steer, & Warman, Reference Beck, Baruch, Balter, Steer and Warman2004; Dimaggio & Lysaker, Reference Dimaggio and Lysaker2010), which has been associated with impaired insight in SSD (Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018; Nair et al., Reference Nair, Palmer, Aleman and David2014). Cognitive insight is a core metacognitive domain which refers to the person's ability to evaluate and correct his/her own distorted beliefs and misinterpretations (self-reflectiveness) and the tendency to overconfidence in one's conclusions (self-certainty) (Beck et al., Reference Beck, Baruch, Balter, Steer and Warman2004). Clinical insight therefore represents a different, albeit related, construct from cognitive insight. Moreover, the association between the two has been recently shown to be weaker than previously thought (Van Camp, Sabbe, & Oldenburg, Reference Van Camp, Sabbe and Oldenburg2017). Nevertheless, interventions targeting metacognitive skills, including cognitive insight, should improve clinical insight too, provided clinical insight has a metacognitive basis (Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018; Nair et al., Reference Nair, Palmer, Aleman and David2014), which forms the context for this systematic review and meta-analysis.
Two metacognitive interventions were designed for patients with SSD, namely Metacognitive Training (MCT) (Moritz & Woodward, Reference Moritz and Woodward2007) and Metacognition Reflection and Insight Therapy (MERIT) (Lysaker & Klion, Reference Lysaker and Klion2018). In addition, so-called Metacognitive Therapy was developed by Wells and colleagues (Fisher & Wells, Reference Fisher and Wells2009), which targets the dysfunctional metacognitive belief about thinking, thus contributing to symptom improvement in a range of mental disorders, such as depression, anxiety and obsessive-compulsive disorder, although more recently it has also been applied to psychosis. By focusing on different topics such as attributional style, jumping to conclusions, changing beliefs, empathy, memory, depression and self-esteem and stigma, MCT seeks ‘to sow the seeds of doubt’ (Moritz et al., Reference Moritz, Andreou, Schneider, Wittekind, Menon, Balzan and Woodward2014a) regarding cognitive biases related to delusional ideas. MCT is usually delivered by trained staff to a group of 8–10 patients as 8 weekly, or twice a week, 45–60-minute sessions, although individual MCT is available (Moritz et al., Reference Moritz, Andreou, Schneider, Wittekind, Menon, Balzan and Woodward2014a). The MCT manual can be accessed at no cost at http://www.uke.de/mkt. MERIT is an integrated form of psychotherapy which promotes recovery from psychosis by helping patients to make more constructive narratives about themselves and others so they can set up their own recovery goals through metacognitive tasks more focused on reflection than on cognitive biases (Lysaker & Klion, Reference Lysaker and Klion2018). MERIT takes the form of 24 face-to-face individual 50-minute sessions. This noted, theoretical differences between these three metacognitive interventions can become rather blurred in the clinical setting. Moreover, other non-metacognitive interventions, such as cognitive-behavioural therapy, may actually involve metacognitive processes, although this remains subject to further debate (Moritz & Lysaker, Reference Moritz and Lysaker2018a). Nevertheless, since insight in SSD was demonstrated to have a metacognitive basis (Lysaker et al., Reference Lysaker, Pattison, Leonhardt, Phelps and Vohs2018; Nair et al., Reference Nair, Palmer, Aleman and David2014), both MCT and MERIT should contribute to improving insight.
One systematic review (Moritz et al., Reference Moritz, Andreou, Schneider, Wittekind, Menon, Balzan and Woodward2014a) and four meta-analyses (Eichner & Berna, Reference Eichner and Berna2016; Jiang, Zhang, Zhu, Li, & Li, Reference Jiang, Zhang, Zhu, Li and Li2015; Liu, Tang, Hung, Tsai, & Lin, Reference Liu, Tang, Hung, Tsai and Lin2018; Philipp et al., Reference Philipp, Kriston, Lanio, Kühne, Härter, Moritz and Meister2019) demonstrated MCT to improve positive psychotic symptoms, although a 2016 meta-analysis failed to replicate this (van Oosterhout et al., Reference van Oosterhout, Smit, Krabbendam, Castelein, Staring and van der Gaag2016a). In a later reply letter from the meta-analysis' authors (van Oosterhout et al., Reference van Oosterhout, Smit, Krabbendam, Castelein, Staring and van der Gaag2016b) the inclusion of four additional studies (Aghotor, Pfueller, Moritz, Weisbrod, & Roesch-Ely, Reference Aghotor, Pfueller, Moritz, Weisbrod and Roesch-Ely2010; Gawęda, Krężołek, Olbryś, Turska, & Kokoszka, Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015; Moritz et al., Reference Moritz, Kerstan, Veckenstedt, Randjbar, Vitzthum, Schmidt and Woodward2011a; So et al., Reference So, Chan, Chong, Wong, Lo, Chung and Chan2015) in the meta-analysis (van Oosterhout et al., Reference van Oosterhout, Smit, Krabbendam, Castelein, Staring and van der Gaag2016a) made the effects of MCT on positive symptoms (g = 0.32) and delusions (g = 0.31), although not on data gathering bias, become significant (van Oosterthout et al., Reference van Oosterhout, Smit, Krabbendam, Castelein, Staring and van der Gaag2016b). No systematic reviews or meta-analyses of MERIT trials have been conducted to date. Most importantly, whether these metacognitive interventions may contribute to gaining insight remains unknown (David, Reference David2019) since conflicting results from previous RCTs reporting insight data, which are detailed below, have not been subject to systematic review or meta-analysis to date.
We carried out a new systematic review and a meta-analysis of previous RCTs to investigate the effect of MCT and MERIT on clinical and cognitive insight (as co-primary outcome measures) in patients with SSD. We hypothesized: (i) that MCT and MERIT will improve clinical and cognitive insight compared with the control intervention; (ii) that the effect size of MCT and MERIT on clinical and cognitive insight changes at follow-up will be larger than immediately after treatment, thus replicating previous findings of longer-term ‘sleeper’ effects of MCT on delusions (Moritz et al., Reference Moritz, Veckenstedt, Andreou, Bohn, Hottenrott, Leighton and Roesch-Ely2014b).
Methods
This systematic review and meta-analysis complied with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, Reference Moher, Liberati, Tetzlaff and Altman2009).
Search strategy
We conducted a literature search in PubMed, PsycInfo and Embase of articles that reported the effects of MCT and MERIT on clinical and/or cognitive insight in samples of patients with SSD from January 2007, when MCT became available (MERIT was developed in 2014), to June 2019. The search strategy used Medical Subjects Headings (MeSH) terms and keywords (‘metacog*’, ‘MCT’, ‘MERIT,’ ‘insight*,’ ‘awareness*,’ and ‘consciousness*’, ‘schizophr*,’ ‘psychos*,’ ‘psychot*,’ ‘illness*,’), including cross-referencing. The only initial search limitation was by English language. References from selected articles were cross-reviewed and selected if they met the following criteria and were indexed into PubMed, PsycInfo or Embase.
Selection criteria
All the abstracts from the initial search were independently screened by JDLM and OA against the following selection criteria. Any doubt about meeting/not meeting the selection criteria was resolved by reviewing the full article:
• Sample size of more than 10 patients;
• Age: 16–64 years;
• Diagnosis: ‘Schizophrenia spectrum disorders’ (SSD) encompassing schizophrenia, schizoaffective disorder, delusional disorder and psychotic disorder Not Otherwise Specified, according to either International Statistical Classification of Diseases (ICD), 10th Revision (World Health Organization, 1993), or Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) and Fourth Edition Text Revision (DSM-IV-TR) definitions (American Psychiatric Association, 2000); or first-episode psychosis (FEP) according to the DSM-IV-TR criteria (American Psychiatric Association, 2000). In terms of diagnosis as a selection criterion, we decided to use a broader category, such as SSD, in order to include all the trials testing MCT or MERIT in samples of patients with any non-affective psychotic disorder, thus aiming to answer the research question formulated above. Although the inclusion of a tiny proportion of patients with bipolar disorder (or affective psychosis) cannot be ruled out, particularly in first episode or early onset psychosis trials (e.g. Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017), based on the aims of the included studies and reported samples characteristics this seems very unlikely.
• Outcome measures:
-
o Clinical Insight had to be assessed before and after treatment with a validated instrument which, based on the search, included the Insight and Treatment Attitudes Questionnaire (ITAQ) (McEvoy et al., Reference McEvoy, Freter, Everett, Geller, Appelbaum, Apperson and Roth1989), the Schedule for Assessment of Insight, expanded version (SAI-E) (Kemp & David, Reference Kemp, David and Blackwell1997), the Scale to assess Unawareness of Mental Disorders (SUMD) (Amador et al., Reference Amador, Strauss, Yale, Flaum, Endicott and Gorman1993), the Birchwood Insight Scale (BIS) (Birchwood et al., Reference Birchwood, Smith, Drury, Healy, Macmillan and Slade1994), the general item 12 of the Positive and Negative Syndrome Scale (PANSS) (Kay, Fiszbein, & Opler, Reference Kay, Fiszbein and Opler1987) and a unidimensional insight questionnaire (Kokoszka, Telichowska-Leśna, & Radzio, Reference Kokoszka, Telichowska-Leśna and Radzio2008) used in one trial (Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015);
-
o Cognitive Insight had to be measured before and after treatment with the Beck Cognitive Insight Scale (BCIS) (Beck et al., Reference Beck, Baruch, Balter, Steer and Warman2004);
-
• Clinical setting: In-, out-patients and mixed samples were included;
• In case of replication studies by the same group, only the latest one with the largest sample size was considered;
• Only RCT were included regardless of the masking (double-, single-blind or unblind).
Statistical analysis
Individual effect sizes (Cohen's d) for control and intervention conditions of each RCT were calculated with reported means and standard deviations using the effect size calculation software developed by Wilson (Reference Wilson2010). Subsequently, the effect size of the control condition was subtracted from the effect size of the intervention, resulting in one effect size for each study (Morris & DeShon, Reference Morris and DeShon2002).
Meta-analyses were performed with the program Review Manager 5.0, developed by the Cochrane Collaboration. Effect sizes were weighted by their standard error. Based on the reported means and standard deviations of insight scores before- and after-treatment (Lipsey & Wilson, Reference Lipsey and Wilson2001), between-group differences in cognitive and clinical insight were calculated at three timepoints (at baseline, at post-treatment and at follow-up) using a random-effects model (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2010), which was chosen to account for the influence of the differences in interventions received across the study groups. Because of the variance in the type of interventions, a random-effects model was used. The overall effect size was calculated and represented in a forest plot together with the effect size of each study.
We adjusted for the presence of any publication bias using the Duval and Tweedie ‘trim-and-fill’ method (Duval & Tweedie, Reference Duval and Tweedie2000). Heterogeneity was measured with the Q statistic yielding a chi-square and p-value and the I2 statistic with scores above 50% and 75% indicating moderate and high heterogeneity, respectively (Higgins, Thompson, Deeks, & Altman, Reference Higgins, Thompson, Deeks and Altman2003). The summary statistics were illustrated with forest and funnel plots. Forest plots provide an indication of heterogeneity between studies (Phan, Xie, Di Eusanio, & Yan, Reference Phan, Xie, Di Eusanio and Yan2014); while the funnel plot is utilized to detect and illustrate publication bias (Duval & Tweedie, Reference Duval and Tweedie2000b). Statistical significance was set at p ⩽ 0.05.
Results
The initial search yielded 189 references. Eight more records were retrieved from the grey literature, although none of them fulfilled the above selection criteria. Hence, 197 records were screened at an abstract level. In total, 168 of these articles were excluded based on our selection criteria. Twenty-nine articles were assessed for eligibility so the full text was reviewed. Seventeen articles were excluded as follows: 11 articles did not report on insight measures (Aghotor et al., Reference Aghotor, Pfueller, Moritz, Weisbrod and Roesch-Ely2010; Buonocore et al., Reference Buonocore, Bosia, Riccaboni, Bechi, Spangaro, Piantanida and Cavallaro2015; Erawati, Keliat, Helena, & Hamid, Reference Erawati, Keliat, Helena and Hamid2014; Kumar et al., Reference Kumar, Rao, Raveendranathan, Venkatasubramanian, Varambally and Gangadhar2015; Moritz et al., Reference Moritz, Kerstan, Veckenstedt, Randjbar, Vitzthum, Schmidt and Woodward2011a, Reference Moritz, Veckenstedt, Randjbar, Vitzthum and Woodward2011b, Reference Moritz, Veckenstedt, Bohn, Hottenrott, Scheu, Randjbar and Roesch-Ely2013, Reference Moritz, Veckenstedt, Andreou, Bohn, Hottenrott, Leighton and Roesch-Ely2014b; Naughton et al., Reference Naughton, Nulty, Abidin, Davoren, O'Dwyer and Kennedy2012; Ross, Freeman, Dunn, & Garety, Reference Ross, Freeman, Dunn and Garety2011; So et al., Reference So, Chan, Chong, Wong, Lo, Chung and Chan2015) and 3 articles did not have a RCT design (Balzan, Delfabbro, Galletly, & Woodward, Reference Balzan, Delfabbro, Galletly and Woodward2014; Favrod, Maire, Bardy, Pernier, & Bonsack, Reference Favrod, Maire, Bardy, Pernier and Bonsack2011; Ussorio et al., Reference Ussorio, Giusti, Wittekind, Bianchini, Malavolta, Pollice and Roncone2016). One study used an overlapping sample (Moritz et al., Reference Moritz, Mahlke, Westermann, Ruppelt, Lysaker, Bock and Andreou2018b) and 2 trials tested other metacognitive interventions such as ‘metacognition and social cognition training’ (MSCT) (Rocha & Queirós, Reference Rocha and Queirós2013) and the so-called REFLEX (Pijnenborg et al., Reference Pijnenborg, de Vos, Timmerman, Van der Gaag, Sportel, Arends and Aleman2019), both of which are briefly described below. Hence, 12 articles fulfilled the selection criteria, so were included in the systematic review and meta-analysis, which totalled n = 807 participants. Of these, n = 713 individuals (83.3%) received the allocated interventions and completed the post-treatment assessment, at which attrition rates ranged from 0% (Balzan, Mattiske, Delfabbro, Liu, & Galletly, Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Kuokkanen, Lappalainen, Repo-Tiihonen, & Tiihonen, Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014) to 27% (Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017). Seven studies followed-up participants over 6 months (Andreou et al., Reference Andreou, Wittekind, Fieker, Heitz, Veckenstedt, Bohn and Moritz2017; Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; de Jong et al., Reference de Jong, van Donkersgoed, Timmerman, Aan Het Rot, Wunderink, Arends and Pijnenborg2019; Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014; Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014; Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017; van Oosterhout et al., Reference van Oosterhout, Krabbendam, de Boer, Ferwerda, van der Helm, Stant and van der Gaag2014). Attrition rates over the 6-month follow-up period ranged from 1% (Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014) to 41.4% (de Jong et al., Reference de Jong, van Donkersgoed, Timmerman, Aan Het Rot, Wunderink, Arends and Pijnenborg2019). The flow chart in Fig. 1 shows the studies selection process and Table 1 provides full details of included studies.

Fig. 1. Flow chart of the studies selection process.
Table 1. Description of the selected studies

Ni, initial sample size; NPT, sample size at post-treatment; PT, post-treatment; FU, follow-up; SSD, schizophrenia spectrum disorder; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, fourth edition; DMS-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revised; E, experimental; C, Control; G-MCT, Group metacognitive training; I-MCT, individual metacognitive training; TAU, treatment as usual; BCIS, Beck Cognitive Insight Scale (Beck et al., Reference Beck, Baruch, Balter, Steer and Warman2004); SR, Self-Reflectiveness; SC, self-certainty; CI, Composite Index; MINI, Mini International Neuropsychiatric Interview (Sheehan et al., Reference Sheehan, Lecrubier, Sheehan, Amorim, Janavs, Weiller and Dunbar1998); SAI, Schedule for Assessment of Insight (Kemp and David, Reference Kemp, David and Blackwell1997); PANSS, The Positive and Negative Syndrome Scale (Kay et al., Reference Kay, Fiszbein and Opler1987); SUMD, Scale to assess Unawareness of Mental Disorder (Amador et al., Reference Amador, Strauss, Yale, Flaum, Endicott and Gorman1993); MERIT, Metacognitive Reflection and Insight Therapy; ICD −10, 10th revision of the International Statistical Classification of Diseases (ICD).
Ten studies used MCT in samples of patients with SSD (total N = 717 participants). These were divided into six articles on cognitive insight, which were meta-analysed, and five articles with non-meta-analysable data on clinical insight, including one MCT trial reporting clinical and cognitive insight results (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019). Owing to the use of different insight assessment scales (in some studies insight was measured in a unidimensional manner, while in others multidimensional scales were used) and the lack of consistent quantitative data needed, a meta-analysis of clinical insight RCTs was not feasible. As an alternative, we conducted a narrative review of the findings from the selected studies.
MCT and cognitive insight
Six studies reported on the effects of MCT on cognitive insight, that is, BCIS scores (Ahuir et al., Reference Ahuir, Cabezas, Miñano, Algora, Estrada, Solé and Labad2018; Andreou et al., Reference Andreou, Wittekind, Fieker, Heitz, Veckenstedt, Bohn and Moritz2017; Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Lam et al., Reference Lam, Ho, Wa, Chan, Yam, Yeung and Balzan2015; Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017; van Oosterhout et al., Reference van Oosterhout, Krabbendam, de Boer, Ferwerda, van der Helm, Stant and van der Gaag2014). Full details are provided in Table 1. Sample sizes ranged from n = 28 (Ahuir et al., Reference Ahuir, Cabezas, Miñano, Algora, Estrada, Solé and Labad2018) to n = 154 (van Oosterhout et al., Reference van Oosterhout, Krabbendam, de Boer, Ferwerda, van der Helm, Stant and van der Gaag2014), totalling N = 443 participants. Details of the meta-analytic results of these six studies, including heterogeneity and publication bias, are provided in Table TS1 of the online Supplementary Material. A visual inspection of the funnel plots (online supplementary Figures FS1, FS2, FS3, FS4, FS5, FS6, FS7, FS8 and FS9) revealed some asymmetry so we adjusted for potential missing studies, although this did not alter the results below.
The overall effect on self-reflectiveness (higher self-reflectiveness score, greater cognitive insight), which was not observed at baseline, d = 0.20, 95% CI −0.18 to 0.58, Z = 1.02, p = 0.31, favoured MCT compared with controls both at post-treatment, d = 0.46, 95% CI 0.21–0.71, Z = 3.64, p < 0.01, and, at a lesser level, at follow-up, d = 0.30, 95% CI 0.08–0.51, Z = 2.70, p < 0.01. There was no evidence of heterogeneity at post-treatment, I2 = 38%, p = 0.16, or at follow-up, I2 = 0%, p = 0.49 (Fig. 2).
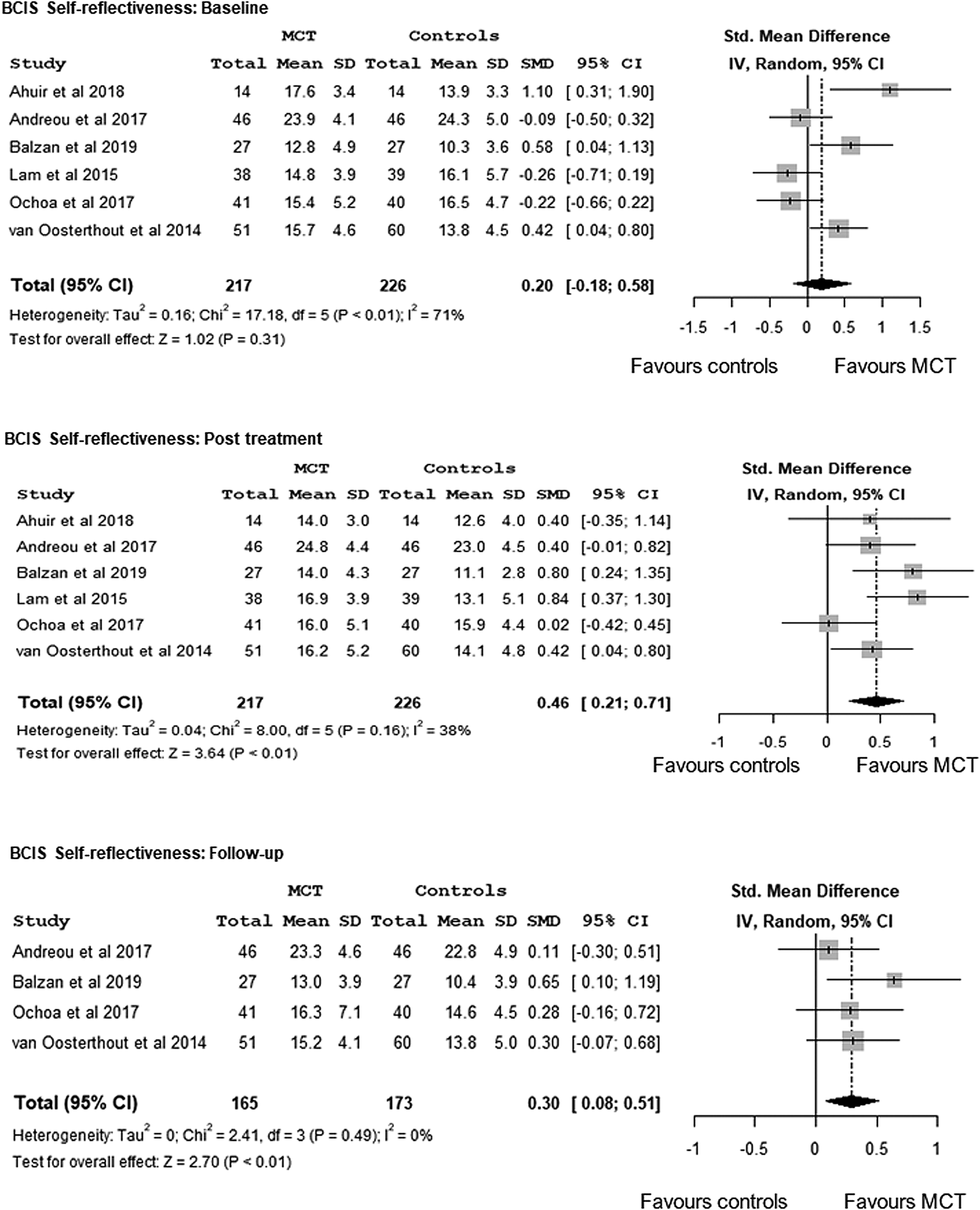
Fig. 2. Meta-analysis of the effects of Metacognitive Training on cognitive insight - BCIS-Self-Reflectiveness -: at baseline, at post-treatment and at a follow-up.
In terms of self-certainty (lower self-certainty score indicating greater cognitive insight), while baseline between-group differences were non-significant, d = −0.13, 95% CI −0.34 to 0.09, Z = −1.16, p = 0.24, meta-analysis showed MCT to be superior to the control condition at post-treatment at a significant small effect size, d = −0.23, 95% CI −0.44 to −0.02, Z = −2.14, p = 0.03, but not at follow-up, d = 0.01, 95% CI −0.20 to 0.22, Z = 0.10, p = 0.92. No evidence of heterogeneity was found at post-treatment, I2 = 23%, p = 0.26 or at follow-up, I2 = 0%, p = 0.75 (Fig. 3).

Fig. 3. Meta-analysis of the effects of Metacognitive Training on cognitive insight - BCIS-Self-Certainty -: at baseline, at post-treatment and at follow-up.
Although only three studies reported on Composite Index (higher Composite Index score, greater insight) (Ahuir et al., Reference Ahuir, Cabezas, Miñano, Algora, Estrada, Solé and Labad2018; Lam et al., Reference Lam, Ho, Wa, Chan, Yam, Yeung and Balzan2015; Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017), based on the self-reflectiveness and self-certainty scores, we calculated the Composite Index for the remaining three studies (Andreou et al., Reference Andreou, Wittekind, Fieker, Heitz, Veckenstedt, Bohn and Moritz2017; Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; van Oosterhout et al., Reference van Oosterhout, Krabbendam, de Boer, Ferwerda, van der Helm, Stant and van der Gaag2014). There were baseline differences between treatment-arms favouring MCT v. controls, d = 0.67, 95% CI 0.04–1.31, Z = 2.09, p = 0.04. Post-treatment meta-analysis revealed a large effect, d = 1.11, 95% CI 0.28–1.93, Z = 2.64, p < 0.01, and evidence of heterogeneity, I2 = 90.0%, p < 0.01. Based on four follow-up trials (Andreou et al., Reference Andreou, Wittekind, Fieker, Heitz, Veckenstedt, Bohn and Moritz2017; Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017; van Oosterhout et al., Reference van Oosterhout, Krabbendam, de Boer, Ferwerda, van der Helm, Stant and van der Gaag2014), the meta-analysis favoured MCT over controls, d = 0.86, 95% CI 0.08–1.63, Z = 2.17, p = 0.03, although we found evidence of heterogeneity, I2 = 89.0%, p < 0.01 (Fig. 4).

Fig. 4. Meta-analysis of the effects of Metacognitive Training on cognitive insight - BCISComposite Index -: at baseline, at post-treatment and at follow-up.
MCT and clinical insight
Five RCTs (N = 244) reported on the effects of MCT on clinical insight (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014; Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014; Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015; Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014), including one RCT on both cognitive and clinical insight (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019). Out of these five trials, four of them favoured MCT.
First, from a multidimensional approach to insight measured with the SUMD, a 6-month follow-up RCT from France found that group MCT [compared with treatment as usual (TAU)] was effective in helping patients gain insight. Specifically, awareness of delusions improved in the MCT group (compared with controls) both at post-treatment and at 6-month follow-up with a significant medium-large effect size, d = 0.51 and d = 0.56, respectively, although differences in the attribution of delusions were non-significant (Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014). In line with this, the results from a trial with a sample of n = 68 SSD patients (Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014) favoured group MCT compared to a control condition of supportive therapy in terms of awareness of hallucinations with small effect size, F (1.46,3.75), p = 0.058, r = −0.25, although this was not replicated by other SUMD scores. A trial in which insight was assessed unidimensionally with the Kokozska et al.'s insight questionnaire (Kokoszka et al., Reference Kokoszka, Telichowska-Leśna and Radzio2008) in n = 52 SSD outpatients revealed a large effect size increase in insight, d = 0.98, in the MCT group compared with TAU (Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015).
More recently, individual MCT was compared with an active control intervention, namely cognitive remediation, in a cohort of n = 56 schizophrenia patients, who were followed-up over 6 months (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019). Total insight scores, which were measured with the SAI, increased significantly from baseline to post-treatment in both treatment arms, with a larger effect size for MCT, d = 0.70, compared with controls, d = 0.29. From post-treatment to follow-up, total insight scores decreased in both groups, although this was only significant in the control group. The Group × Time interaction for total insight scores based on the ANOVA model, although statistically significant, p = 0.009, yielded a small effect size, ŋ2 = 0.07 (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019).
However, a 6-month follow-up trial testing group MCT against TAU in n = 20 forensic patients with schizophrenia failed to find between-group differences in terms of clinical insight gain evaluated with the single PANSS item (Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014).
Metacognitive reflection and insight therapy
The first MERIT trial (Vohs et al., Reference Vohs, Leonhardt, James, Francis, Breier, Mehdiyoun and Lysaker2018) recruited n = 20 early psychosis patients who were randomized to either MERIT or TAU. Insight was assessed with the SUMD before and after treatment. There were between-group differences in clinical insight improvement favouring MERIT at a medium effect size, F (1,16) = 11.5, p < 0.001, pη2 = 0.4. A larger 6-month follow-up trial (n = 70), however, failed to replicate this positive effect of MERIT on cognitive insight compared with TAU (de Jong et al., Reference de Jong, van Donkersgoed, Timmerman, Aan Het Rot, Wunderink, Arends and Pijnenborg2019).
Discussion
Main findings
We carried out a systematic review and meta-analysis of RCTs testing the effects of two metacognitive interventions designed for patients with SSD, namely MCT and MERIT, on insight changes, from which two main conclusions can be drawn. First, in line with our first hypothesis, MCT was found to improve cognitive insight, particularly self-reflectiveness, which was also supported by meta-analytic results, and two clinical insight dimensions, such as illness awareness and awareness of some psychotic phenomena, including delusions and hallucinations. However, somewhat in contrast to our expectations (hypothesis i), this was not replicated by the two MERIT trials. Second, our results showed that the effects of MCT and MERIT on insight were larger at post-treatment than at follow-up, which conflicted our hypothesis ii. We also noted relevant between-study methodological differences, which did not permit us to apply meta-analytic techniques to the clinical insight trials.
Metacognitive interventions and cognitive insight
Cognitive insight measured by a 15-item self-rated scale (BCIS) has two factors, namely self-reflectiveness and self-certainty (Beck et al., Reference Beck, Baruch, Balter, Steer and Warman2004). Patients with psychotic disorders were reported to have lower self-reflectiveness and higher self-confidence than the general population (Beck et al., Reference Beck, Baruch, Balter, Steer and Warman2004). Hence, interventions aim to increase self-reflectiveness and to decrease self-certainty. In this regard, all the selected trials reporting self-reflectiveness data found MCT to be superior to a control condition, according to our meta-analysis. Hence, it seems that MCT does improve patient's ability to reflect on his/her own thoughts and to correct interpretations based on contradictory evidence and/or external feedback, particularly shortly after treatment. Longer-term trials are needed to establish whether this cognitive insight improvement is maintained over time. As alluded to above, SSD patients have a tendency to overconfidence in their beliefs, which is known as self-certainty. Our meta-analysis revealed MCT to reduce patients' self-certainty after treatment, while this effect was not observed at follow-up. In keeping with this, a reanalysis (Köther et al., Reference Köther, Veckenstedt, Vitzthum, Roesch-Ely, Pfueller, Scheu and Moritz2012) of data from an included RCT (Moritz et al., Reference Moritz, Veckenstedt, Bohn, Hottenrott, Scheu, Randjbar and Roesch-Ely2013) revealed MCT (when compared with cognitive remediation-CogPack®) to reduce the amount of overconfidence ratings (which ranged from 1, i.e. ‘100% sure’, to 4, i.e. ‘100% uncertain’) of mental state perceptions assessed with the Reading the Mind in the Eyes test (Baron-Cohen, Wheelwright, Hill, Raste, & Plumb, Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb2001). Consistent with this, the three selected trials using an overall measure of cognitive insight, the BCIS Composite Index score, favoured MCT over TAU (Lam et al., Reference Lam, Ho, Wa, Chan, Yam, Yeung and Balzan2015) or PSE (Ahuir et al., Reference Ahuir, Cabezas, Miñano, Algora, Estrada, Solé and Labad2018; Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017).
Only one trial reported on both cognitive and clinical insight (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019), which linked MCT-related cognitive insight improvement with better clinical insight. Of note, controls received an active intervention, namely cognitive remediation. Hence, this trial, although awaiting replication studies, showed MCT to be superior to cognitive remediation in increasing cognitive and clinical insight levels.
In summary, our meta-analytic results on cognitive insight appear to provide sufficient evidence to recommend MCT as a cognitive insight improving intervention for patients with SSD, particularly in terms of increasing self-reflectiveness, while we could not observe such a relevant effect on self-certainty, particularly in the long-term. Two non-mutually exclusive explanations may have contributed to this finding. First, while MCT does seem to enhance patient's ability to reflect on his/her own thoughts, particularly in terms of receiving and accepting external feedback, this intervention may fail to make patients become less (over)-confident in their own conclusions. In other words, MCT may be more helpful in improving cognitive insight based on external feedback (i.e. others-based cognitive insight), while confidence in one's thoughts, which is, of course, a more internal process, may be less prone to such an intervention (i.e. oneself-based cognitive insight). Second, it could be argued that the impact of MCT on self-certainty, which was supported by a significant small effect size at post-treatment but not at follow-up, may require maintenance MCT sessions. In this regard, a MCT-based smartphone application has recently become available (https://clinical-neuropsychology.de/app_en), which showed promising results in terms of feasibility and efficacy for depressive symptoms (Lüdtke, Pult, Schröder, Moritz, & Bücker, Reference Lüdtke, Pult, Schröder, Moritz and Bücker2018). In addition, the extent to which this cognitive insight improvement results in better clinical insight and outcomes in the longer-term, which is what really matters since SSD tend to be chronic, remains to be established.
Our results, however, went against our second hypothesis, that is, we failed to find larger effects of MCT on insight in the longer-term than immediately after treatment. This said, the RCT behind this postulation (Moritz et al., Reference Moritz, Veckenstedt, Andreou, Bohn, Hottenrott, Leighton and Roesch-Ely2014b) revealed the so-called ‘sleeper’ effects of MCT on delusions at 3 years, while the longest follow-up period of the trials included in our review was 6 months. Hence, sustained effects of MCT on insight in the (very) long-term cannot be ruled out despite our negative results. On the other hand, the only RCT testing the effect of MERIT on cognitive insight (de Jong et al., Reference de Jong, van Donkersgoed, Timmerman, Aan Het Rot, Wunderink, Arends and Pijnenborg2019) failed to find this in comparison to TAU, which warrants further investigation. As discussed further below, MERIT seems to improve patient's ability to make narrative judgements about concepts such as mental illness and recovery, that is, MERIT may be more helpful in tackling clinical insight rather than cognitive insight.
Metacognitive interventions and clinical insight
We identified five MCT trials on clinical insight (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014; Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014; Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015; Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014), four of which (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014; Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014; Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015) favoured MCT. Of note, three of these trials (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014; Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014) measured insight with multidimensional scales, consistently with the multidimensional model of insight (Amador & David, Reference Amador and David2004; David, Reference David1990; Lysaker & Klion, Reference Lysaker and Klion2018). MCT may thus affect clinical insight dimensions differently. For instance, one trial found MCT to improve illness awareness in comparison to cognitive remediation after treatment, although no significant between-group differences were observed at 6-month follow-up (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019). This raises issues about the extent to which the gain in awareness of having an illness was an actual response to MCT or the consequence of psychotic symptoms remission. Also, this trial (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019) used individual MCT. Hence, participants, who consented to an intensive face-to-face intervention, may have had higher baseline insight levels than those who refused to take part in the trial, thus introducing a selection bias. Indeed, the two trials testing individual MCT (Andreou et al., Reference Andreou, Wittekind, Fieker, Heitz, Veckenstedt, Bohn and Moritz2017; Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019) reported much higher BCIS scores than the other studies, all of which used group MCT. Nevertheless, future trials should properly investigate differences in outcomes, including insight, between both MCT approaches.
The other two trials using a multidimensional insight scale, such as the SUMD, reported MCT to increase insight into psychotic symptoms, such as delusions (Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014) and hallucinations (Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014). Also, this positive impact of MCT on clinical insight was replicated by another trial (Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015) in terms of illness awareness gain, although MCT was compared with TAU and outcomes were only measured after treatment by means of a less widely used insight scale (Kokoszka et al., Reference Kokoszka, Telichowska-Leśna and Radzio2008). On the other hand, one small (n = 20) trial (Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014) failed to replicate this, which may have been due to insufficient statistical power and/or measuring insight in a unidimensional manner through the PANSS item. Another potentially unpowered (n = 20) RCT failed to show that MERIT improved clinical insight (Vohs et al., Reference Vohs, Leonhardt, James, Francis, Breier, Mehdiyoun and Lysaker2018). However, given the lack of follow-up data potential longer-term benefits from MERIT in terms of clinical insight gain cannot be ruled out.
In summary, four out of five trials found MCT to positively affect clinical insight in comparison to TAU (Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014; Gawęda et al., Reference Gawęda, Krężołek, Olbryś, Turska and Kokoszka2015) or some control interventions, such as cognitive remediation (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019) or supportive therapy (Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014). However, at 6-month follow-up, only one trial reported improvements in delusion awareness as a result of receiving MCT (Favrod et al., Reference Favrod, Rexhaj, Bardy, Ferrari, Hayoz, Moritz and Bonsack2014). These intensive metacognitive interventions, particularly individual MCT (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019) and MERIT (Vohs et al., Reference Vohs, Leonhardt, James, Francis, Breier, Mehdiyoun and Lysaker2018), appear to make patients gain awareness of mental illness and symptoms. However, further trials are warranted to establish whether delivering these interventions as maintenance treatment may contribute to sustaining this insight improvement in the long-term.
Overall drop-out rates were very low, ranging from 0% (Balzan et al., Reference Balzan, Mattiske, Delfabbro, Liu and Galletly2019; Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014) to 27% (Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017) at post-treatment and from 1% (Kuokkanen et al., Reference Kuokkanen, Lappalainen, Repo-Tiihonen and Tiihonen2014) to 41.4% (de Jong et al., Reference de Jong, van Donkersgoed, Timmerman, Aan Het Rot, Wunderink, Arends and Pijnenborg2019) at 6-month follow-up. This may reflect the high levels of participants' satisfaction with MCT, in line with previous studies [e.g. (Moritz et al., Reference Moritz, Veckenstedt, Andreou, Bohn, Hottenrott, Leighton and Roesch-Ely2014b)], including a meta-analysis (Eichner & Berna, Reference Eichner and Berna2016). In addition, the high attendance rates may be the result of a therapeutic effect of MCT on attendees. However, a potential selection bias cannot be ruled out since participants tend to be more compliant than those who refuse to enrol research studies, particularly RCTs.
Other non-included metacognitive interventions
As shown in Fig. 1, we identified n = 17 studies which, although reporting on metacognition-based interventions and insight, did not meet our selection criteria (Aghotor et al., Reference Aghotor, Pfueller, Moritz, Weisbrod and Roesch-Ely2010; Balzan et al., Reference Balzan, Delfabbro, Galletly and Woodward2014; Buonocore et al., Reference Buonocore, Bosia, Riccaboni, Bechi, Spangaro, Piantanida and Cavallaro2015; Erawati et al., Reference Erawati, Keliat, Helena and Hamid2014; Favrod et al., Reference Favrod, Maire, Bardy, Pernier and Bonsack2011; Kumar et al., Reference Kumar, Rao, Raveendranathan, Venkatasubramanian, Varambally and Gangadhar2015; Moritz et al., Reference Moritz, Kerstan, Veckenstedt, Randjbar, Vitzthum, Schmidt and Woodward2011a, Reference Moritz, Veckenstedt, Randjbar, Vitzthum and Woodward2011b, Reference Moritz, Veckenstedt, Bohn, Hottenrott, Scheu, Randjbar and Roesch-Ely2013, Reference Moritz, Veckenstedt, Andreou, Bohn, Hottenrott, Leighton and Roesch-Ely2014b; Reference Moritz, Mahlke, Westermann, Ruppelt, Lysaker, Bock and Andreou2018; Naughton et al., Reference Naughton, Nulty, Abidin, Davoren, O'Dwyer and Kennedy2012; Pijnenborg et al., Reference Pijnenborg, de Vos, Timmerman, Van der Gaag, Sportel, Arends and Aleman2019; Rocha & Queirós, Reference Rocha and Queirós2013; Ross et al., Reference Ross, Freeman, Dunn and Garety2011; So et al., Reference So, Chan, Chong, Wong, Lo, Chung and Chan2015; Ussorio et al., Reference Ussorio, Giusti, Wittekind, Bianchini, Malavolta, Pollice and Roncone2016). Overall, these trials support the use of metacognitive interventions for enhancing insight. Of note, a metacognition-based intervention called REFLEX was showed to improve insight-related aspects such as internalized stigma (Pijnenborg et al., Reference Pijnenborg, de Vos, Timmerman, Van der Gaag, Sportel, Arends and Aleman2019).
Limitations
We searched three major databases, such as PubMed, PsycInfo and EMBASE, and we retrieved n = 8 papers from the grey literature. However, the search was limited to English language papers and the selection criteria may have been too restrictive, particularly regarding insight scales. Hence, this review may not include all the metacognitive interventions-based trials reporting insight data, especially those in the very grey literature outside PubMed, PsycInfo and EMBASE. Also, the clinical insight studies' results could not be meta-analysed for reasons given above. In addition, it should be noted that the MCT modules on self-esteem and stigma were not available in the original manual of MCT, although the selected trials did not specify this. As a result, we could not investigate whether these two additional modules may have a larger effect on insight compared with the original MCT manual. With regard to the cognitive insight studies, two issues need to be considered. First, the BCIS is a self-report, hence ratings may have been affected by the degree of cooperation and motivation, which tends to be low in subjects with limited insight; and some caution is therefore needed when interpreting BCIS results. Second, cognitive insight was a secondary outcome in most of the included studies, which may also explain why the composite index was only reported in three selected trials. Finally, this was a systematic review and meta-analysis of RCTs, most of which were part of larger research projects, which were not focused on insight. As a result, the comprehensiveness and duration of the studies assessments may have contributed to increasing insight themselves, in addition to the potential selection bias due to being a participant in a RCT, that is, giving consent to such a lengthy protocol, which included two or three face-to-face interviews.
Clinical relevance and implications for future research
This systematic review therefore adds to the field, namely treatments for lack of insight in SSD, which is of major clinical relevance given the association of insight with outcomes. In particular, one previous systematic review (Henry & Ghaemi, Reference Henry and Ghaemi2004) and a meta-analysis (Pijnenborg et al., Reference Pijnenborg, van Donkersgoed, David and Aleman2013) reported small effects of previous treatments for insight in psychosis, although metacognitive interventions were unavailable at that time. Hence, our systematic review and meta-analysis would provide support for delivering metacognitive interventions, particularly MCT, in clinical settings managing psychosis patients to improve insight.
Future trials should include clinical and social outcomes measures other than psychotic symptoms, such as readmissions, suicidal behaviour and psychosocial functioning, including self-appraisal of quality of life. Larger sample sizes and longer follow-up periods are required to examine rare outcomes. Multidimensional insight scales should be used since the impact of metacognitive interventions on individual insight dimensions may differ, which may also change over time. Future trials should also compare individual with group interventions, including cost-effectiveness investigations. With regard to the control group, instead of TAU, in which case between-group differences in insight changes may be attributed to the effect of attending a weekly group rather than to the metacognitive intervention, controls should receive an active intervention such as PSE (Ochoa et al., Reference Ochoa, López-Carrilero, Barrigón, Pousa, Barajas and Lorente-Rovira2017) or supportive therapy (Briki et al., Reference Briki, Monnin, Haffen, Sechter, Favrod, Netillard and Vandel2014). Indeed, this is the question that clinicians intend to answer, i.e., ‘Which intervention should I put my patient on (for improving insight)?’, while no intervention (i.e. TAU) does not tend to be considered an option. In line with this, only five out of the twelve selected trials used an active control intervention (see Table 1 for details), which may limit, to some degree, the apparent benefits from MCT and MERIT to enhance insight.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291720003384
Acknowledgements
We are very grateful to our colleagues from the Department of Psychiatry of Hospital Universitario Fundación Jiménez Díaz, who are too numerous to mention by name, for their helpful comments on earlier versions of this manuscript. J.D.L.M. acknowledges funding support from the Universidad Autónoma de Madrid and European Union-European Commission via the 2019–2021 Intertalentum Project & Marie Skłodowska-Curie Actions Grant (GA 713366). O.A. is further funded by the National Institute for Health Research (NIHR) (NIHR Post-Doctoral Fellowship - PDF-2018-11-ST2-020). The views expressed in this publication are those of the authors and not necessarily those of the Spanish National Health Service, the United Kingdom National Health Service (NHS), the National Institute for Health Research or the Department of Health and Social Care.
Conflict of interest
J.D.L.M. has lectured for Janssen and Otsuka Pharmaceuticals and A.S.D. has received honoraria from Janssen and Roche Pharmaceuticals. The other authors have no conflict of interest to declare.








 Open access
Open access